|
Ms Catherine Collins - Dept of Nutrition and Dietetics
- St Georges Hospital
- London
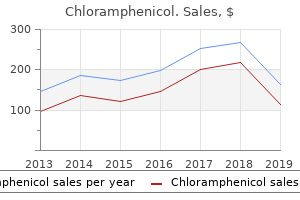
Chloramphenicol dosages: 500 mg, 250 mg
Chloramphenicol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Generic chloramphenicol 250 mg without a prescriptionAcute or subacute sensorineural hearing impairment was reported in lower than 5% of clinically evident circumstances of mumps virus your computer has been locked 250 mg chloramphenicol with amex, though it may happen following subclinical an infection. High-frequency listening to impairment from mumps infection is usually transient, and bilateral in nature. Current literature suggests that vaccinated circumstances present with lower issues, and after they do happen, extreme problems are reported in adults greater than kids. The clinical presentation, symptoms, and course of mumps in immunocompromised children has not been nicely studied. In the transplantation population, reviews of fatal meningoencephalitis and severe nephritis resulting in permanent renal failure have been reported after bone marrow transplantation and renal transplantation, respectively. Adolescents, nonetheless, are extra likely to have prodromal signs similar to low-grade fevers, conjunctival injection, pharyngitis, headache, and diffuse myalgias. Lymphadenopathy, a generally noticed discovering in rubella an infection, arises most frequently during the second week after publicity; nevertheless, it could develop as early as 4 days after publicity, and can precede rash onset by 1 week or more. Lymphadenopathy attributable to rubella is characterised by its posterior auricular, suboccipital, and posterior cervical locations, though generalized lymphadenopathy may be noticed. The whole length of lymphadenopathy averages roughly 7 days, however has been observed up to 14 days after rash onset. The attribute rash has been described as mild, discrete, and erythematous, with a maculopapular look. The rash first appears on the face and neck, with subsequent spread to the trunk and finally extremities, in a centrifugal unfold similar to measles. Unlike measles, nevertheless, the duration of exanthem presence is temporary, with most lasting a mean of three days from onset till complete resolution. In adolescents, the rash may be pruritic, additional differentiating it from the exanthem of measles. Transient polyarthritis and arthralgias might happen, though these findings are extra common in adolescent ladies and adults. Joint symptoms develop 1 to 7 days after exanthem eruption, and often persist for 1 to 2 weeks. Acute rubella encephalitis is an unusual feature of rubella infection, and is estimated to happen in roughly 1 in 6,000 instances. Encephalitis signs commonly start between 2 and 4 days following exanthem appearance, although in some cases they might not occur until 1 week or extra after rash growth. Greater than 80% of those with rubella encephalitis get well without sequelae, although extreme, protracted programs have been reported. In basic, timing of maternal an infection acquisition correlates with severity of infection, with the best variety of abnormalities noticed in kids whose mothers acquired rubella in the course of the first or second trimester of being pregnant. The presence of IgM antibody may be transient in those that have had 1 or 2 doses of measles-containing vaccine. False-negative outcomes are common inside the first 72 hours after rash onset; thus, testing should be repeated if the clinical suspicion remains excessive. Comparison of IgG antibody titers in paired acute and convalescent sera, obtained roughly 2 weeks apart, can be used to diagnose acute measles an infection. IgG antibody ranges are boosted following reexposure, although confirmation requires a second degree to be drawn 14 to 30 days after the preliminary IgG titer. Measles virus is troublesome to cultivate but can be isolated in viral tradition of nasopharyngeal, urinary, or throat swabs, in addition to blood specimens. It is the preferred method of analysis in an immunocompromised host in whom serology is unreliable. Specimens obtained inside 72 hours after rash onset are most probably to yield optimistic development on tradition, with a progressive decline in virus isolation between four and 10 days after rash onset. Genotyping may be useful in determining epidemiology and differentiating an infection attributable to wild-type 374 Succinct Pediatrics virus versus a vaccine virus pressure. Probable: In the absence of a more likely prognosis, an illness characterised by the entire following findings: � � � � � Generalized rash lasting three d Temperature of 38. Mumps A variety of different laboratory strategies are useful for diagnosis of mumps within the nonimmune host. Guidance should be sought from the Centers for Disease Control and Prevention relating to specimen collection via their Web web site or the state health division. Levels peak at approximately 7 days, and can stay elevated for weeks to months after symptom onset. Swabbing of the buccal mucosa/Stensen duct usually yields the best Chapter 32 � Measles, Mumps, Rubella 375 concentration of virus. In the susceptible host, mumps virus could also be isolated from buccal mucosa between 10 and 14 days after the onset of signs. In the vaccine period, parotitis is way extra prone to be brought on by different viral agents than mumps. In addition, there are inherent difficulties in making the analysis of mumps in an immunized particular person. Therefore, session with an infectious diseases specialist may be helpful earlier than endeavor a diagnostic evaluation in such circumstances. Reverse transcriptase-polymerase chain response testing (and to a lesser extent viral culture) seems to be one of the best diagnostic modality for these with partial or preexisting immunity to mumps and in the immunocompromised host. Unlike in the nonimmune host, nonetheless, obtaining this specimen may be critical within the prognosis given the obstacles faced with serologic analysis and theoretical danger of decreased shedding period and amount. Rubella In the susceptible host, laboratory strategies to diagnose rubella are much like these used for measles and mumps. Rubella-specific IgM antibody usually seems within the blood between 4 and 30 days after onset of symptoms, however adequate production could not occur till after seventy two to ninety six hours following onset of symptoms. Thus, repeat rubella IgM testing should be carried out 5 days after onset of rash in sufferers in whom suspicion is high for rubella infection. Other noninfectious sources similar to elevated rheumatoid issue may also be liable for falsepositive rubella IgM test results. Recent rubella infection may be decided by measuring the rise in rubella-specific IgG ranges in paired acute and convalescent sera. In the susceptible host, rubella IgG is usually current inside 8 days after symptom onset. A sharp decline within the focus of detectable virus 376 Succinct Pediatrics in the blood usually coincides with rash onset. Virus could be isolated from oropharyngeal secretions in the course of the interval starting with prodromal symptom onset, up to and together with 14 days after exanthem look. Oropharyngeal specimens obtained within the first four days after rash onset typically yield the highest focus of virus. Reverse transcriptase-polymerase chain reaction testing for rubella virus (sensitivity averaging 80%�90% and specificity of close to 100%) is preferred for analysis within the immunocompromised host.
