|
Dr Craig Davidson - Director Lane Fox Respiratory Unit
- Guys & St Thomas� Foundation Trust
- London
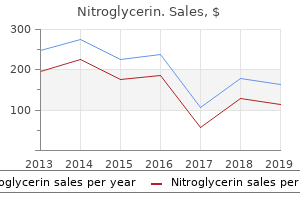
Nitroglycerin dosages: 6.5 mg, 2.5 mg
Nitroglycerin packs: 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps

Buy nitroglycerin 6.5mg amexEach order is duplicated so one set of clothes may be worn while the opposite is being washed medications affected by grapefruit discount nitroglycerin express. Today, pressure garment companies provide multiple colours of materials and, for the pediatric population, cartoon characters could additionally be sewed on the garments to make them cosmetically appealing and improve patient compliance. These places embody concave physique areas such as the face, neck, antecubital fossae, sternum, palm of the hands, internet areas, upper again, and arches of the toes. These materials come commercially prefabricated or could also be custom-made by the burn therapist. Inserts come in different varieties, corresponding to silicone/nonsilicone gels or gel sheets, elastomers, putties combined with a silicone catalyst, skincare silastic pads, foam, and even within the type of hard thermoplastic materials contouring to completely different anatomical places. The skilled burn therapist chooses the suitable insert materials best suited to the affected person in accordance with the stage of scar maturation and pores and skin sensitivity. Generally, strain therapy begins with a soft, thin, and elastic insert and progresses to a extra rigid insert in miserable the extra unyielding burn scar. Inserts have to be worn beneath pressure clothes, beginning with a number of hours of application and progressing as tolerated toward a 23-hour application. In instances of scar maceration, blisters, pores and skin breakdown, contact dermatitis, a rash, or an allergic response, inserts must be eliminated instantly until healing occurs. Silicone, a polymer primarily based on the component silicon, seems to be the pattern in the therapy of hypertrophic scars. Clinically, silicone has been noticed to depress the height of hypertrophic scars, prevent shrinking of fresh pores and skin grafts (hard elastomer silicone pads vs. Silicone, being occlusive, might cause the gathering of excessive moisture and cause pores and skin maceration if not eliminated regularly for cleansing and drying. Other insert materials embrace liquid silicone elastomer, which when mixed with a catalyst varieties a stable however elastic insert. The experienced therapist is ready to create customized inserts for difficult anatomical areas such because the face and net areas using this technique. Prosthetic Foam is a liquid-based silicone elastomer which, when combined with a catalyst, solidifies in the type of a really pliable foam insert that works greatest for the palm of the palms, where. These foam inserts additionally work best for making use of strain to contour surfaces on the face (around the eyes, mouth, and nose) while defending these sensitive areas from excess and inflexible stress. Elastomer putties similar to Otoform K or Rolyan Ezemix kind semi-rigid but still elastic inserts for different areas of the physique where the scar can tolerate extra stress, such as within the internet areas to prevent syndactyly. These masks require the moulaging of the affected person in creating a adverse facial mildew. A high thermoplastic material corresponding to Uvex or W-Clear is then pulled over the optimistic mould to create the clear face orthosis. The clear face orthosis is worn with various harness methods designed to safe it to the face to tackle facial scar management. The scan is sculpted on a pc and a constructive software is manufactured out of foam off-site. In the previous, scanners were so giant that facilities had to dedicate a complete room to their use; today, scanners are sufficiently small to fit in a conveyable case and are run by laptops. These newer portable scanners give a therapist the freedom to scan sufferers in any setting in the hospital together with intraoperatively. In instances of serious scar hypertrophy on the face, the constructive mould is sculpted sequentially over a time frame to keep away from extreme strain over facial scar that might result in pores and skin breakdown. A silicone elastomer face mask could additionally be created utilizing the present optimistic facial mold and is worn underneath facial stress clothes t. The use of the clear and silastic masks is preferred over the use of only a facial garment as a end result of these masks provide conforming stress round facial openings (eyes, nostril, and mouth). Frequently, the burn therapist manufactures the clear orthosis to be worn through the day and the silastic masks along with the facial garment to be worn at night. Scar therapeutic massage is an efficient modality for sustaining joint mobility in the case of contractures. It aids in softening or transforming the scar tissues by freeing adhering fibrous bands, allowing the scars to turn into extra elastic and stretchy, thus enhancing joint mobility. Initially, the therapist may make the most of a nonfrictional therapeutic massage making use of largely stationary strain to skin blanching and mobilizing the pores and skin surface without friction. As the skin begins to tolerate frictional massage, the scar tissue is manipulated in circular, parallel, and perpendicular motions, utilizing a lubricant and mobilizing the skin to blanch when performing the desired technique. An electrical massager with a heat attachment may be used together with lubrication as a result of heat and massage in combination might improve scar pliability. Massage ought to be carried out no less than twice day by day; the advice is three to five times every day for 5�10 minutes on each handled physique surface. The burn therapist should incessantly assess the skin situation to avoid further injuries. The patient and/or household are instructed on home massage strategies, and electrical massagers may be issued for residence use. To lower the consequences of scar tissue, a burn therapist must make the most of all obtainable choices to obtain a functional consequence. Application of warmth may allow simpler elongation of scar tissue by way of increased extensibility of connective tissue. Heat modalities may embody sizzling packs, paraffin wax, fluidotherapy, and ultrasound. Even though using therapeutic heat as an adjunct to rehabilitation is welldocumented, therapeutic warmth modalities are infrequently utilized in burn rehabilitation. Patients might not have the flexibility to tolerate heat over areas of healed or grafted burns because of hypersensitivity. Conversely, patients with diminished sensation are unable to decide if the temperature is suitable and are at risk for additional injury. Although warning needs to be taken, the usage of therapeutic warmth in burn patients can present an efficient method for growing burn scar extensibility. The use of passive stretch at the aspect of therapeutic warmth greatly increases the effectiveness of the therapy. Because of the shallow depth of heat penetration, scorching packs may have little effect on deeper layers of scar tissue. Reported advantages of ultrasound in the remedy of burn scar include increased extensibility of collagen tissue, increased blood flow, and elevation of pain thresholds. Heated paraffin encourages collagen extensibility and may also be helpful because of the softening of the scar by the mineral oil within the paraffin. Extensive coaching should happen addressing the use and care of pressure garments, inserts, lubrication, and different therapeutic scar administration procedures to be performed by sufferers and their caregivers. Follow-up visits to the burn or rehabilitation clinic for the evaluation of general recovery, together with clothes, inserts, and different residence therapeutic interventions, are wanted so that the patient might successfully complete his or her burn rehabilitation during the first two years after the damage. Therapeutic exercise is outlined as scientific supervision of bodily movement with or without equipment, for the purpose of restoring regular perform to diseased or injured tissues. Exercise is initially painful, and the very first repetition is usually probably the most tough.
