|
Dr James Down - Consultant in Intensive care and Anaesthesia
- University College Hospital
- London
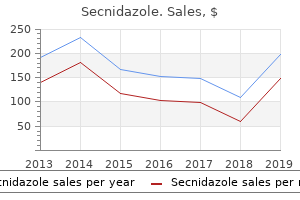
Secnidazole dosages: 500 mg
Secnidazole packs: 1 pills, 12 pills, 24 pills, 36 pills, 60 pills, 120 pills

Order secnidazole 1 gr without prescriptionClinical Features the scientific features of a secondary orbital tumor necessarily vary with the sort and placement of the first neoplasm symptoms 6 days post iui order 500mg secnidazole with amex. This is especially true of eyelid, conjunctival, lacrimal sac, and intraocular tumors. In cases of sinus or nasopharyngeal tumors and sphenoid wing meningioma, the orbital manifestations are commonly the initial options of the disease. Diagnostic Approaches In instances of suspected secondary orbital tumor, it is very important take a detailed medical history and to carry out an ocular and systemic analysis. External ocular examination, slitlamp biomicroscopy, and fundus examination can reveal the first tumor. Chapter forty Orbital Secondary Tumors 769 Pathology the histopathology of a secondary orbital tumor necessarily varies with the sort of neoplasm. The pathology of those tumors is covered in textbooks and elsewhere in the current atlases. Management the management of orbital extension of the assorted periorbital tumors can differ greatly from case to case; each case should be individualized. In general, broad surgical resection often adopted by irradiation or chemotherapy are treatment options. Massive orbital extension by primary eyelid and conjunctival tumors (basal cell carcinoma, squamous cell carcinoma, melanoma, and so on. Massive orbital extension of uveal melanoma (18) or retinoblastoma can also require orbital exenteration, however there are various alternate options for gentle levels of orbital involvement, together with techniques of irradiation and chemotherapy. Mild degrees of secondary orbital invasion by lymphoma, metastatic carcinoma, rhabdomyosarcoma, and esthesioneuroblastoma can often be managed by irradiation. Orbital extension of sphenoid wing meningiomas may be managed by surgical excision, irradiation, or both, depending on the clinical scenario. There are many different conditions where treatment depends on the entire clinical state of affairs. Sebaceous gland carcinoma of the ocular adnexa: A clinicopathologic study of 104 cases with five year followup data. Conjunctival melanoma: Risk elements for recurrence, exenteration, metastasis and dying in one hundred fifty consecutive patients. Oncocytic adenocarcinoma of the lacrimal sac: report of a case with paranasal sinus and orbital extension. Neglected basal cell carcinoma close to lateral canthus with secondary orbital invasion in a 63-year-old man. The motility of the eye was markedly restricted owing to diffuse orbital involvement. Neglected basal cell carcinoma of lower eyelid and lateral canthus with secondary orbital invasion causing upward displacement of the proper eye in a 69-year-old man. The fibrosis within the tumor was producing a secondary ectropion of the lower eyelid. Orbital invasion by basal cell carcinoma of the lower eyelid in a 66-year-old man. Note the huge tumor replacing the medial side of the orbit and ethmoid sinus with extension into the cranial cavity. Mass in superotemporal orbit with thickening of higher eyelid in a 65-year-old lady. A small lacrimal gland biopsy accomplished elsewhere revealed a malignancy and orbital exenteration was accomplished. Low-magnification photomicrograph displaying basophilic mass superior to the globe within the lacrimal gland. Photomicrograph exhibiting Pagetoid invasion of sebaceous gland carcinoma within the dermis. Although there was a suggestion of major lacrimal gland neoplasm, the thickened eyelids instructed sebaceous carcinoma. The lesion was eliminated surgically and residual eyelid/conjunctival tumor was treated with plaque brachytherapy. Chapter 40 Orbital Secondary Tumors 773 Orbital Invasion From Eyelid Melanoma Cutaneous melanoma has a tendency in some cases to invade the dermis by neurotropic mechanisms and to recur as a deep nodule. An eyelid melanoma can invade the delicate tissues of the orbit by an analogous mechanism. This is particularly true of desmoplastic melanoma, which can exhibit deeper invasion along nerves, a course of referred to as "neurotropism. The affected person underwent orbital exenteration however later developed overt systemic metastasis. Blepharoptosis and proptosis of left eye in a 79-year-old lady who had excision of a cutaneous melanoma from left medial canthal area 5 years earlier. Axial computed tomography displaying circumscribed tumor within the posterior side of the orbit. Histopathology of reexamined cutaneous lesions displaying spindle cells invading a nerve. Photomicrograph of another area of orbital tumor exhibiting anaplastic spindle and epithelioid cells. Immunohistochemistry of each the original eyelid lesion and the orbital recurrence confirmed the diagnosis of melanoma. In such situations, eyelid-sparing orbital exenteration is commonly required to obtain tumor management. Orbital computed tomography confirmed extension into the orbit with compression of the equator of the globe. Proptosis, eyelid ecchymosis, and conjunctival hemorrhagic chemosis in a 56-year-old man who was immunosuppressed after liver transplantation. Surgery was carried out elsewhere for conjunctival squamous cell carcinoma and this represented recurrence. Sectioned orbital exenteration specimen demonstrating a big hemorrhagic mass temporal to the globe. Chapter forty Orbital Secondary Tumors 775 Orbital Invasion From Conjunctival Melanoma In rare instances, conjunctival melanoma is much superior on the time of the preliminary analysis and first orbital exenteration is necessary. Much extra generally, nevertheless, orbital invasion of conjunctival melanoma happens after numerous prior resections of very aggressive conjunctival melanoma, notably the kind that arises from major acquired melanosis. Recurrent conjunctival melanoma in superonasal fornix with anterior orbital invasion in a 64-year-old man. Coronal magnetic resonance imaging in T2-weighted picture showing inferior orbital melanoma in a 50-year-old lady who had prior excisions of conjunctival melanoma. Recurrent conjunctival melanoma with orbital invasion surrounding the left globe in a 72-year-old girl.