Generic chloramphenicol 500 mg without prescriptionAcute otitis media should be categorized as extreme or non-severe to assist in treatment decisions (Box 1-1) virus yahoo search buy chloramphenicol 250mg low cost. However, "ear pain" can also be brought on by intense paratonsillar irritation due to pharyngotonsillitis or current tonsillectomy. Therefore, cleaning cerumen or foreign materials from the exterior ear canal is step one toward an accurate analysis. At some level, the ossicle is completely obscured, resulting in no visible landmarks. Effusions may be detected by reduced movement on insufflation of the external ear canal with a pneumatic otoscope. Tympanometry includes applying constant low levels of sound to a sealed external ear canal and measuring reflected versus absorbed sound while various the strain in the canal from negative (<1 atm) to constructive (>1 atm). This results in a linear readout for which the shape indicates whether or not an effusion is current. A regular center ear produces a tympanogram readout designated as an A curve, in which a peak happens at zero stress (the level at which most of the sound is absorbed). Discussion with the radiologist is recommended to be positive that the modality is acceptable for the specified results. Topical brokers containing anesthetics (eg, benzocaine, procaine, or lignocaine) seem to provide temporary aid of ache in youngsters older than 5 years. They could also be of profit for younger kids, however knowledge are inconclusive (Evidence Level I). Orally administered acetaminophen, ibuprofen, naproxen, or codeine/ codeine analogs have been shown to be modestly effective (Evidence Level I). Potential narcotic use should take into account added value and risks inherent with narcotics. Spontaneous perforation relieves much of the ache, however the ragged edges could heal poorly. This is sort of effective 22 Succinct Pediatrics but requires particular training to stop procedural complications. Antimicrobial Treatment Decisions the selection of preliminary antibiotics versus remark is outlined in Table 1-2. Some experts suggest giving households a "rescue" prescription for antibiotics when initially selecting remark (Evidence Level I). Data indicate that less than half the families have to use the rescue prescription. Parents are instructed to call the clinician to report worsening or failure to enhance within 72 hours. Antibiotics are initially preferred because of superior outcome compared to placebo (Evidence Level I). Chapter 1 � Acute Otitis Media and Acute Bacterial Rhinosinusitis 23 return office/clinic visit. The return name could be essential in order that the clinician can really feel assured that a severe invasive complication, one that may require parenteral antibiotics and even hospitalization, has not occurred. This is in contradistinction to ceftriaxone which is extra energetic in opposition to each pneumococci and non-typeable H influenzae than amoxicillin. Modified from American Academy of Pediatrics Subcommittee on Management of Acute Otitis Media. Cefdinir tastes higher however has less scientific efficacy than amoxicillin (against pneumococcus) or its two cephalosporin alternate options (against nontypeable H influenzae), even on the "excessive dose" recommended here. More non-typeable H influenzae and pneumococcal failures are expected with cefdinir than cefuroxime or cefpodoxime. Trimethoprim/sulfamethoxazole dosing is 10 mg/kg/day divided in 2 doses based on the trimethoprim part. Purulent conjunctivitis nearly all the time indicates that the pathogen is non-typeable H influenzae, so a -lactamase�stable drug is beneficial. These medicine are additionally beneficial for each early and late remedy failures of first-line medication (see above). Chapter 1 � Acute Otitis Media and Acute Bacterial Rhinosinusitis 25 or � -Lactamase�stable oral cephalosporin (Evidence Level I). More non-typeable H influenzae and pneumococcal failures are anticipated with cefdinir than cefuroxime. Note: Because no pneumococcal pressure has ever produced -lactamase, -lactamase stability of a drug adds no further exercise towards pneumococcus, however is important in extending exercise towards non-typeable H influenzae and M catarrhalis. Up to 3 doses can be utilized, with second or third doses used when symptoms persist longer than forty eight hours after the prior dose. The 19A strains are most frequently proof against azithromycin and all oral cephalosporins. Almost 40% of circumstances are clindamycin resistant, and up to 30% are ceftriaxone resistant. Consultation with an infectious illnesses expert could be helpful when prescribing these off-label medicine that can have unusual adverse effects. Both are superior to and produce much less opposed effects than oral or other systemic antibiotics. If a foul odor is present, one ought to suspect anaerobes and potential cholesteatoma. Aural toilet (direct cleansing of the external ear canal with suction) is usually a important element to a successful end result. Still, if a toddler has signs suggestive of hearing impairment and bilateral effusions longer than three months, referral to an otolaryngologist is warranted. Otorrhea with a pungent or foul scent could indicate a cholesteatoma, a probably life-threatening condition, and is a sign for referral to an otolaryngologist. Therefore, an important distinction that impacts potential antibiotic remedy is whether or not a secondary bacterial 28 Succinct Pediatrics Box 1-3. Definitions of Acute Bacterial Rhinosinusitis Persistent symptoms A: Nasal discharge (of any quality) or daytime cough (which may be worse at night), or each, persisting for >10 d without enchancment. Recently, sleep disturbance via cough has been advised as more specific than daytime cough. Persistent signs B: Acutely worsening symptoms of nasal discharge or daytime cough (or sleep disturbance via cough), worsening after the sixth day of signs, plus both a new onset of fever (>38. In a recent examine during which more than 2,000 children 1 to 10 years of age with rhinorrhea have been screened, 139 (6. Antimicrobial selections are subsequently substantially the same (see Otitis Media, Antimicrobial Treatment Decisions section). Associations with different ailments, conditions, or exposures embody � Conditions with altered nasopharyngeal anatomy: nasal polyps, deviated septum, inadvertent or medical international bodies, tumors, choanal atresia, or abnormally developed sinus structures.
Diseases - Polycystic ovarian disease, familial
- Macrocephaly pigmentation large hands feet
- Bronchiolitis obliterans with obstructive pulmonary disease
- Cypress facial neuromusculoskeletal syndrome
- Hypogonadism hypogonadotropic due to mutations in GR hormone
- Facial clefting corpus callosum agenesis
- Hearing disorder
- Alport syndrome, dominant type
- Hypomandibular faciocranial dysostosis
Purchase cheap chloramphenicol onlineClinicians will recognize the quick onset and the length of pulpal anesthesia efficacy of antibiotics for acne buy chloramphenicol uk. Using 3% mepivacaine for a supplemental intraosseous injection ends in a short length of pulpal anesthesia (around 30 minutes). Duration of pulpal anesthesia utilizing a plain resolution of 3% mepivacaine is roughly 30 minutes. The repeated intraosseous injection offered an additional 15 to 20 minutes of anesthesia. The key to success with an intraosseous injection the key to success with the intraosseous injection is move of the anesthetic into the cancellous area. Reperforation or choosing another perforation website would be a good selection to acquire access to the cancellous bone. In lower than 10% of intraosseous injections, constricted cancellous areas may limit the distribution of the anesthetic answer around the apices of the teeth. Repeating the intraosseous injection Jensen and coauthors82 found that repeating the intraosseous injection (1. This was just like the period of pulpal anesthesia with the initial intraosseous injection. Significant variations had been found at time intervals three and 4 with the lidocaine solution. In most sufferers, the center rate returned to baseline readings inside four minutes (time period 5). Chamberlain and coauthors77 discovered that the Stabident intraosseous injection of 2% lidocaine with 1:a hundred,000 epinephrine resulted in a imply heart fee enhance of 12 beats per minute. Guglielmo and coauthors73 reported that the supplemental Stabident intraosseous injection of 1. Bigby and coauthors80 discovered a pulse rate enhance of 32 beats per minute utilizing 4% articaine with 1:a hundred,000 epinephrine. Wood and coauthors85 found that a transient heart price enhance (measured with a pulse oximeter) will occur with the intraosseous injection however not with the infiltration injection of 1. Verma and coauthors86 found a 96% incidence of subjective/objective enhance in heart fee with intraosseous injection. Zarei and coauthors87 discovered a transient increase (9 to 10 beats per minute) in heart price with intraosseous injection. Therefore, injection of anesthetic solutions containing vasoconstrictors, using either the Stabident or X-Tip system, will end in a transient coronary heart price enhance. Clinical significance of coronary heart price increase While the heart price enhance with the Stabident or X-Tip intraosseous injection of 2% lidocaine with 1:a hundred,000 epinephrine would probably be noticed by the affected person, it might not be clinically significant in most healthy sufferers. Epinephrine sensitivity After receiving epinephrine-containing options in commonplace infiltrations and nerve blocks, some patients could overreact to the results of epinephrine. They could proceed to give consideration to the uncomfortable feeling that their heart is beating quick, inflicting concern for the practitioner. Because the guts rate results of an intraosseous injection of epinephrinecontaining solutions usually happen extra usually than they do with infiltrations and nerve blocks, we advocate that dental practitioners choose 3% mepivacaine for these patients. Medical circumstances as contraindications to vasoconstrictors Vasoconstrictors are