Diseases - Infantile axonal neuropathy
- Neuronal intranuclear hyaline inclusion disease
- Diaphragmatic agenesia
- Cataract, congenital ichthyosis
- Phosphoglucomutase deficiency type 1
- Rambaud Galian syndrome
- Attenuated FAP
- Ackerman syndrome
- Stargardt disease
Buy nitroglycerin 6.5mg on lineThe pulse width or period of the laser pulse have to be inside the thermal leisure time of the treated tissues treatment authorization request order nitroglycerin 2.5mg visa. Thermal rest time is the amount of time it takes to transfer two-thirds of the resultant warmth to the surrounding tissues. Nonablative lasers will thermally injure the tissue, whereas ablative lasers will destroy whole columns of tissue, including dermis. Children may require basic anesthesia, whereas adults can be treated with topical anesthesia. The use of topical anesthetic as a part of multimodal analgesia for fractionated laser therapy of burn scars significantly decreases the requirement for opioid analgesia and reduces procedure to discharge instances. Patients present process fractional ablative laser are routinely washed with chlorhexidine and totally dried prior to initiation of laser treatment. All patients receiving fractional ablative laser to the face are given acyclovir for herpes simplex prophylaxis. Wound care after laser therapy is initiated on the primary postoperative day and features a topical antiseptic wash and application of a beneficiant amount of emollient for a quantity of days. Hydrocortisone 1% cream can be offered to these patients present process fractional laser remedy to assist with itching. Analgesia is usually achieved with over-the-counter ache medications; nevertheless, some sufferers might require a short course of narcotic medication. Patients may resume regular activity nearly immediately, including bodily or occupational therapy. Depending on the discomfort stage and the specified sort of exercise, patients might return to college or work after 1�3 days. Overview of Lasers in Hypertrophic Burn Scar the final word aim in the treatment of hypertrophic scars is to make improvements both aesthetically and functionally, in addition to reduce itching and ache related to the scars. Traditional and emerging laser- and light-based applied sciences provide new hope for sufferers with burn scars. Although the mechanism of action for scar improvements is unknown, most theories are based on the principle that vascular proliferation plays a key role in hypertrophic scars. The kind of anesthesia employed previous to laser therapy is dependent upon several components, including the mode of laser remedy. Similar to a z-plasty, the laser breaks up the thick, disorganized collagen fibrils that created the scar, permitting these regions to repair in a extra organized trend. However, a major quantity of dermis and dermis stays intact, which assists in wound therapeutic. Fractional laser damage has additionally been shown to induce a molecular cascade including heat shock proteins and matrix metalloproteinases as well as inflammatory processes that lead to a speedy healing response and prolonged neocollagenesis. Two further studies additionally investigated 1540-nm nonablative fractional erbium laser in mature burn scars and found an identical lack of enchancment in thick scars. There is a considerably larger potential depth of thermal injury with ablative fractional laser in comparison with nonablative fractional laser gadgets (approximately four. One examine cited improvement in hypertrophic burn scars in 24 patients on face, neck, or low neckline, and eight on the hands. Improvement of tactile sensation after treatment of burn scars of the palm has additionally been reported. The device generates tons of of very deep microchannels that penetrate up to 4 mm. Usually after the first procedure patients feel a reduction of pressure and softening of the scar. A lengthy pulse is used for hair removing (by destroying hair follicle stem cells) and ultra brief (nano-second) pulse for interfollicular and follicular melanocyte destruction. This creates a broad spectrum of various wavelengths to enable targeting of different pigments and depths of melanocytes. They are thus helpful for the removing of pigmentation and pigmented hairs to treat burn scar folliculitis. Indications included hypertrophic scar, contracture bands, unstable or thick, cracked scars. The Ruby laser was used for 30 (15%) of procedures alone and fifty one procedures in whole, with indications being hyperpigmentation and folliculitis. This allows the relief of tissues, enabling release of pores and skin across the neck and in the webspaces of the hand. Folliculitis Commonly, hair becomes trapped underneath scars or grafts causing irritation and repeated localized infections, this might be significantly problematic in the beard space of men. Following this a laser targeted at pigment (in this case Alexandrite laser) is used to remove the hair. Patients should be comprehensively consented, as the laser will cause hypopigmentation which can be equally distressing. Occasionally skin blistering or crusting may occur in the early posttreatment section. Hypo- or hyperpigmentation may also happen, especially in patients with darker skin types. Overtreatment of burn scars could induce scarring exacerbation, especially in skin with darker pigmentation, in which melanin acts as a competing chromophore. Postoperative topical application of ascorbic acid has been proven to decrease the duration in addition to the severity of erythema. Patients with a historical past of herpes who bear laser remedy across the face might experience an outbreak if not pretreated as discussed earlier in the chapter. These regulations determine the licensing requirements for who can operate a laser under the supervision of a doctor. The greatest danger when operating a laser is that of eye harm to either the medical personnel or the affected person. The protecting specs (wavelengths and optical densities) are normally printed on the goggles, generally near the top of the unit. Protective eyewear must also be positioned on the door(s) exterior the laser operating room in case emergency entrance is required. To assist prevent eye injury, laser procedures ought to be restricted to dedicated rooms which are clearly labeled and solely permit the necessary personnel. However, if the procedure is being carried out below the neck, burnished stainless-steel eye cups are fitted over the eyelids and secured so that the complete periorbital space is roofed. The sign should describe the character of the laser getting used, its wavelength, and energy. Signs should solely be posted when the laser is in precise use and removed or covered when the laser is turned off and the vital thing removed. Lasers that have foot pedals are useful in allowing expeditious use of the laser.