Purchase secnidazole with paypalFurthermore medicine 832 order secnidazole paypal, evidence from quasielastic light-scattering spectroscopy reveals that nucleation of solid cholesterol crystals might occur directly from supersaturated micelles in conjugated deoxycholate-rich bile in vitro with out an intervening vesicle or liquid crystalline phase. With typical physiologic phospholipid contents (region C), early liquid crystals (d = 1. With still larger phospholipid contents (region D), liquid crystals are followed by cholesterol monohydrate crystals only. At the best phospholipid mole fractions (region E), liquid crystals are fairly secure and no solid crystals form. Nonprotein factors that retard ldl cholesterol nucleation and crystallization include (1) a total lipid concentration less than three g/dL, (2) reduced hydrophobicity of the bile salt pool, (3) low bile saltto-phospholipid ratios, (4) low cholesterol-to-phospholipid ratios in vesicles, and (5) low total calcium ion concentrations. The states reverse to these circumstances speed up ldl cholesterol nucleation and crystallization. These findings suggest that lithogenic bile could comprise pronucleating brokers that speed up crystallization or that normal bile might comprise antinucleating brokers that inhibit crystallization. Furthermore, bile may comprise both accelerators and inhibitors of crystallization, and imbalances between them can induce speedy ldl cholesterol crystallization in gallbladder bile in sufferers with cholesterol gallstones. Mucin or mucin glycoproteins are large molecules that encompass a protein core and a lot of carbohydrate aspect chains. Gallbladder mucins, a heterogeneous household of O-linked glycoproteins, are divided into 2 lessons: epithelial and gel-forming mucins. Mucins from totally different organs vary in carbohydrate facet chain, protein composition, and cost however usually have related properties. They have an overall cost and are able to binding different charged species corresponding to calcium. Hydrophobic domains in the mucin molecule (on the nonglycosylated areas of the polypeptide core) allow binding of lipids such as cholesterol, phospholipids, and bilirubin. Gallbladder mucins play an important function in the early phases of gallstone formation and are a potent pronucleating agent for accelerating ldl cholesterol crystallization in native and mannequin biles. Indeed, hypersecretion of gallbladder mucins is a prerequisite for gallstone formation, and increased quantities of gallbladder mucins are consistently observed in gallbladder bile of several animal models of gallstones. Mucins are additionally a major part of sludge within the gallbladder, and sludge has been shown to be a precursor of gallstones. Therefore, 2 roles in the formation of gallstones have been proposed for mucins: (1) a pronucleating agent for accelerating the nucleation and crystallization of ldl cholesterol from saturated bile and (2) a scaffolding for the deposition of stable ldl cholesterol monohydrate crystals during the development of stones. The synthesis of mucin glycoproteins which may be secreted by the mucin-producing cells of the gallbladder and bile ducts could also be regulated by mucosal prostaglandins derived from arachidonic acid�containing biliary phospholipids. Then, the carbohydrate groups of the polymers of mucins avidly bind water to type gels. The hydrophobic polypeptides within the core of mucin glycoproteins also can bind bilirubin and calcium in bile. The resulting water-insoluble complicated of mucin glycoproteins and calcium bilirubinate provides a floor for nucleation of ldl cholesterol monohydrate crystals and a matrix for the expansion of stones. Mucin secretion and accumulation in the gallbladder is decided by multiple mucin genes. As a result, ldl cholesterol crystallization and the event of gallstone formation are significantly retarded. These findings counsel that gene-gene interactions between the Muc1 and Muc5ac genes may affect mucin secretion and accumulation within the gallbladder. Many glycoproteins that bind reversibly to concanavalin A� Sepharose also velocity up ldl cholesterol crystallization. Calcium certain to micelles and vesicles in bile might accelerate ldl cholesterol crystallization by selling fusion