contraindicated for intraosseous anesthesia in patients with untreated hyperthyroidism and pheochromocytoma. However, these conditions are contraindica146 Intraosseous Anesthesia tions to even routine dental treatment. Drug therapies as contraindications to vasoconstrictors Please evaluate the discussion of vasoconstrictors and drug interaction in chapter 1. In basic, the recommendations on drug interactions state that minimal dosages of epinephrine ought to be used with frequent aspiration and a gradual price of injection. Mepivacaine in medically compromised sufferers There shall be no vital improve in coronary heart fee when 3% mepivacaine is used for intraosseous anesthesia. Long-acting anesthetic brokers In an try and increase the length of pulpal anesthesia with intraosseous injections, some clinicians might use long-acting anesthetic brokers. Plasma ranges of lidocaine Some authors have cautioned that administration of a very massive quantity of native anesthetic with an intraosseous injection could lead to overdose reactions. Additionally, if it had been an intravascular injection, little or no anesthetic effect could be demonstrated. That is, all of the local anesthetic answer can be carried into the vascular system with none left for pulpal anesthesia. Obviously, medical and experimental studies have demonstrated medical anesthesia with intraosseous strategies. No vital differences had been seen between the two methods at any time interval. Postoperative results Discomfort As a main and supplemental approach with the Stabident system, approximately 12% of sufferers will report average postoperative pain. They felt this was related to denser and extra mineralized bone in the posterior mandible in males and the reality that the diameter of the X-Tip perforating system is larger than the diameter of the Stabident perforator, resulting in extra frictional warmth throughout perforation. Gallatin and coauthors94 found that the X-Tip system could have a barely higher incidence of postoperative swelling clinically. With both methods, the swelling and exudate may be current for weeks after the injection however will often resolve with time. Over the final 10 years, anecdotal stories conveyed to the authors from clinicians who use intraosseous anesthesia routinely for endodontic therapy have outlined a really uncommon incidence of nonhealing websites that required a minor surgical process (curettage) for decision. Recently, Woodmansey and coauthors95 wrote a case report by which osteonecrosis supposedly occurred as a result of intraosseous anesthesia. Basically, an inexperienced dental student performed the intraosseous injection and separated a portion of an X-Tip perforator. Judging from the pictures in the article, the intraosseous injection was coronal to the perfect website. The incidence with the intraosseous injection is decrease than that reported with the intraligamentary injection (37% incidence). Precautions Do not use intraosseous injections in painful enamel with necrotic pulps and periapical radiolucencies or enamel exhibiting cellulitis or abscess formation. Although it has not been studied, sufferers taking oral bisphosphonates may have the ability to obtain intraosseous injections. Supplemental injections ought to lead the clinician to successful pulpal anesthesia. The anesthetic efficacy of articaine in buccal infiltration of mandibular posterior enamel. Periodontal ligament injection: An evaluation of the extent of anesthesia and postinjection discomfort. Single-tooth anesthesia: Pressuresensing expertise offers revolutionary advancement in the area of dental local anesthesia.
Generic 500mg chloramphenicol free shippingHowever infection joint replacement order chloramphenicol cheap, with use of both volumes, there was the next incidence of average pain in the lateral incisor in comparison with the posterior tooth. This demonstrates again that the anterior maxilla is more delicate than the posterior space. The larger quantity was significantly better from the twenty first minute until 59th minute (asterisks). The greater quantity was considerably higher from the 49th minute until the 59th minute (asterisks). Pitt Ford and coauthors9 additionally found that the next epinephrine concentration elevated duration in maxillary central incisors. Mason and coauthors19 discovered that increasing the epinephrine concentration to 1:50,000 epinephrine was not considerably totally different than using a 1:one hundred,000 epinephrine formulation in the maxillary first molar. For the initial infiltration, approximately 78% of the topics had pulpal anesthesia at half-hour. However, at forty five minutes, approximately 60% of the subjects had pulpal anesthesia, and at 60 minutes, solely 33% had pulpal anesthesia. With the repeated infiltration, 90% of the subjects had pulpal anesthesia at 60 minutes. At seventy five minutes, roughly 85% of the subjects had pulpal anesthesia, and at ninety minutes, 70% have been anesthetized. Knowing that standard infiltration anesthesia is of brief duration and that repeating the infiltration at 30 minutes will provide pulpal anesthesia for 60 minutes or longer should be very useful. The repeated infiltration considerably improved pulpal anesthesia from the 37th minutes via the 90 minute. The repeated infiltration considerably improved pulpal anesthesia from the twenty eighth by way of the 109th minute. Loetscher and coauthors46 evaluated pulpal anesthesia in an experimental research utilizing 30 topics, 1. Intraoral infraorbital nerve block Malamed21 describes the maxillary infraorbital nerve block as an efficient technique of achieving profound pulpal anesthesia from the maxillary central incisor through the canine. He states that the pulps of the premolars and the mesiobuccal root of the first molar may even be anesthetized in about 72% of sufferers. Corbett and coauthors50 found related results utilizing 1 mL of 2% lidocaine with 1:80,000 epinephrine. Successful pulpal anesthesia of the canine and first and second premolars ranged from 75% to 92% utilizing 2% lidocaine with 1:100,000 and 1:50,000 epinephrine. The use of 3% mepivacaine offered a shorter length of anesthesia than the lidocaine formulations with epinephrine within the canines and premolars. For pulpal anesthesia, this injection approach is just like an infiltration injection over the premolars. A plain resolution of 3% mepivacaine leads to an even shorter duration of pulpal anesthesia. The intraoral infraorbital nerve block was ineffective in providing profound pulpal anesthesia of the maxillary central incisor, lateral incisor, and first molar. Successful pulpal anesthesia of the canine and first and second premolars ranged from 75% to 92% utilizing the lidocaine formulations. The 3% mepivacaine formulation offered a shorter period of anesthesia than the lidocaine formulations with epinephrine within the canines and premolars. Needle insertion pain and postoperative sequelae were more widespread with the extraoral infraorbital nerve block. Both nerve blocks have been ineffective in providing profound pulpal anesthesia of the maxillary central incisor, lateral incisor, and first molar. Successful pulpal anesthesia of the canine for both nerve blocks was 92%; success of the primary and second premolars ranged from 80% to 90%. Second division nerve block Malamed21 described the second division nerve block as an efficient technique of reaching profound anesthesia within the hemimaxilla. Broering and coauthors63 in contrast the anesthetic efficacy of the larger palatine second division nerve block and the high tuberosity second division nerve block technique utilizing three. Both techniques had been ineffective for profound pulpal anesthesia of the anterior tooth and first premolars. High tuberosity second division nerve block using 3% mepivacaine Forloine and coauthors64 compared the anesthetic efficacy of three. Approximately 76% to 78% of the second premolars were anesthetized with both anesthetic formulations. Both anesthetic formulations have been ineffective for the anterior tooth and first premolars. Using 2% lidocaine with 1:one hundred,000 epinephrine, the first and second molars had the highest success charges. The 3% mepivacaine resolution offered a significantly shorter duration of pulpal anesthesia. Palatal�anterior superior alveolar nerve block Traditionally, maxillary anterior tooth have been anesthetized by administering an infiltration injection near the apex of the target tooth. For needle placement into the incisive canal, 54% to 58% of the topics reported moderate-to-severe ache. For anesthetic resolution deposition, 8% to 12% of the topics reported reasonable ache. Regarding postoperative pain after numbness wore off on the day of the injection, 12% to 18% of the themes reported moderate pain, and 2% reported severe pain. Postoperative issues have been relatively minor, with roughly 12% to 18% of the themes having experienced temporary numbness/paresthesia of the incisive papilla and 20% to 28% having had incisive papilla swelling or soreness. Corbett and coauthors50 discovered the next success fee for this injection using 1 mL of 2% lidocaine with 1:eighty,000 epinephrine. Tetracaine nasal spray for maxillary anesthesia Ciancio and coauthors77 evaluated tetracaine/oxymetazoline nasal spray for anesthesia of maxillary enamel. The authors discovered that the mixture nasal spray was adequate for numerous maxillary dental procedures. Renatus) was lately cleared by the United States Food and Drug Administration for dental use. It is used for restorative procedures on the premolars and anterior tooth as properly as the maxillary major teeth in children who weigh 88 kilos or more. Addition of mannitol to lidocaine for maxillary infiltrations Younkin and coauthors78 decided the anesthetic efficacy of lidocaine with epinephrine compared to lidocaine with epinephrine plus 0. Buccal and palatal infiltration of the primary molar Guglielmo and coauthors79 evaluated the anesthetic efficacy of a mix palatal (using zero. The buccal plus palatal infiltration significantly elevated the incidence of pulpal anesthesia from 21 by way of fifty seven minutes.