Discount nitroglycerin 2.5 mg onlineImplementation of the plan is the next step medications 1040 order 6.5 mg nitroglycerin overnight delivery, adopted by an intensive analysis of the effectiveness of learning and/ or willpower of whether the educational goal is being achieved. Alterations within the unique plan could additionally be needed at any time during the academic course of relying on unexpected situations or unanticipated modifications in circumstances. This process ensures communication of educational subjects among the team members, provides a historical account of training, and paperwork progress and/or adjustments in the plan. It benefits the patient and family by making them competent of their position as care supplier when discharged from the hospital. Knowledge allays anxiety in regards to the unknown and aids in compliance with really helpful care after discharge, thus improving the long-term outcomes. Rehabilitation of the Burn Patient A major burn is certainly one of the most devastating injuries, each physically and emotionally, known to man. After weeks of being an invalid, present process repeated surgical procedures, preventing infection, having the body ravaged by the metabolic consequences of injury, and enduring pain and anxiety, the patient now faces months of continued physical remedy to regain the extent of function that he or she had identified before the injury. In addition, these patients incessantly turn into depressed as they face an altered self-image and a pressured bodily dependence on others. Although nurses have been very involved within the care of the patient in the early phases of care, the position of the nurse modifications at this stage. The transition from the hospital to residence care is commonly tough for each the affected person and family. It is important prior to discharge that the patient and family be educated within the care of open wounds, healed skin, itching, ache, and anxiousness before they depart the hospital. This is where the nurse case manager turns into an integral part of the affected person care team. Hospitalbased nurse case managers can begin to work with the Patient and Family Education In order for nurses to be competent teachers, they should be competent practitioners with stable theoretical foundations. Continuing education to maintain competency is vital for medical workers because of their position as educators of patients and households. Reinforcement of the academic process (assess, plan, implement, consider, and document), characteristics of patient populations, updates on instructional strategies, age-appropriate interventions, and methods to evaluate learning are subjects that can sharpen educator competency. Identifying data deficits and barriers to training, prioritizing methods for schooling, and offering supplemental instructional handouts and/or classes, as properly as growing a plan for evaluating the effectiveness of the instructing opportunity are integral elements of the tutorial course of. Assessment supplies essential info for planning an academic program to meet the precise individual needs of every patient and family. It can be done periodically throughout different levels of the tutorial process to determine if the plan remains valid or adjustments have to be made. The evaluation findings turn into a part of the tutorial plan in that the plan is tailored to meet the needs and considerations of the patient and family. The plan contains the training goals, methods for training, and studying t. Coordination of activities between case managers is essential to present seamless care. Although the rehabilitation therapist performs an important role in providing referrals to group therapists and psychologists, and social staff incessantly make referrals to neighborhood mental health providers, the nurse case supervisor should be involved within the overall coordination of these and different providers to foster a unified strategy. The free move of communication amongst all providers is important for optimum rehabilitation of the affected person. Implementation Once the details are labored out, the subsequent hurdle is to get buy-in from the affected person and household. Some programs require the affected person to be in a facility far from the house; this may present issues for each the patient and family. Similarly if the program is in the space people, every day visits to the rehabilitation facility may pose transportation points, especially if the patient is unable to transport him- or herself. These details can normally be worked out with cooperation of all caregivers and the household involved. The nurse case supervisor may be very instrumental in rallying the burn team and caregivers in the community to help the affected person and household to see this as a method to return the patient to more regular perform. Evaluation Success in such applications requires that each one concerned have the same goals and that these goals lead to measurable outcomes. The main concern for the nurse case supervisor and the burn team is early identification of which sufferers want these packages and at what level the affected person will benefit most from such intensive applications. Assessment Burn sufferers, like those recovering from coronary coronary heart illness and surgery, discover themselves deconditioned. Even 3 weeks of bedrest in a healthy subject can end result in a 25% decrease in maximal oxygen consumption. Burn sufferers must be first assessed for risk factors associated with coronary heart illness. This can make it tough for the child to return to school, where she or he should be alert and attentive for 6�8 hours a day. Younger children be taught much about their setting and world via play and varied actions. Limitations in motion from burn scars or low vitality could decrease their rate of studying. Also, children learn much about socialization by way of their participation in sports actions. Physical limitations in sports activities could present a sort of isolation from their normal group of peers. If the affected person has a number of Assessment Children and their household situation must be evaluated to decide what exercise program is greatest for their burn t. Generally, kids 7 years of age and older can participate in an intensive train program. The program can start immediately after discharge or may be delayed for a quantity of months to enable the household to return house and put together for the subsequent phase of intensive exercise rehabilitation care. This may be a big factor in when the patient is in a position to begin such a program. For children youthful than 7 years of age, extra artistic interactive play and train packages have been developed utilizing music therapy as a stimulus for youngsters to take part within the exercise program. These activities can embrace using tricycles, playing sports games, obstacle programs, racing, dancing, stretching, and any activity that could be made right into a game that promotes strength and endurance. The use of actions set to music can enhance stamina, actively stretch scar tissue, and improve joint mobility. Helping the father or mother see this as a useful program would require the entire burn staff to work together with the patient and household. Alternatives could additionally be obtainable for older children throughout the community by utilizing local gyms or health centers. Communicating a prescription for exercise to the local facility and maintaining regular follow-up of progress may be as effective as having the patient stay within the bigger hospital system. Evaluation the end result of those programs for the child can be measured in increased train tolerance and improved psychological and social adjustment. A major operate of these programs is to convince the kid and father or mother that the patient is a normal baby and can succeed mentally and physically. The nursing role of patient advocate may be crucial for the affected person and family.