of cholesterol-rich vesicles. The rapidity of cholesterol crystal formation also varies in proportion to the deoxycholate content material of bile and is expounded to the impact of deoxycholate on the equilibrium part relationships of biliary lipids. The diploma of cholesterol supersaturation of bile may be a determinant of fast crystallization of cholesterol. The protein could inhibit growth of strong cholesterol crystals by attaching to the most quickly rising microdomains on a crystal face and interfering with additional solute attachment. It remains to be uncertain whether only 1 or a number of antinucleating factors exist and how they may inhibit the initiation of ldl cholesterol crystal formation, however unilamellar vesicles have been proposed to be the necessary thing sites of action. In abstract, though many biliary proteins apart from mucin gel have been proposed as both pronucleating or antinucleating factors influencing ldl cholesterol nucleation and crystallization in bile, their in vivo roles (if any) in the pathogenesis of cholesterol gallstone formation stay unclear. Gallbladder Dysfunction Under normal physiologic circumstances, frequent gallbladder contractions occur throughout the day. Between meals, the gallbladder stores hepatic bile (with a mean fasting quantity of 25 to 30 mL in healthy subjects). Following a meal, depending on the degree of neurohormonal response, the gallbladder discharges a variable amount of bile. Furthermore, the poor interdigestive gallbladder filling is in maintaining with delivery of a greater percentage of lithogenic bile from the liver immediately into the small intestine, leading to augmentation of the enterohepatic effects of elevated recycling and bile salt hydrophobicity. These observations present that emptying and filling of the gallbladder are affected in sufferers with gallbladder hypomotility. These findings indicate that extra ldl cholesterol molecules within the gallbladder wall may act as myotoxic agents. In particular, signal transduction in response to binding of agonists is impaired. Defects in contractility related to ldl cholesterol gallstones are reversible at an early stage and are mainly as a end result of accumulation of extra biliary cholesterol in the membranes of gallbladder clean muscle cells. This mechanism seems to clarify why gallbladder emptying is impaired earlier than gallstones are fashioned in animal fashions at a time when bile is supersaturated with cholesterol. In addition, the intracellular mechanisms of easy muscle contraction appear to be intact in human gallbladder muscle cells from sufferers with cholesterol gallstones. These findings support the speculation that increased absorption of ldl cholesterol from the gallbladder lumen is associated with gallbladder smooth muscle dysfunction. This alteration could induce stiffening of sarcoplasmic membranes secondary to an increase in ldl cholesterol content material of the membranes. Gallbladder stasis induced by the hypofunctioning gallbladder might present the time necessary to accommodate nucleation of ldl cholesterol crystals and progress of gallstones within the mucin gel within the gallbladder. In explicit, sludge incorporates calcium, pigment, bile salts, and glycoproteins and will function a nidus for nucleation and crystallization of ldl cholesterol or precipitation of calcium bilirubinate. As a end result, bile stagnates and sludge develops within the gallbladder, thereby enhancing gallstone formation. Differential absorption charges of ldl cholesterol, phospholipids, and bile salts by the gallbladder epithelial cells could reduce cholesterol saturation of bile in normal topics; however, the gallbladder epithelium of sufferers with cholesterol gallstones loses the capacity for selective absorption of biliary cholesterol and phospholipids. In all likelihood, cholesterol molecules are absorbed constantly by the gallbladder mucosa from supersaturated bile,146 and the unesterified cholesterol molecules diffuse rapidly to the muscularis propria as a end result of the gallbladder lacks an intervening muscularis mucosae and submucosa. As in an atherosclerotic plaque, mucosal and muscle membranes apparently turn into saturated with cholesterol and coexist with stored cholesteryl ester droplets.