Order chloramphenicol in united states onlineWe feel that maybe some change in intrapulpal stress happens when the pulp is entered and results in this preliminary ache virus joint pain buy 500mg chloramphenicol mastercard. Anesthesia must be efficient with the supplemental intraosseous injection for approximately 30 minutes with 3% mepivacaine10 and 60 minutes with 2% lidocaine with 1:a hundred,000 epinephrine. Alternative alternative for supplemental anesthesia Although not as efficacious as intraosseous anesthesia, intraligamentary anesthesia can be given on the mesial and distal facet of the tooth using 2% lidocaine with 1:one hundred,000 epinephrine. The first intraligamentary injection may be profitable from 63% to 74% of the time14�16; reinjection will increase success to 92% to 96%. When supplemental anesthesia is required An infiltration of 4% articaine with 1:a hundred,000 epinephrine is given over the site of the proposed intraosseous injection to assist lower the pain of the injection. If initial pain occurs in dentin, take away the rubber dam and readminister the supplemental intraosseous injection utilizing 1. If the initial ache happens when the pulp is entered, remove the rubber dam and administer a cartridge of 3% mepivacaine or 2% lidocaine with 1:a hundred,000 epinephrine intraosseously. For supplemental intraosseous injections, anesthesia should be effective for round 30 minutes with 3% mepivacaine10 and 60 minutes with 2% lidocaine with 1:100,000 epinephrine. Once the lip is numb (soft tissue anesthesia is required in the mandible for achievement of the supplemental injections), add a labial infiltration of 1. Pulpal anesthesia must be efficient for roughly half-hour with a labial infiltration of 1. For intraosseous anesthesia, anesthesia must be efficient for round half-hour with 3% mepivacaine10 and 60 minutes with 2% lidocaine with 1:100,000 epinephrine. Slowly administer an infiltration utilizing a cartridge of 2% lidocaine with 1:one hundred,000 epinephrine. If the affected person responds to chilly, you can wait a further three to 5 minutes and retest. Red, rare; green, No response If pain (rare) Proceed with remedy No response Proceed with remedy very uncommon. This regimen should work the majority of the time in anesthetizing the posterior tooth. Therefore, if pain is experienced through the later phases of instrumentation or obturation, a further infiltration injection is important. Slowly administer an infiltration utilizing a cartridge of 2% lidocaine with 1:50,000 or 1:100,000 epinephrine. This regimen should work the majority of the time in anesthetizing the anterior enamel. Because intraligamentary anesthesia could be very painful in anterior tooth, has a success fee of solely 39% in asymptomatic teeth, and offers only a 10-minute length of anesthesia,17 intraosseous anesthesia is the best choice. It is important to realize that anesthesia starts to decline after an preliminary infiltration in anterior tooth. If the patient experiences ache in the course of the later phases of instrumentation or obturation, an extra 1. Other Considerations for Endodontic Anesthesia Symptomatic tooth with total pulpal necrosis and apical pathosis When patients present with symptomatic teeth, and examination reveals complete pulpal necrosis and periapical radiolucencies, this is an indication of pain in the periapical tissue. Because these tooth may be painful to manipulation and motion throughout therapy, additional care must be taken. For maxillary teeth with no swelling, administer anesthesia with standard infiltrations. After reaching indicators of anesthesia, place rubber dam and slowly start the entry. Hand and rotary file placement and debridement could be performed with out a lot ache if devices are finessed. Do not use intraosseous injections, intraligamentary injections, or intrapulpal injections. While efficient for tooth presenting with irreversible pulpitis, these injections would likely be very painful and ineffective for symptomatic necrotic teeth with apical pathosis. Asymptomatic teeth with complete pulpal necrosis and apical pathosis Patients presenting with asymptomatic tooth with pulpal necrosis are the best to anesthetize; affected person consolation is normally attained with out difficulty. On rare events, there could additionally be some discomfort throughout canal preparation requiring an intraosseous or intraligamentary injection. Do not inject intrapulpally as a outcome of micro organism and particles may be pressured from the canal into the periapical tissue. In the maxilla, a further infiltration could additionally be needed if anesthesia begins to put on off. Incision and drainage We should at all times attempt to achieve some stage of anesthesia before performing an incision and drainage process. The conventional perception is that injecting instantly right into a swelling is contraindicated. The causes given have been the attainable spread of an infection and that the anesthetic options would be affected by the decrease pH and would be rendered less efficient. However, a fundamental science investigation discovered that native anesthetics may be profitable in inflamed tissue, which is acidified. Injecting into this space causes the anesthetic to be carried away into the systemic circulation quite than effectively numbing the area domestically. Periapical surgical procedure It have to be remembered that anesthesia is required for both gentle tissue and bone. Additional infiltration injections within the vestibule are helpful to obtain vasoconstriction, particularly in the anterior mandible. Usually larger volumes are essential to provide anesthesia over the surgical area. That is, for maxillary anterior teeth, a cartridge of 2% lidocaine with 1:50,000 epinephrine may be given over the tooth requiring an apicoectomy, and a cartridge of 2% lidocaine with 1:100,000 epinephrine is given over each adjoining tooth. Gutmann and coauthors25 reported that larger concentrations of vasoconstrictors can be used during surgical procedures. In the premolars and molars, a cartridge of 2% lidocaine with 1:100,000 epinephrine may be given over the tooth requiring an apicoectomy, and a cartridge of 2% lidocaine with 1:a hundred,000 epinephrine is given over every adjoining tooth. After anesthetizing the palatal tissue initially, a cartridge of 2% lidocaine with 1:one hundred,000 epinephrine is given over the apex of the tooth. If the surgical area is infected or the patient is apprehensive, anesthesia may not be totally profitable. Yamazaki and coauthors26 discovered that the effectiveness of surgical anesthesia is decreased by half in comparison with anesthesia for nonsurgical procedures. We have discovered anecdotally that when surgical anesthesia in the course of the latter part of the surgery is insufficient, giving a palatal infiltration over the surgical website is helpful in the maxilla. As a prophylactic measure, an intraosseous injection could additionally be administered on the web site after routine injections and earlier than the surgical procedure.