Cheap 6.5mg nitroglycerin amexThis giant adverse interstitial hydrostatic stress constitutes a strong "suction pressure" or imbibition pressure promoting microvascular fluid filtration and sustained burn wound edema medicine 4839 discount generic nitroglycerin uk. In vivo measurements present a temporary discount of -20 to -30 mmHg; the less negative Pif in vivo is as a end result of of the continued tissue perfusion and fluid extravasation that relieves the imbibition stress. Kinsky30 reported a continued negative stress offering a partial explanation for the sustained edema in the course of the first 4 hours submit damage. The mechanism for the big lower in Pif is due, at least partially, to the release of cellular tension exerted on the collagen and microfibril networks in the connective tissue by way of the collagen-binding 1-integrins. The integrins are transmembrane adhesion receptors that mediate cell�cell and cell�matrix adhesion, thereby allowing the glycosaminoglycan ground substance, which is normally underhydrated, to expand and take up fluid. This helps the mechanism of interfascial rather than colloidal osmotic fluid transfer as a mechanism for burn edema and supports the collagen structural transitions as therapeutic targets. Arturson and Mellander27 showed that, in the scalded hindlimb of canine, Kf instantly increased two to thrice, suggesting that the hydraulic conductivity (water permeability) of the capillary wall elevated. Thus local vasodilation and microvascular recruitment contribute to the increased Kf along with elevated hydraulic conductivity. Measuring Kf and the speed of edema formation (Jv) allowed Arturson and Mellander to decide the changes in transcapillary forces necessary to account for the elevated capillary filtration. Their calculations indicated that a transcapillary strain gradient of 100�250 mm Hg was required to explain the extremely fast edema formation that occurred within the first 10 minutes after a scald damage. They concluded that only a small fraction of the early formation of burn edema could be attributed to the adjustments in Kf and permeability. They additional suggested that osmotically active molecules generating sufficiently large osmotic reabsorption pressures are launched from burn-damaged cells. This hypothesis was never confirmed, and subsequent studies described herein present that giant will increase in filtration forces result from an elevated Pc, and from a big lower in Pif (Table 8. The reflection coefficient is traditionally attributed to the endothelial cellular junctions however might be primarily decided by the glycocalyx. Lymph sampled from burned skin has shown elevated protein concentrations in keeping with the big and sustained will increase in capillary permeability,14,34,35 whereas a transient and smaller increase in microvascular permeability happens over 8�12 hours following injury in other gentle tissue not directly burned. The osmotic reflection coefficient, decreases with burns but never equals zero; thus protein concentration in capillary filtrate is all the time less than in plasma even in burn-injured skin. Several clinical and animal research have established that sustaining higher levels of whole plasma protein concentration can ameliorate the general web fluid retention and edema. These scientific data assist experimental findings on endothelial dysfunction after burn harm. Plasma is additional diluted and p is further reduced after crystalloid resuscitation. Increased fluid filtration is less as a outcome of the fall in p and more doubtless attributed to elevated Kf and reductions in Pif and as a result of a damaged glycocalyx. Many of those changes in endothelial and interstitial function may be attributed to the glycocalyx-a glycoprotein and polysaccharides layer on the luminal aspect of endothelial cells that maintains the barrier between the endothelium and plasma by reducing the osmotic gradient and thereby decreasing filtration. The thickness of the glycocalyx varies from 20 nm in capillaries to 3000 nm in bigger vessels. Based on research of the glycocalyx, the paradigm of the traditional Starling equation of microcirculatory forces has been challenged, and a revised equation has been proposed. Levick and Michel, together with others, proposed the revised Starling equation proven here and in. Plasma colloid osmotic stress decreases in nonresuscitated burn-injured animals as protein-rich fluid extravasates into burn wounds and a big quantity of protein-poor interstitial fluid initially enters the circulation from transvascular reabsorption and lymph of unburned tissue, corresponding to skeletal muscle. Increased fluid filtration is less because of the autumn in p and extra likely attributed to elevated Kf, reductions in Pif and due to a broken glycocalyx. Initial remedy with colloid answer has all the time been advocated by some clinicians6 but is commonly delayed 8�24 hours after damage primarily based on the reasoning that normalization of microvascular protein permeability in injured tissue must happen before colloid remedy is value efficient. Evidence for the use of albumin for resuscitation can additionally be lined in Chapter 9 on burn resuscitation. Maximum elevated lymph circulate and tissue water content had been observed to correlate with the extreme hypoproteinemia that occurred during the early resuscitation interval of a 40% burn harm in sheep. This mannequin allows testing of the consequences of assorted inhibitory and therapeutic brokers in ameliorating the resultant physiologic derangements. High-dose vitamin C, an antioxidant, administered to the recipient rat was discovered to considerably cut back capillary leakage but not leukocyte-endothelial interactions. Unburned Tissue Generalized edema in gentle tissues indirectly injured is another characteristic of huge cutaneous burns. Arturson reported an increased transvascular fluid flux (lymph flow) from unburned tissue and a transient enhance in permeability as measured by an increase within the lymph concentration of plasma protein and macromolecular dextran infused as a tracer. They discovered that pores and skin and muscle permeability (flank lymph from sheep) were elevated for up to 12 hours postburn for molecules the scale of albumin and immunoglobulin G, but the In addition to a lack of microvascular barrier integrity, thermal damage additionally causes adjustments in the mobile membrane. In skeletal muscle mobile transmembrane potentials lower at sites distant from the harm. Micropuncture techniques in hemorrhaged animals have demonstrated partial depolarization in the skeletal muscle membrane potential of -90 mV to levels of -70 to -80 mV; cell death occurs at -60 mV. These shock-induced decreases in membrane potentials are associated with will increase in intracellular water and sodium. Encephalopathy, muscle weakness, impaired cardiac contractility, and intestine dysfunction are related to major burn harm and may be due partly to decreased membrane potentials. Furthermore, the depolarization may be reversed by altering the superfusate to regular plasma or saline. Very little is understood about the time course of the adjustments in membrane potential in medical burns. Furthermore, we have no idea the extent to which the altered membrane potentials affect complete volume requirements and organ perform in burn harm. Histamine and its metabolic derivatives elevated the catalytic activity of xanthine oxidase in rat plasma and in rat pulmonary artery endothelial cells. Burn edema was tremendously attenuated by treating rats with the mast cell stabilizer cromolyn, complement depletion, or the H2 receptor antagonist cimetidine but was unaffected by neutrophil depletion. Inflammatory Mediators of Burn Injury Many local and circulating mediators are produced in the blood or released by cells after thermal harm. These mediators play essential but complicated roles within the pathogenesis of edema and the cardiovascular abnormalities of burn damage. For example, mediators alter vascular permeability and transvascular fluid flux, either directly or indirectly, by rising the microvascular hydrostatic stress and floor space via the arteriolar vasodilation superimposed on an already injured endothelial barrier. The actual mechanism(s) of mediator-induced damage are of considerable scientific curiosity because this understanding would enable for the event of pharmacologic modulation of burn edema and shock by mediator inhibition. Unfortunately most methods directed at mediator blockage have solely been efficient in small localized burn wounds in sufferers or in animal research and have had no scientific impact on the care of patients with main burns. LaLonde83 showed that topically applied ibuprofen (which inhibits the synthesis of prostaglandins and thromboxanes) reduces both native edema and prostanoid production in burned tissue with out altering systemic production. Histamine is launched from mast cells in thermally injured skin; nevertheless the rise in histamine levels and its actions are only transient.
Amomum zedoaria (Zedoary). Nitroglycerin. - How does Zedoary work?
- Colic, spasms, improving appetite and digestion, inflammation, nervous diseases, and other uses.
- Are there safety concerns?
- Dosing considerations for Zedoary.
- What is Zedoary?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96355
Cheap nitroglycerin 6.5mg amexProteoglycans are fashioned by a protein core treatment bulging disc purchase nitroglycerin 2.5 mg amex, usually with repeating units similar to leucine in decorin, and glycosaminoglycan facet chains. Decorin binds to collagen fibrils, controlling their diameter, morphology,16 and interfibrillar distance. Biglycan is 57% similar to decorin in amino acid sequence but with two dermatan sulfate chains and is believed to have originated as a gene duplication of decorin. Numerous studies have demonstrated that dermal fibroblasts may be divided into distinct subpopulations-superficial (papillary) and deep (reticular)-based on each bodily location and phenotype. In this mannequin, deep dermal fibroblasts closed wounds and superficial dermal fibroblasts then transformed them. Proto-myofibroblasts evolve, however not necessarily at all times, into the differentiated myofibroblast. The resulting Ca2+ influx induces a contraction that can feed again on the first cell and/or stimulate different contacting cells, working like a syncytium. This mechanism might improve the reworking of cell-dense tissue by coordinating the activity of myofibroblasts. The myofibroblast modulation of fibroblastic cells begins with the looks of the proto-myofibroblast, whose stress fibers contain only - and -cytoplasmic actins and evolves, however not essentially all the time, into the looks of the differentiated myofibroblast, the commonest variant of this cell, with stress fibers containing -smooth muscle actin. The myofibroblast can endure apoptosis; the deactivation resulting in a quiescent phenotype has not been clearly demonstrated a minimum of in vivo. In vivo, covering granulation tissue through the use of carbon tetrachloride treatment, chemical denervation considerably reduces matrix deposition and myofibroblast differentiation. When myofibroblasts beforehand cultured in plastic dishes are incorporated in a floating collagen gel, a excessive proportion quickly undergo apoptosis (arrows). In contrast, when integrated in an connected collagen gel, they show a typical elongated morphology, specific high quantities of -smooth muscle actin, and proliferate. The majority of these cells originate from native recruitment of connective tissue fibroblasts. For instance, in pores and skin, dermal fibroblasts located in the edges of the wound can acquire a myofibroblast phenotype and participate in tissue restore. These progenitor cells have been described within the dermal sheath that surrounds the outside of the hair follicle going through the epithelial stem cells, constituting a niche of stem cells. They are involved within the regeneration of the dermal papilla and also can turn into wound healing (myo) fibroblasts after an harm. These mesenchymal stem cells are bone marrow-derived nonhematopoietic precursor cells89,ninety that contribute to the maintenance and regeneration of connective tissues through engraftment. In normal tissue repair, myofibroblasts disappear by apoptosis during the transition between granulation tissue and scar. In pathological conditions, myofibroblasts proliferate and take part in the extreme deposition of extracellular matrix. In all these conditions, not solely interaction between fibroblasts/myofibroblasts and extracellular matrix, but also the dialogue between epithelial cells and mesenchymal cells play a major position. Wound restore and regeneration: mechanisms of pathological scarring: role of myofibroblasts and present developments. In hypertrophic scar nodules myofibroblasts specific large quantities of -smooth muscle actin (A,B, immunohistochemistry for -smooth muscle actin) and develop big contractile activity in scars after burn injury (C,D) (From Desmouli�re A; C,D are from Casoli P, Plastic Surgery and Burns Unit, University Hospital of Bordeaux, France. However the degree to which this process contributes to fibrosis and stroma response within the skin remains a matter of intense debate and is prone to be context dependent. Like leukocytes, fibrocytes can act as antigen-presenting cells to prime na�ve T cells104 and in addition specific Toll-like receptors, allowing them to operate as a part of the innate immune system. Various cell sorts can purchase a myofibroblast phenotype; these various origins result in distinct myofibroblast subpopulations. The fibrogenic and antifibrogenic elements that modulate fibroblast function throughout wound therapeutic. The Role of Cytokines in Hypertrophic Scar Cytokines serve as alerts for communication between cells, in paracrine signaling, and for cells to signal themselves in autocrine signaling. The Immune System Regulates Wound Healing Mast cells, neutrophils, and macrophages have lengthy been acknowledged as taking part in essential roles in the inflammatory part of wound therapeutic. Cytokine manufacturing by lymphocytes from burn sufferers as a operate of time after damage. Hypertrophic scar, keloids and contracture: the mobile and molecular foundation for remedy. This leads to a mass of disorganized connective tissue with skinny, irregular collagen bundles in whorls and nodules instead of thick, organized fibers parallel to the floor. It is our hope that this will provide therapies to enhance the standard of life for each burn patients and others with fibroproliferative circumstances. Transforming growth factor-beta stimulates the expression of fibronectin and collagen and their incorporation into the extracellular matrix. Identification of circulating fibrocytes as precursors of bronchial myofibroblasts in bronchial asthma. Chemical characterization and quantification of proteoglycans in human post-burn hypertrophic and mature scars. Proteoglycans of the extracellular environment: clues from the gene and protein facet offer novel perspectives in molecular range and performance. Decorin regulates assembly of collagen fibrils and acquisition of biomechanical properties throughout tendon growth. Decorin core protein (decoron) shape enhances collagen fibril floor construction and mediates its binding. Targeted disruption of decorin results in abnormal collagen fibril morphology and skin fragility. Decorin evokes protracted internalization and degradation of the epidermal progress factor receptor through caveolar endocytosis. Transient transgene expression of decorin within the lung reduces the fibrotic response to bleomycin. Mice deficient in small leucine-rich proteoglycans: novel in vivo models for osteoporosis, osteoarthritis, EhlersDanlos syndrome, muscular dystrophy, and corneal illnesses. Versican is expressed in the proliferating zone in the dermis and in affiliation with the elastic network of the dermis. Human dermal fibroblast subpopulations; differential interactions with vascular endothelial cells in coculture: nonsoluble factors within the extracellular matrix influence interactions. Scarring occurs at a crucial depth of skin injury: exact measurement in a graduated dermal scratch in human volunteers. Wound healing of human pores and skin transplanted onto the nude mouse after a superficial excisional damage: human dermal reconstruction is achieved in several steps by two different fibroblast subpopulations. Apoptosis mediates the decrease in cellularity through the transition between granulation tissue and scar. Transforming development factor-beta 1 induces alpha-smooth muscle actin expression in granulation tissue myofibroblasts and in quiescent and growing cultured fibroblasts. Sympathetic denervation accelerates wound contraction but delays reepithelialization in rats. The compliance of collagen gels regulates remodeling progress factor-beta induction of alphasmooth muscle actin in fibroblasts. The position of matrix stiffness in hepatic stellate cell activation and liver fibrosis.
Purchase discount nitroglycerinThe autonomic dysfunction could additionally be influenced by -adrenergic antagonists symptoms 0f parkinsons disease order nitroglycerin australia, calcium-channel blockers, and low-dose diazepam or may require intravenous regional blocks and sympathetic ganglion blockade. The scientific findings may resemble upper-extremity compression syndromes or peripheral neuropathy. Cataracts may occur with out damage to the head and seem even years after injury. Long-term follow-up of these patients is recommended in accordance with the late onset of pigmentary changes at the fovea and papillomacular bundle, which can additional prevent visual improvement. Another frequent late complication of electrical burns is heterotopic calcifications in periarticular tissue of large joints, especially the elbows. Causative elements embrace compelled passive mobilization, secondary articular bleeding, and calcium precipitation and deposition in damaged or degenerating muscle and connective tissue. Particularly for electrical injury, heterotopic bone formation also occurs in amputation stumps of lengthy bones. This, as well as the common formation of bone cysts in the amputation stump, might lead to secondary pores and skin erosion, inflammation, and difficult adjustment to a prosthesis. After preliminary resuscitation, early debridement, essential decompression of neurovascular buildings, and early wound closure are important to successful restoration of operate. Extensive surgical procedures together with free soft-tissue switch could also be necessary to obtain wound closure and to save and restore limb perform. Sometimes, however, early amputation might provide simpler and earlier restoration and reintegration into day by day life. Long-term problems such as central nervous sequelae, cataracts, and heterotopic ossification should be thought of and addressed early within the rehabilitation course of. Early free tissue transfer for extremity reconstruction following high-voltage electrical burn accidents. Skeletal Injury In addition to direct tissue destruction through electrical energy, extra trauma can be not directly inflicted by electric present. Fractures occur as a result of secondary falls or with forceful tetanic muscle contractions. These are mostly seen within the shoulder,119 wrists,one hundred twenty,124,125 femurs,121,123 and spine122 and may require open reduction and internal fixation. The remedy of electrical damage in comparability with burn injury: a evaluate of pathophysiology and comparison of patient administration protocols. Angiographic findings and wish for amputation in excessive tension electrical accidents. Model of cell electrofusion: membrane electroporation, pore coalescence and percolation. A quantitative analysis of the voltage-current relationships of mounted charge membranes and the related property of `punch-through. A histological evaluation of a high-voltage electric present harm to an higher limb. A potential