Syndromes - Low blood pressure
- CSF VDRL test
- Decreased alertness
- Severe mental dysfunction
- Shoulder shrugging
- Salivary gland tumors
- Seizures
- Slow urinary stream
Chloramphenicol 500 mg otcDiagnosis could also be made on medical grounds virus xp order 250mg chloramphenicol, with testing and early establishment of treatment really helpful for high-risk patients. Morbidity and mortality are greatest within the very young, the elderly, and those with cardiopulmonary, metabolic, neurologic, and immunocompromising situations. Overview Influenza virus an infection is a notable explanation for higher respiratory tract sickness in kids, causing vital morbidity and mortality on this susceptible population. Influenza viruses even have the potential for inflicting periodic international pandemics, as exemplified by the 2009 H1N1 outbreak. Causes and Differential Diagnosis Influenza viruses are orthomyxoviruses of 3 types (A, B, and C). Influenza virus varieties 354 Succinct Pediatrics A and B are the principal pathogens indicated in epidemic illness. Influenza virus sort C is thought to trigger sporadic, gentle influenza-like sickness in kids. Annual winter epidemics of influenza A (H1N1 and H3N2) and B are predictable and customarily related to significant mortality in elderly and certain different high-risk populations. Annual antigenic drift in subtype relates to minor variation within the virus, and produces the seasonal adjustments in circulating virus. Antigenic shift, on the other hand, occurs only when influenza A virus is the gas of pandemics. Since viral shedding in nasal secretions can persist for 7 to 10 days, and longer in younger children and immunodeficient patients, the virus effectively circulates, especially in close-knit populations. Specific antibodies to these numerous antigens, particularly to hemagglutinin, are necessary determinants of immunity. Rates of communal immunity, in turn, affect incidence charges of the influenza virus. Upper respiratory tract infections attributable to other infectious pathogens share the same host of signs. Influenza usually presents with a higher severity of symptoms (eg, fever, chills, myalgia) than the extra common higher respiratory tract an infection (eg, nasal congestion, rhinorrhea). Clinical Manifestations the virus is often marked by a host of symptoms together with acute onset of high fever, chills, rigors, malaise, headache, diffuse myalgia, and nonproductive cough. Subsequent signs and symptoms embody nasal congestion, rhinitis, sore throat, and persistent cough. Less notable symptoms embody belly pain, vomiting, diarrhea, nausea, and conjunctival injection. Cough could persist for longer periods, and indication of small airway disturbance is usually discovered weeks later. Although most kids with influenza recover fully after 3 to 7 days, beforehand healthy children might reveal extreme symptoms and complications. Reported sequelae of the influenza virus embody quite a lot of secondary diseases. Complications might embody acute otitis media, neurologic problems (eg, encephalopathy, seizures), myocarditis, pneumonia, bronchiolitis, sepsis, myositis, parotitis, and nephritis. A post-influenza myositis could follow both influenza A or B, although more generally the latter. Affected patients, often school-aged boys, typically Chapter 31 � Influenza 355 develop extreme calf ache 3 to 4 days into their scientific sickness and refuse to weight bear. Laboratory testing may reveal leukopenia and occasionally thrombocytopenia with blood creatine kinase elevated concentrations within the vary of 1,000 to 5,000 U/L. Rhabdomyolysis resulting in renal failure occurs not often, and extra generally in women. Influenza is especially extreme in youngsters with predisposing conditions similar to hemoglobinopathies, diabetes mellitus, persistent renal illness, malignancy, cardiopulmonary illness, cardiomyopathy, and chronic lung disease, together with bronchopulmonary dysplasia, bronchial asthma, cystic fibrosis, and neuromuscular ailments, which affect the accent muscle tissue of respiratory. Mortality secondary to the influenza virus has been reported in youngsters with underlying continual disease in addition to previously wholesome youngsters. Invasive secondary infections with group A Streptococcus, Staphylococcus aureus, Streptococcus pneumoniae, or different bacterial pathogens could end in severe disease and dying. Other laboratory exams, corresponding to a complete blood cell rely, are additionally not essentially indicated in confirming the prognosis of influenza illness. A complete blood cell count or blood tradition, nonetheless, may show useful in instances when bacterial superinfection or concomitant bacterial disease is suspected. In patients with confirmed illness, it may reveal hyperaeration, peribronchial thickening, diffuse interstitial infiltrates, or bronchopneumonia in severe cases. Enlarged hilar lymph nodes and pleural effusion are rare in uncomplicated influenza. A excessive index of suspicion for the diagnosis is influenced by the seasonality of influenza. Influenza testing should be performed in any of the following populations: � Patients hospitalized with suspected influenza � Patients for whom a analysis of influenza will warrant changes in clinical care (Box 31-1) � Treatment of close contacts of patients who died of an unspecified acute sickness in which influenza was suspected Respiratory tract specimens should be collected shortly after illness onset, preferably within the first seventy two hours of sickness. Specimen collection after 5 days of sickness onset may end in false-negative results because of a marked lower in amount of viral shedding over time. Optimal specimens in infants and younger kids embody nasal aspirates and swabs. Oropharyngeal and sputum specimens end in a lower yield for influenza virus detection. In patients undergoing mechanical air flow, higher and lower respiratory tract samples ought to be obtained. Lower respiratory tract samples embody endotracheal aspirates and bronchoalveolar lavage. Specimens of nasopharyngeal secretions obtained by swab, aspirate, or wash should be placed in applicable transport media for tradition. After inoculation into eggs or cell culture, influenza virus usually can be isolated within 2 to 6 days. Clinical profit is greatest when treatment is initiated within forty eight hours of onset of signs. Influenza testing strategies are varied, and the particulars of a given scientific scenario will dictate which sort of influenza test is the best option. Each technique of testing has its personal advantages and drawbacks, as described in Table 31-1. It is imperative to use scientific judgment in deciding whether or not any affected person with an influenza-like illness ought to be treated regardless of check results, especially because of the poor sensitivity of fast influenza diagnostic testing. Confirmatory testing (viral culture or reverse transcriptasepolymerase chain reaction) ought to be thought of in these instances to confirm accurate outcomes. Clinical judgment is a vital consider remedy choices for pediatric patients presenting with influenza-like sickness.