study of urine and serum myoglobin ranges in patients with acute rhabdomyolysis. Early predictors of myoglobinuria and acute renal failure following electrical harm. Is immediate decompression of high-voltage electrical accidents to the upper extremities at all times essential A model for recording the microcirculatory adjustments associated with standardized electrical injury of skeletal muscle. New observations on tissue changes along the pathway of the present in an electrical damage. Early adipofascial flap protection of deep electrical burn wounds of higher extremities. Salvage of the mutilated higher extremity with temporary ectopic implantation of the undamaged part. Outcome and treatment of electrical damage with instant median and ulnar nerve palsy at the wrist: a retrospective evaluation and a survey of members of the American Burn Association. The use of allografts in the management of exposed calvarial electrical burn wounds of the cranium. Cranial coverage involving scalp, bone and dura using free inferior epigastric flap. A case-matched managed study on high-voltage electrical injuries vs thermal burns. Early vascular grafting to forestall upper extremity necrosis after electrical burns. Microvascular reconstruction in burn and electrical burn accidents of the severely traumatized higher extremity. A-A kind, arterialized, venous, flowthrough, free flaps for simultaneous digital revascularization and delicate tissue reconstruction � revisited. Current ideas of microvascular reconstruction for limb salvage in electrical burn injuries. Amputation of the penis as a outcome of electrical burn � role of prefabricated urethra in penile reconstruction. Penile and upper extremity amputation following high-voltage electrical trauma: case report. Peripheral nerve compression related to low-voltage electrical damage with out related vital cutaneous burn. Local anaesthetic block protects towards electrically induced injury in peripheral nerve. High voltage electrical damage leading to a delayed onset tetraplegia, with restoration. Ocular adjustments from electrical burn injuries: a literature review and report of cases. Ocular manifestations of electrical damage: a case report and evaluate of the literature. For partial-thickness burns, short-term substitutes, in contrast to traditional wound dressings, provide a biological wound cowl that promotes therapeutic by lowering moisture loss and accelerating epithelialization. In addition, most of those merchandise (such as Biobrane, Suprathel, and amniotic membrane) are utilized only once. This is a major advantage, particularly for youngsters, as a result of it avoids the ache and associated psychological trauma of repeated wound dressing adjustments. For full-thickness excised burn wounds, short-term various substitutes can provide cowl if pores and skin grafting or software of a permanent substitute is planned as a staged procedure. In sure circumstances, to allow for a discount in wound exudate and to ensure full hemostasis, this might be delayed for 24�48 hours after wound excision in a serious burn. Due to lack of obtainable donor websites for pores and skin graft harvest, it may be determined to apply a everlasting substitute, and "take" can be optimized by staging the procedure; during this time a temporary substitute can be very helpful. Temporary substitutes are very useful for covering widely meshed pores and skin grafts (the Alexander technique). Alexander described making use of allograft on high of widely meshed autograft to present organic wound closure that protects the open wound inside the interstices (gaps) of the meshed graft. While allograft tends to adhere to the wound mattress and may in reality interfere with epithelization of the interstices, E-Z Derm dries out after a week of its software with virtually full epithelization underneath.
Nitroglycerin 2.5mg visaDespite these limitations medicine 8 letters order nitroglycerin mastercard, together with substantial price, collection from totally different burn centers have proven promising outcomes when used at the facet of allograft dermis. Donor website therapeutic is a results of migration and proliferation of the epithelial cells from hair follicles, sweat glands, and sebaceous glands inside the dermis. Early re-epithelialization after every week can enable reprocurement of thin split-thickness pores and skin grafts from donor websites. Smaller donor sites can be handled with occlusive or adherent dressings such as Opsite or Biobrane. Another method is using alginate sheets or hydrocolloid dressings, which produce a moist environment that promotes therapeutic and diminishing ache. The commonest examples are Xeroform or locally prepared dressing containing olive oil, petrolatum, lanolin, and the chemotactic agent "Sudan pink. The healing time of donor sites is dependent upon the depth of skin graft, vascularity of the donor site, wound administration, and common situation of the affected person. At our establishment, gauze impregnated with a petrolatum-based ointment and a mixture of an antibacterial (Polymyxin/Bacitracin) and an antifungal (Mycostatin) is used. This is followed by the location of a layer of fluff gauze and an elastic bandage. With areas of the physique vulnerable to shearing, such because the again and axilla, the appliance of a bolster dressing to shield the skin grafts may be beneficial. The utility of negativepressure wound therapy can also be helpful in splinting and defending the grafts. This timeframe is often enough to permit for adherence of the skin graft to the wound bed. Donor websites characterize new wounds that may add significant morbidity to the patient; sufferers often complain of extra pain at the donor website compared to the burn wound or graft web site. Whenever attainable, skin grafts should be obtained from donor sites matching the color of the recipient area. The face and neck should be grafted with pores and skin obtained from the area above the road of the nipple for the most effective colour match. Thigh, hip, and again are generally used as donor sites as a result of the skin is flat for straightforward procurement, and scars are simply covered under clothing. Good high quality pores and skin grafts of consistent depth are obtained utilizing an electrical or pneumatic-powered dermatome. The depth of the pores and skin harvest could be exactly adjusted, with thickness normally between zero. Anatomical regions which are normally spared and symbolize viable choices for skin graft are the axilla, the mons pubis, and the scrotum. Given the irregular topography, tumescent fluid can be infiltrated to facilitate skin graft procurement. Wound coverage prevents water and electrolyte losses in addition to tissue desiccation, therefore maintaining a moist surroundings that permits sooner epithelial cell migration and proliferation. Other advantages include lowering ache, making a barrier to bacterial contamination, and preventing protein loss. Available momentary pores and skin substitutes are either organic, such as allografts, xenografts, or amniotic membrane, or synthetic, corresponding to Biobrane. This process also can function a test for wound mattress viability after burn excision, with immune rejection occurring t. When allografts are used as a short lived coverage to the face and palms, they need to be utilized as sheet grafts. This prevents the formation of granulation tissue between the interstices, which might cause scarring and poor cosmetic end result following definitive autografting. Amniotic membrane can be used to provide short-term coverage to superficial burns. Given its flexibility and pliability, amniotic membrane is beneficial for software on irregular surfaces such as the face. Despite not decreasing therapeutic time or scarring, it offers some of the benefits of wound coverage and reduces the variety of dressing changes required until healing is achieved. Ideally, near-total excision ought to be accomplished as soon as attainable in the first few days following injury, positively within per week. The again, buttocks, and posterior thighs are lined with autograft skin taken at thickness between zero. Allografts are the finest option to apply as an overlay to protect broadly meshed autografts. Dermal replacements are an costly possibility but produce good leads to relation to scarring. Integra is a bilaminar composite that has a neodermis of bovine collagen held in a matrix sample of shark cartilage chondroitin-6-sulfate. The stomach, anterior thigh, forearm, leg, and male chest are websites where Integra may be easily utilized. The neo-dermis is vascularized from the underlying wound mattress, and the method takes 2�3 weeks to full. The neo-dermis often develops a pink or plum color as a result of staining of the matrix through the vascularization course of. If hematoma or seroma develops, it can be aspirated with a 27-gauge needle, or the overlying Integra is incised, the hematoma eliminated, and the edges are stapled down. The second-stage operation involves gentle removal of the silicone layer and utility of zero. The first priority stays excision of all of the burn wounds, wound coverage with autografts, and application of allografts to the remaining areas, with a return to the working room planned once used donor websites are healed. Only half of the delayed excision group finally required surgical intervention, and a significantly smaller area of excision was necessary. This strategy needs to be balanced with the knowledge that the longer a wound remains open, the larger the inflammatory response and subsequent scar formation. Biobrane is a nylon/silicone bilaminated composite skin substitute that becomes adherent to the exposed dermis, thereby appearing as a neo-epidermis. Other alternate options embrace using silverimpregnated dressings similar to Acticoat, allografts, and xenografts. The Operating Room the burn operating room is usually an extension of the burn intensive care unit. The procedures are long, intense, and require a number of particular person setups for different types of gear and instrumentation. A very important perioperative concern for secure management of a affected person present process intensive burn excision is the upkeep of physique temperature. The affected person is normally completely uncovered with little intact skin, significantly after procurement of donor pores and skin, resulting in speedy warmth loss. A number of methods can be used to counteract heat loss and preserve normothermia. The working room ought to be warmed to 32�C, since the latent heat of water evaporation is 31. Above this temperature, the energy supply for evaporation will come from the environment rather than the affected person. Other adjunctive measures embody the use of area blankets, aluminum foil coverings, plastic t.