Purchase cheap chloramphenicol lineA 78-year-old Caucasian man presents to the emergency division with a several-week historical past of stomach ache that has significantly worsened over the previous 12 hours bacteria 6th grade buy chloramphenicol 500mg with visa. He describes the ache as severe, midabdominal in 60 Topics Involving Multiple Organs location, and accompanied by again pain, which is worse mendacity down and improved considerably by leaning forward. On physical examination, a pulsatile mass is noted left of the umbilicus, and he has tenderness to palpation and mild guarding diffusely. A 36-year-old man presented to emergency division after trauma to his abdomen throughout taking part in basketball. A 63-year-old man presented with nausea, periumbilical ache, and a 15-pound weight reduction up to now 3 months ago. Open biopsy of the mass showed irritation and fibrosis with no proof of tumor. A 55-year-old man underwent laparotomy and partial small bowel resection following bowel perforation. What is the most common organism associated with peritonitis secondary to continuous peritoneal dialysis A 35-year-old girl with previous medical historical past of pelvic inflammatory illness and diabetes mellitus introduced with fever and right upper quadrant abdominal ache. Abdominal exam showed proper upper quadrant Chemistries are normal, together with a lipase. Ruptured abdominal aortic aneurysm with hemorrhage within the retroperitoneal space D. Small bowel protruding by way of an belly wall defect with a narrowed neck of the hernia sac 113. A 68-year-old girl with a history of systemic sclerosis and arthritis presents with lightheadedness and fatigue and reports a number of days of dark tarry stools. Her vital indicators are as follows: Blood stress 108/68 mm Hg Heart price ninety five bpm Respiratory fee 16 breaths/min Oxygen saturation 99% Her conjunctiva and mucous membranes are pale, and stomach examination is unremarkable. A 50-year-old woman with no past medical history introduced with belly pain and distention. Kidney Topics Involving Multiple Organs tenderness with out guarding or rebound tenderness. Abdominal ultrasound was performed, which confirmed small quantity of ascites, normal gall bladder, and normal liver size and counter. Cytology showed no malignant cells, and culture of ascites fluid was negative for any bacterial an infection. A 25-year-old lady G1P0, 36 weeks pregnant with none previous medical history of liver illness offered to the emergency division with nausea, vomiting, belly ache, jaundice, and confusion. Vital indicators are as follows: Temperature 99� F Blood strain 95/65 mm Hg Heart price 102 bpm the patient has evidence of asterixis and is disoriented to time, place, and individual. The hallmark of liver biopsy is periportal hemorrhage and intrasinusoidal fibrin deposition B. A 38-year-old pregnant girl, 35 weeks pregnant offered with complaint of heartburn, regurgitation, nausea, and vomiting. Fungal peritonitis Secondary bacterial peritonitis Spontaneous bacterial peritonitis Chlamydia peritonitis Starch peritonitis one hundred twenty. Abdominal ultrasound revealed regular size and contour of the liver, normal gallbladder, and reasonable sized ascites. Abdominal paracentesis was performed, which confirmed low serum to ascites albumin gradient (<1. She would want to cease penicillamine during pregnancy, as this treatment is teratogenic. She can begin taking penicillamine in the second trimester and can proceed taking zinc throughout pregnancy C. She should continue at a low dose of penicillamine necessary for chelation and zinc throughout pregnancy sixty two Topics Involving Multiple Organs a hundred thirty. Which of the following situations could be difficult by hepatic rupture throughout pregnancy A 56-year-old man with historical past of gastric adenocarcinoma presented with diarrhea with 4 to five loose, nonbloody bowel actions per day and abdominal bloating for the previous three months. He received chemoradiotherapy therapy as a part of the treatment for gastric adenocarcinoma 2 years ago. On bodily exam his very important indicators are as follows: Temperature 37 � C Blood pressure 110/60 mm Hg Heart price eighty bpm Respiratory price 12 breaths/min His belly exam is mildly distended and nontender. Initial laboratory blood work revealed low vitamin B12 level and excessive folic acid degree. He was advised to receive chemoradiotherapy for prostate cancer and wants to know if he has any threat components for radiation-induced colitis. A 70-year-old man with history of prostate cancer treated with radiation therapy 2 years in the past current with hematochezia and diarrhea. A 28-year-old Asian lady, eight weeks pregnant G1P0, is seen in clinic for evaluation of her hepatitis B infection. A 28-year-old lady G1P0, 10 weeks pregnant presented to your workplace with extreme nausea, vomiting, and a 5-pound weight reduction. Phenothiazines are useful if antiemetic, and antireflux therapies fail to treat nausea 128. A 35-year-old lady, 35 weeks pregnant G2P1 presented with nausea, vomiting, headache, and blurred vision. Diagnosis based on evaluation of clinical circumstances and the time of presentation is normally not accurate E. She has history of complicated cholecystitis and underwent open cholecystectomy three years in the past. Which intestinal cell damage primarily contributes to the pathophysiology of acute radiation-induced proctitis A 65-year-old man with historical past of knee replacement surgical procedure 1 yr in the past who presents for a colonoscopy with random biopsies for evaluation of diarrhea E. A 60-year-old girl with previous medical history of diabetes mellitus and hypertension offered for screening colonoscopy. Colonoscopy was performed, which revealed normal colonic mucosa and scattered diverticulosis. Three hours after the procedure, the patient started having progressive belly ache and nausea. On presentation to the emergency division, her very important signs included the following: Temperature 37. Temperature Blood stress Heart fee Respiratory rate 37� C 110/60 mm Hg 80 bpm 12 breaths/min His stomach examination is gentle and nontender. A 64-year-old man with history of non�small cell carcinoma of the lung underwent lobar resection. Three weeks following initiation of the radiation remedy, he developed sharp sudden onset of chest ache. Intravenous fluids, serial belly exam, and consultation to basic surgical procedure for urgent laparotomy E. A 34-year-old woman with a history of alcoholic cirrhosis offered to the hospital with complaints of dizziness and hematemesis.
Purchase chloramphenicol with a visaInitial makes an attempt to bypass the obstacle to guarantee patency of the distal esophagus does antibiotics for acne work discount chloramphenicol 500 mg mastercard, permitting the foreign physique to be superior into the abdomen, are met with resistance and were terminated. Terminate the procedure, give glucagon 1 mg intravenously, and reattempt endoscopy in 12 hours B. Withdraw endoscope, insert an overtube and try piecemeal international physique removing C. Terminate procedure, give carbonated drink, and reattempt endoscopy in few hours D. Terminate process and use a colonoscope to push the international physique into the stomach 25. Initially her disease was diagnosed roughly 2 years ago, and she was maintained on azathioprine 50 mg by mouth per day and intravenous infliximab 5 mg/kg every 6 weeks. Despite immunomodulators and biologic remedy, she continued to develop intermittent flares of her forty eight Topics Involving Multiple Organs disease, presenting with proper lower quadrant uninteresting discomfort and unfastened bowel actions. The affected person now states that her symptoms from earlier this week are different, as her ache is now sharp and progressive. Following the initiation of intravenous normal saline, antibiotics, and admission, the intraabdominal abscess is drained percutaneously under radiographic steering. The following day, the patient denies any pain, her white cell count has normalized, and she feels markedly improved. In anticipation of surgical and medical intervention, the query of when to discontinue the percutaneous catheter arises. Discontinuation of percutaneous catheter after complete cessation of drainage and an extra 3 days of antibiotics E. Discontinuation of percutaneous catheter after full cessation of drainage and an extra 5 days of antibiotics to the emergency division, complaining of large fluid output from a gap on his belly wall in the left upper quadrant. The patient is status postresection of 20 cm proximal jejunum, sophisticated by postoperative infection because of partial dehiscence with out free air that required a prolonged hospital course and conservative management with antibiotics. Initially, he noted an erythematous nodular lesion in his left higher quadrant that eventually began draining clear fluid however developed into discharge of stable food and a appreciable quantity of fluid. This morning after waking up, he noted huge discharge from the opening in his left upper quadrant, soiling his mattress and garments, in addition to a syncopal episode. The patient is being admitted for dehydration and was started on intravenous fluids. As a consultant for immediate administration of the fistulous tract, what are your suggestions Surgical session for resection and revision of the fistulous tract and anastomosis B. Intravenous regular saline supplemented with potassium to match the output from the fistulous tract E. The patient had an uneventful postoperative recovery, has resumed his daily actions, denies any ache, nausea, or vomiting, and maintains a normal appetite, regaining three pounds of weight over the past 2 weeks since being discharged from the hospital. His stomach exam is remarkable for left upper quadrant, well-healed incision, with out evidence of inflammation or an infection. The affected person inquires about infectious issues, being on two medications to management his disease and is anxious in regards to the recurrence of fistulae. Which of the following statements is true relating to fistulae recurrence after surgical resection The fistulous tract extends from the proximal jejunum to the periumbilical space, confirmed by fistulogram and small bowel follow-through. Management of the fistulous tract has been tough, as the output decreased by only 25% in response to intravenous infliximab 5 mg/kg every 6 weeks. You increase the frequency of infliximab to each four weeks, added weight-adjusted azathioprine at 75 mg by mouth per day, which resulted in further discount of output from the fistula, estimated at 50%. Physical examination revealed the fistula, but in otherwise soft, nontender abdominal exam, with a normal-sized liver and no palpable spleen tip. The patient is eager to get the signs beneath control, considering interference of the illness together with his social and professional life. A 24-year-old man with a gunshot wound to the abdomen 3 months in the past and exploratory laparotomy, presents Topics Involving Multiple Organs A. Ill-defined heterogeneous assortment, tissue response surrounding the fluid assortment E. A 18-year-old man presents to the emergency division after an argument that escalated into a knife flight, receiving a stab wound to the left upper quadrant. The patient arrives at your native hospital with steady vital signs, 2 out of 10 sharp pain in the left higher quadrant, and a small, nonbleeding incision near the tenth rib. Postoperatively, the affected person is admitted for statement and was discharged 3 days later. Within 10 days, the affected person returns for followup to surgical procedure clinic with the complaint of left higher quadrant pain, nausea, vomiting, and a temperature to 40 � C. Which of the next is true relating to endoscopic drainage of intraabdominal abscesses An abscess within the left infradiaphragmatic location ought to at all times be drained surgically C. The abscess can be amenable for endoscopic drainage, unbiased of anatomic location but dependent on distance of lumen to abscesses wall being lower than 2. Endoscopic drainage is feasible for the infradiaphragmatic location, with a lumen to abscesses wall distance of 1 cm or much less E. Endoscopic drainage ought to only be considered after unsuccessful makes an attempt by interventional radiology 31. A 36-year-old man is seen in clinic for follow-up of eosinophilic esophagitis (EoE). Endoscopy was performed to disimpact the food bolus, and biopsies from the mid and distal esophagus showed eosinophilic infiltration of the mucosa. Over the final 12 months, he had three episodes of esophageal meals bolus obstruction. An upper endoscopy is performed, and biopsies from the mid and distal esophagus confirmed eosinophilic infiltration of the mucosa, forty nine appropriate with EoE. However, he improves symptomatically after beginning swallowed topical fluticasone. A 63-year-old girl presents to her primary care physician for weight loss and belly discomfort for the previous 6 months. Biopsy specimens from the abdomen, duodenum, and colon reveal dense eosinophilic infiltration, suggestive of eosinophilic gastroenteritis. Which of the following infections need to be dominated out previous to starting remedy A 25-year-old man is seen in clinic for evaluation of intermittent dysphagia for the previous 6 months. He feels that stable food gets caught in the midst of his chest however has no problems with liquids. An higher endoscopy is carried out, which reveals regular esophagus with no strictures. A 12-year-old woman presents to her gastroenterologist complaining of intermittent midepigastric ache, diarrhea, and occasional nausea and vomiting.
Discount chloramphenicol 500 mgManagement Previously antimicrobial keyboard and mouse buy chloramphenicol 250mg amex, full surgical excision was really helpful, and this continued to be true for first and second branchial lesions. However, latest proof suggests that in third and fourth arch anomalies, endoscopic obliteration of the opening of the tract is adequate to stop recurrence or reinfection. Vascular anomalies Vascular tumors Benign Locally aggressive Malignant Vascular malformations Simple Capillary malformation Lymphatic malformations Venous Malformations Combined Arteriovenous malformations current within the neck space. We will cowl the extra frequent types, which Hemangioma Infantile hemangiomas are widespread, benign vascular tumors, however must be differentiated from the more aggressive types of vascular tumors (Table 36. The incidence is elevated (23%) in untimely babies with a delivery weight < 1,200 g. Sixty percent of infantile hemangiomas occur within the head and neck area and 20% shall be associated with different lesions within the mind, gastrointestinal tract, or liver. They develop quickly during infancy and have three distinct clinical, microscopical, and immunohistochemical phases. The proliferative part lasts 6�9 months and after 12 months the tumors are likely to shrink, fade, and flatten (involution phase). More than 50% youngsters have full resolution by the age of 5 years with further improvement until age of 12 years (involuted phase). Almost half of the kids have some residual abnormality similar to residual fibrofatty tissue, redundant skin, yellow discoloration, or telangiectasia (Abramowicz and Padwa, 2012). They may be subclassified in phrases of the pattern of presentation and depth of the lesion. There has been a big administration shift when propranolol was found to have a constructive beneficial effect in lowering the proliferative section of this situation, and lots of circumstances have averted destructive local development and surgical extirpation. Rapidly involuting congenital hemangiomas are raised, red-violaceous lesions with central telangiectasia, superficial ulceration, and a peripheral pale halo. They seem in head and neck, including the airway, behind the ear, or on the scalp. Vascular Malformations Vascular malformations end result from abnormal embryonic growth. Slow-flow vascular malformations could trigger bony deformation and fast-flow lesions might trigger osteolysis. Venous Malformations Venous malformations are the commonest vascular anomaly and end result from abnormal venous growth. They encompass thin walled, dilated channels with regular endothelium but poor in easy muscle. They generally come up underneath pores and skin, but may additionally be current in other tissues and organs. Presentation Venous malformations are typically blue�purple in colour but this depends on the depth of the lesion and the diploma of enlargement of the affected vessels. More superficial lesions are darker in color, usually maroon pink, while deeper lesions are bluish. If the child cries or lies down, the lesion expands and the colour can become intense. Generally, the indications for intervention are lesions inflicting pain, creating deformity, producing gastrointestinal bleeding, affecting imaginative and prescient, or obstructing important structure. Sclerotherapy: the infiltration of drugs similar to absolute alcohol, 3% sodium tetradecyl sulfate, and bleomycin, could cause shrinkage in 75�90% lesions. Management includes selective embolization, sclerotherapy, surgical resection, and reconstruction. They occur in 1 in 2,000�4,000 stay births and are mostly isolated lymphatic lesions but might combine with arterial or venous vasculature to form a blended lymphovascular lesion. Cystic lymphatic malformations are stated to be benign in growth but their infiltrative development pattern causes vital impact on surrounding tissues. They are described as microcystic or macrocystic (or combined) depending on the scale of the malformed channels. Arteriovenous Malformation Arteriovenous malformations end result from abnormal communication between arteries and veins without the normal capillary bed. Progression is indicated by the onset of pain, pruritus, or enlargement and they could endure fast growth following trauma (including attempted ligation) or throughout puberty. Clinical development proceeds from quiescence, by way of growth, destruction, and decompensation as described by the Schobinger staging system. Magnetic resonance imaging shows dilated feeding arteries and draining veins with flow voids. Presentation Cystic lymphatic malformations current as a gentle, compressible cystic mass, which transilluminate and could additionally be small or extensive. They could occur anyplace in the body but generally arise within the head and neck region, where they contain the neck, tongue, cheek, and cervicofacial region. Two-thirds of kids with cervicofacial lymphatic malformations require a tracheostomy for airway maintenance. Good oral hygiene ought to be maintained to forestall an infection and long-term antibiotics thought-about in sufferers with larger than three infections in a year. Small lesions may be observed, but those encroaching on very important buildings, causing deformity or ache, require treatment. As many of these lesions seem to expand significantly with localized infections, children with adenotonsillar infections might require surgical ablation of these areas. It arises from undifferentiated mesenchymal tissue with potential for malignant skeletal myogenesis and is broadly divided into embryonal and alveolar varieties. It has bimodal shows with peaks in incidence between the ages of two and four years, and 12 and sixteen years. Thirty-five p.c childhood rhabdomyosarcomas happen in the head and neck area. These are typically embryonal and comprise 13% of pediatric head and neck malignancies. Seventy-five % head and neck rhabdomyosarcomas occur within the orbit or parameningeal areas and the remainders are collectively named nonorbital nonparameningeal tumors. Embryonal rhabdomyosarcomas are additional subdivided into botryoid and spindle cell varieties and are the commonest kind within the head and neck region. They occur barely extra regularly in males and have a better prognosis than alveolar, which is usually found in extremities. Like other soft tissue sarcomas, imaging findings in rhabdomyosarcoma may be nonspecific. Sclerotherapy is the mainstay of remedy for big macrocystic or combined lesions. Injection of a sclerosing agent corresponding to ethanol, bleomycin, or doxycycline after aspiration, induces scarring of the cyst wall and shrinkage of the lesion.