Cheap 2.5mg nitroglycerin with visaA profit much like treatment genital herpes nitroglycerin 6.5mg mastercard every day wake-up protocols but without related morbidity can be attainable with a protocol of day by day assessment of sedation and dosage adjustment. Elimination is very fast by nonspecific esterases in blood and tissue, which give it a context-sensitive half-time of roughly four min with out regard to length of infusion. The abrupt recovery from remifentanil analgesia has been related to hyperalgesia. This may be prevented by concomitant doses of -2 adrenergic agonists, ketamine, or a longer-acting opiate prior to termination of infusion. With a Vd of less than one-fourth that of fentanyl, alfentanil additionally has a quicker clearance and shorter half-life. There are multiple reviews of improved pain control in patients switched from morphine to methadone. Its onset of motion is more fast than morphine after intravenous injection due to its greater lipid solubility. Its elimination is quite variable but considerably longer (t1/2 7�65 hours) than that of morphine (t1/2 1. As a outcome, treatment of burn sufferers with lorazepam must be more predictable than with diazepam and due to this fact extra controllable and efficient. Diazepam has a relatively lengthy half-life and is biotransformed to energetic metabolites. Midazolam is a shorteracting agent appropriate for temporary procedures or infusion and is probably the most incessantly used sedative in U. However its major hydroxylated metabolite, -hydroxymidazolam, is at least as potent as midazolam. Although its analgesic action is too weak to adequately control pain of more than minor burns by itself, acetaminophen acts synergistically with more potent analgesics and is a vital element of multimodal ache protocols. Gabapentin and pregabalin are such drugs which were discovered to be effective for the management of neuropathic pain. Benzodiazepines are essentially the most commonly used anxiolytic agents used in burn centers. Pharmacokinetic concerns affect the choice of benzodiazepines in burn sufferers. Diazepam is metabolized by P450 oxidases (phase I reaction), and its metabolism and clearance have been depressed in burned patients. It has been used extensively alone and in combination with different medication primarily for controlling ache throughout procedures associated to burn care, but in addition low-dose infusions can enhance ache control in some sufferers tolerant to morphine. Ketamine causes pain when administered intramuscularly or through a peripheral intravenous catheter. It additionally causes tachycardia and hypertension, which may be poorly tolerated by older patients with hypertension or coronary artery disease. These side effects could be lowered by concomitant administration of an 2 adrenergic agonist. Ketamine has been avoided in sufferers with increased intracranial stress because it has been reported to cause increased cerebral blood flow which may additional increase intracranial stress. At the identical time, respiratory drive, airway patency, and airway reflexes are preserved. Ketamine has an intensive report of safety in pediatric emergency departments even when given without regard to prandial state. Midazolam is commonly described as a remedy, however dexmedetomidine may be more practical. Ketamine sedation may be associated with elevated salivation that can make laryngospasm extra doubtless but, in contrast to laryngospasm attributable to inhalation agents, laryngospasm with ketamine is largely self-limiting. The analgesic action of dexmedetomidine and clonidine is weak, and these medicine are most effective as adjuvants. They cut back dose requirements for narcotics and counteract opiate-induced hyperalgesia. Compared to clonidine, dexmedetomidine is a extra selective adrenergic agonist and has the next affinity for the two receptor. Among some great benefits of 2 adrenergic agonists are the shortage of impact on airway patency, respiratory drive, and airway reflexes. Dexmedetomidine limits the hypertension and tachycardia associated with ketamine, which could be problematic in older sufferers. In addition, dexmedetomidine additionally potentiates the analgesic effect of ketamine and on this method reduces the dose of ketamine wanted. Propofol has additionally been utilized in sub-anesthetic doses together with an analgesic drug for sedation throughout annoying procedures. Ronan and others found sedation of intubated sufferers to be superior with propofol than with midazolam infusion in phrases of velocity of wake-up and quality of sedation. In doses that end in loss of consciousness (general anesthesia) propofol causes lack of pharyngeal tone, which can trigger airway occlusion. If blood stress is maintained by elevated sympathetic tone, as with decreased circulating blood volume, administration of clonidine or dexmedetomidine may cause hypotension. When administered by mouth or nasogastric tube, clonidine has an roughly 85% bioavailability. Its low efficiency requires 50�70% inhaled concentrations to present important analgesia. Filkin and Marvin have reported effective analgesia throughout burn wound care with self-administered nitrous oxide. This outcomes from oxidation by nitrous oxide of the cobalt in vitamin B12, which impairs its coenzyme perform. Clinical presentation mimics pernicious anemia, with megaloblastic anemia and subacute mixed degeneration of the spinal cord. Hayden and colleagues reported a case of myeloneuropathy in a burn affected person chronically uncovered to excessive concentrations when he was given 50% nitrous oxide in oxygen to self-administer advert lib over roughly 4 months. If nitrous oxide is used for analgesia for burn sufferers, enough consideration must be given to continual publicity of personnel. In the case of second-degree wounds, using woundcovering dressings virtually instantly eliminates ache in the burn wound web site. As an example, Schwarze and colleagues in contrast the scientific efficacy of two synthetic burn wound dressings, Suprathel and Omiderm. The mechanism of this phenomenon has not been established, however Sullivan and colleagues found an affiliation of increased fluid volumes administered with elevated doses and number of narcotics given to burn patients. Adequate ache management requires that each patient be continuously assessed for ache and anxiousness. However the advantages of a multimodal method to pain control are usually accepted, particularly for patients with average and extreme pain. The use of a number of medication with different mechanisms of action offers synergistic results that improve ache control and allows the utilization of decrease doses of opiates. During the acute section of recovery from burn accidents sufferers with good pain management usually experience transient periods of sudden intense improve of their ache. The depth of breakthrough pain is often so nice that an opiate is required. Of all different patients with partial or partial plus full-thickness burns, 18% were additionally painless.
Purchase nitroglycerin online pillsPatients who expertise such itching often excoriate new grafts or just lately healed skin treatment 2 go order nitroglycerin with a visa, thus enhancing their susceptibility to infections. Pat Blakeney and Janet Marvin at the Shriners Hospital for Children in Galveston developed an instrument to measure itch referred to as "itch man". One from Belgium has been translated and validated in English and seeks to measure all of the aspects of itching and the method it relates to different forms of variables. The experience of pain may affect the perceptions of other signs, including nervousness, worry, or itch. There are many measurement tools for pain, nervousness, and itch assessment throughout the life span that could be helpful to the clinician and the researcher. It was initially developed in animals and extra recently used clinically in people. For instance, blisters left intact lead to less pain,106 however this apply is questionable due to attainable infection associated with the blisters. One additional concern regarding procedures is the amount of ache created by eradicating a dressing from the burned space. These removals are often facilitated by soaking the dressings off, however the soaks are typically painful. Some newer dressings are straightforward and painless to remove, and moist, exposed-burn ointment dressings107 are being developed to further cut back pain. Acticoat was found to be a lot less painful than silver sulfadiazine within the remedy of partial-thickness burns by Varas et al. The use of resection and grafting of open burn wounds significantly reduces burn pain. Even short-term protection with cadaver skin or pigskin reduces ache in the area of the burn. Cultured allogeneic keratinocyte sheets accelerated therapeutic and thereby reduced pain and suffering compared to Opsite therapy. Pain evaluation as early as day 3 revealed decrease pain scores in those sites handled with keratinocyte sheets. Less costly dressings embrace honey as a result of it provides the synergistic interactions of a moist surroundings, antibacterial exercise, and antiinflammatory motion and thereby promotes healing. The first tenet is that if the patient says he or she is having pain, she or he is struggling. In addition, preliminary physiological changes related to giant burns make uptake from injection sites erratic and unpredictable. Last, dose and type of medication should be reevaluated frequently through the hospital course to make certain pain is t. Dramatic physiological modifications associated with large burns produce important pharmacokinetic and pharmacodynamic alterations that have an effect on drug selection and dosing issues. An preliminary burn shock (ebb) phase with decreased circulating blood volume, decreased cardiac output, and elevated systemic vascular resistance is followed after approximately forty eight hours by a hyperdynamic/hypermetabolic (flow) part with elevated cardiac output and decreased systemic resistance, elevated oxygen consumption, and intense catabolism. These adjustments in cardiac output and organ perfusion also affect hepatic and renal drug clearance in a biphasic fashion. For instance, in the course of the ebb part, hepatic and renal blood circulate could additionally be decreased enough to impair drug metabolism and excretion. Conversely, in the course of the flow section, increased hepatic blood move enhances clearance of medication corresponding to fentanyl and propofol that are effectively extracted by the liver. Furthermore lack of plasma proteins by way of open wounds and extensive edema because of large fluid resuscitation profoundly alter drug distribution and binding to plasma proteins. Sympathetic tone and drug publicity through the hospital course alter the up- and downregulation of varied drug receptors. Devastating burn accidents produce intense anxiousness that could be exaggerated or lowered by the effectiveness of ache management. All these elements ultimately affect responses to analgesic (and other) drugs in ways which are usually unpredictable. Patient response should be carefully monitored and drug choice and dosing adjusted rigorously to avoid undertreatment or problems of overdose. Drug selection and dosing are very different for each of those scientific situations. This allows number of an agent with speed of onset and length of action acceptable to particular clinical wants. A number of routes of administration are additionally possible with this large group of medicine. This drawback occurs frequently when physicians are reluctant to prescribe the recommended dose for ache. Higher doses needed for intense ache associated with procedures may trigger unsafe despair of respiration. Use of adjuvant drugs and a multimodal method Morphine Morphine has been described because the gold normal for treating burn ache and remains the first alternative in many burn items. Time to peak effect and length of action for morphine are applicable for treating background and breakthrough ache most of the time. The energetic morphine-6-glucuronide metabolite of morphine is excreted in urine and may accumulate in patients with renal failure. A change to methadone has been reported efficient in patients poorly controlled by morphine. Additional brokers included in multimodal strategies to scale back narcotic analgesics are benzodiazepines, acetaminophen, gabapentin, and pregabalin. Fentanyl Fentanyl is a potent artificial opiate with a comparatively rapid onset of motion and a shorter length of impact than morphine. An oral transmucosal dosage kind can be out there and has been discovered efficient in pediatric patients throughout procedures. Discontinuing sedation in ventilated patients can be related to significant morbidity, corresponding to unplanned extubations. These observations recommend that the majority patients with full-thickness burns have significant ache. Not solely is the injection painful, but, in the course of the early levels of major burns, absorption from tissue websites is highly variable and unpredictable. With decreased intravascular quantity and cardiac output, tissue perfusion could also be low and absorption poor. Later, with fluid resuscitation, drug might enter the circulation as tissue perfusion is restored. In a survey of using antianxiety medicine in burned youngsters, 72% obtained lorazepam at a dose of zero. Occasionally the standard of ache control will deteriorate to the point that changes in drug dose or selection must be modified to keep adequate analgesia. A number of mechanisms can account for problem or deterioration of ache control by standard protocol (Table sixty four. Also, intubated patients requiring mechanical air flow present a further challenge for managing ache control. Burn patients poorly managed with rising doses of morphine have benefited from substitution of methadone.
References - Theron JG, Payelle GG, Coskun O, et al: Carotid artery stenosis: treatment with protected balloon angioplasty and stent placement, Radiology 201:627-636, 1996.
- Chew D, Aroney C, Aylward P, et al. Addendum to the National Heart Foundation of Australia/Cardiac Society of Australia and New Zealand guidelines for the management of acute coronary syndromes (ACS) 2006.
- Swan C, Tostevin AL, Black GHB. Final observations on congenital defects in infants following infectious disease during pregnancy with special reference to rubella. Med J Aust. 1946;2:889-908.
- Sturzenegger MH, Meienberg O. Basilar artery migraine: a follow-up study of 82 cases. Headache 1985;25:408.
|