Cheap chloramphenicol 250 mg free shippingChapter 39 � Candidiasis 437 Invasive and Deep-seated Candidiasis Candida species are the third to fourth most frequent cause of late-onset sepsis in premature infants infection borderlands 2 best purchase chloramphenicol. The diploma of prematurity (ie, low gestational age, low birthweight) is the most important issue associated with elevated incidence of candidiasis. Candidemia could also be adopted in as a lot as 25% by hematogenous meningoencephalitis and in a much higher share (up to 60%) by urinary tract an infection. Other syndromes which will complicate candidemia in neonates include endocarditis, brain or other organ abscesses, arthritis/osteomyelitis, and renal an infection. Other threat factors are fungal colonization, excessive glucose concentrations, antibiotic and H2-receptor antagonist use, endotracheal intubation, congenital circumstances, and necrotizing enterocolitis. The clinical syndromes that Candida causes in older kids are just like these in adults. Candida species are necessary causes of health care�associated infections in pediatric cancer sufferers receiving remedy for hematologic malignancies, pediatric allogeneic hematopoietic stem cell transplant recipients, and youngsters and adolescents with indwelling central venous catheters. Invasive candidiasis can be a clinically necessary syndrome in strong organ transplant recipients. Acute disseminated candidiasis with hemodynamic and inflammatory indicators of sepsis, in addition to a attainable characteristic erythematous papular exanthema, may comply with candidemia. Candida glabrata and C tropicalis are more frequent in kids with hematologic malignancies than in other sufferers, probably because of the elevated use of azoles and amphotericin B, respectively, in these sufferers. The attributable mortality of invasive candidiasis has been estimated to be round 10% in youngsters. Chronic disseminated candidiasis (hepatosplenic candidiasis) is a welldescribed syndrome that happens in youngsters with hematologic malignancies 438 Succinct Pediatrics during and after restoration from neutropenia. It is characterised by persistent fever and upper stomach ache in addition to increased inflammatory index, alkaline phosphatase, and -glutamyltransferase levels, but not transaminase. The illness can last comparatively long regardless of appropriate antifungal remedy and is set by an ineffective inflammatory response. Organ- or Tissue-Specific Candidal Infections Meningoencephalitis frequently occurs in neonates following about as many as 25% of episodes of neonatal candidemia. In untimely neonates, candidal meningoencephalitis could additionally be followed by calcifications and neurodevelopmental delay. Chorioretinitis and endophthalmitis happen as a comparatively infrequent complication of candidemia, especially when antifungals with suboptimal eye penetration are used, such as echinocandins. Funduscopy can reveal the characteristic image of chorioretinal infiltrates and purulent vitreous opacity, respectively. Endocarditis happens in 5% of sufferers with candidemia and presents as persistent fever with refractory candidemia and usually large coronary heart vegetations shown at echocardiography of the guts. Urinary tract an infection can present as cystitis, pyelonephritis, or fungal balls within the kidneys. Fungal balls are normally refractory to antifungal therapy and in some refractory cases might require surgical procedure. Peritoneal fluid neutrophil count is elevated, and its culture may be positive for Candida species. Osteoarticular infections are comparatively rare infections occurring in neonates and less incessantly in children. In neonates, Candida can infect the bone and joint simultaneously (osteoarthritis), and the an infection is almost all the time hematogenous. In older kids, an infection occurs either hematogenously or by way of contiguous spread of the organism, and it can be both osteomyelitis or arthritis. A current large series of candidal bone and joint infections also involves a comparatively giant variety of neonates and children. The most frequent bones affected are femur, humerus, and then vertebra/ribs, whereas the joints incessantly affected are knee, hip, and shoulder. Spondylodiscitis is a particular form of osteomyelitis that requires notably careful surgery at the facet of antifungal therapy. Chapter 39 � Candidiasis 439 Evaluation Microscopy and tradition of appropriate specimens stay the criterion standards of mycologic prognosis. Successful management of invasive candidal infections relies on early recognition and rapid initiation of efficient remedy. However, a optimistic blood tradition ought to by no means be thought of as contamination, and the patient should obtain antifungal remedy. This is an indication of candidal an infection, but tradition is the method that yields the definitive prognosis. It is important to note that not all yeast-like organisms in the bloodstream are Candida species. Trichosporon and Cryptococcus species are yeasts however have completely different susceptibility profiles and require totally different treatment methods. As a rapid test for presumptive identification of C albicans (and, occasionally, C dubliniensis), germ tube take a look at may be performed. C albicans is germ-tube optimistic, whereas different common non-albicans Candida species are adverse. Testing of susceptibility to antifungals is important, particularly for strains isolated from sterile websites that are non-albicans. Non�culture-based strategies for diagnosing invasive candidiasis, such because the assay for (13) -D-glucan assay and polymerase chain response, may be available to be used. It often is a challenge to distinguish floor colonization, such as candiduria and constructive endotracheal tube secretions, from invasive illness. In the case of candiduria, consideration of the host immune standing, such as neutropenic, deeply immunocompromised, and neonatal; elimination of a urinary catheter and repeat urinary culture; ultrasound of kidneys; and blood cultures must be tried to determine whether candiduria is a sign of invasive disease. Similarly, interpretation of candidal development in endotracheal tube secretion cultures requires consideration of the immune standing of the host, as nicely as seek for lung opacities and other indices of lung irritation. Ultrasound of heart, liver, spleen, kidneys, or neonatal mind is a very useful and simple diagnostic tool and yields reliable outcomes. Finally, radionuclide scanning, corresponding to technetium scan and leukocyte indium scan, is useful for diagnosing troublesome and multiple organ cases. Important considerations when selecting the antifungal and mode of utility embody localization of the an infection, severity of the disease, impairment of liver and renal features, previous current exposure to antifungals, recognized Candida species, and native or institutional patterns of resistance. Antifungals Currently, there are four available classes of antifungals: polyenes, triazoles, echinocandins, and flucytosine (Table 39-1). The obtainable polyenes embrace nystatin, conventional amphotericin B deoxycholate, and lipid formulations, similar to liposomal amphotericin B and amphotericin B lipid complicated. All amphotericin B preparations are fungicidal and effective against most Candida species, with the possible exception of Candida guilliermondii and C lusitaniae. For many years, amphotericin B deoxycholate has been the cornerstone of antifungal remedy; however, its use is restricted by renal and infusionrelated toxicities. The lipid formulations show much less nephrotoxicity than amphotericin B deoxycholate, while infusion-related adverse effects such as fever, chills, and rigor are considerably much less with liposomal amphotericin B solely.
References - Jakobsen H, Steven K, Stigsby B, et al: Pathogenesis of nocturnal urinary incontinence after ileocaecal bladder replacement. Continuous measurement of urethral closure pressure during sleep, Br J Urol 59:148n152, 1987.
- Robbins J, Levine RL. Swallowing after unilateral stroke of the cerebral cortex; preliminary evidence. Dysphagia 1988; 3:11-17.
- Nelson JA, Loredo JS, Acosta JA. The obesity-hypoventilation syndrome and respiratory failure in the acute trauma patient. J Emerg Med. 2011;40:e67-e69.
- Cheung AT, Savino JS, Weiss SJ, et al: Echocardiographic and hemodynamic indexes of left ventricular preload in patients with normal and abnormal ventricular function, Anesthesiology 81:376, 1994.
- Bukoski A, Winter M, Bandt C, et al: Comparison of three intraosseous access techniques in cats. J Vet Emerg Crit Care (San Antonio) 20:393-397, 2010.
- Solaro RJ, Van Eyk J: Altered interactions among thin filaments proteins modulate cardiac function, J Mol Cell Cardiol 28:217-230, 1999.
|