Buy secnidazole 500mg mastercardEur J Gastroenterol Hepatol 1996; eight:685-91; Feldstein A medications definition order cheap secnidazole on line, Perrault J, El-Youssif M, et al. Episodes of pruritus, jaundice, stomach ache, and fever are usually interspersed with asymptomatic durations of various length. These episodes of obstruction could predispose to cholestasis and induce an acute inflammatory reaction. When the serum bilirubin degree is elevated, the bilirubin is predominantly conjugated. Reductions within the serum albumin degree and prolongation of the prothrombin time could mirror hepatic synthetic dysfunction with advanced liver disease. Vitamin K malabsorption related to cholestasis may play a role in prolonging the prothrombin time. Other nonspecific consequences of cholestasis are elevations in serum copper, serum ceruloplasmin, and hepatic copper ranges, elevated urinary copper excretion, and elevated serum levels of cholesterol. Hyperglobulinemia is frequent; serum IgM levels are elevated in as much as 50% of patients, and IgG and IgA levels can also be elevated. When bodily abnormalities are present, the most typical are hepatomegaly, jaundice, and splenomegaly (see Table 68. Skin findings are frequent and include cutaneous hyperpigmentation, excoriations resulting from pruritus, and xanthomata. As liver illness progresses, spider telangiectasias, muscle atrophy, peripheral edema, ascites, and other indicators of superior liver illness may seem (see Chapter 74). The characteristic cholangiographic findings embody multifocal stricturing and ectasia of the biliary tract. Areas of narrowing are interspersed with areas of regular or near-normal caliber and areas of poststenotic dilatation. Localized segments of dilated ducts might have a saccular or diverticular appearance. Major areas of focal, tight narrowing often recognized as dominant strictures, may be seen and infrequently involve the bifurcation of the hepatic duct. The fibrosis is accompanied by a blended inflammatory infiltrate that will involve the epithelium and biliary glands. The attribute bile duct lesion is a fibro-obliterative course of that will lead to an "onion-skin" look of concentric fibrosis surrounding medium-sized bile ducts. Other characteristic histopathologic findings might embrace bile duct proliferation, periductal inflammation, and ductopenia. The degree of irritation can be fairly variable but is typically a portal-based mixture of lymphocytes, plasma cells, and neutrophils with a periductal focus. In one examine, histologic examination could classify solely 28% of patients who had 1 of the 2 ailments. In stage 1 (portal stage) modifications are confined to the portal tracts and encompass portal inflammation, connective tissue expansion, and cholangitis. Stage 2 (periportal stage) is characterized by growth of inflammatory and fibrotic processes past the confines of the limiting plate, leading to interface hepatitis ("piecemeal necrosis") and periportal fibrosis. Depending on the diploma of biliary obstruction, ductular proliferation and cholangitis may be of various severity. The intrahepatic ducts are mainly affected and present diminished arborization (pruning), with diffuse segmental strictures alternating with normal-caliber or mildly dilated duct segments (cholangiectasis), resulting in a beaded appearance. B, Imaging options embrace diffuse irregularity of the intrahepatic ducts, multiple brief strictures and cholangiectasis, small diverticula within the wall of the frequent hepatic duct (arrow), and clips from a prior cholecystectomy. Both the extrahepatic and intrahepatic bile ducts are abnormal in roughly 75% of circumstances. A, A segmental bile duct is obliterated by fibrosis (arrow), demonstrating "fibro-obliterative cholangitis" (H&E, �200). B, A medium-sized bile duct is surrounded by concentric fibrosis with an onionskin appearance (H&E, �400). The development of histologic stage over time has been examined in a single observational study and several clinical trials by which liver biopsy findings had been included as an end point. Using a Markov model, they estimated the charges of development for patients with stage 2 disease to be 42%, 66%, and 93% at 1, 2, and 5 years, respectively. Unlike observational studies, scientific trials present prospectively collected biopsies at defined intervals with much less likelihood of remedy bias. Biopsy specimens had been additionally staged for fibrosis by the Ishak system, and of 216 subjects with evaluable liver biopsy specimens, seventy four (34%) had no change, 80 (37%) progressed a minimal of one stage, and 62 (29%) regressed at least one stage. In addition, 30 of the 191 (16%) without cirrhosis at entry progressed to cirrhosis over 2 years. The characteristic cholangiographic findings are multifocal stricturing and ectasia of the biliary tract. Areas of narrowing are interspersed with areas of regular or near-normal caliber and of poststenotic dilatation. Isolated extrahepatic bile duct involvement is rare, whereas isolated changes of the intrahepatic bile ducts have been reported in 20% to 28% of circumstances. The degree of inflammatory activity might subside as the stage of the disease progresses, and focal bile ductular proliferation could additionally be putting. The actual Nakanuma stage is the sum of the scores for the final 3 options: stage 1 is a rating of zero, stage 2 is 1 to three, stage three is four to 6, and stage four is 7 to 9. The intrahepatic biliary radicles are diffusely irregular and characterized by pruning and a beaded look. Note the highgrade, dominant, distal bile duct stenosis (arrows) with a markedly enlarged gallbladder, suggesting that the stricture includes the insertion of the cystic duct. Although liver histologic findings within the 2 problems might overlap (see earlier),134 the excellence between the 2 is readily obvious on cholangiography. Overall, signs developed in 24 (53%), and progressive liver illness, demonstrated by new symptoms or signs, worsening cholangiographic findings, or progressive liver histologic abnormalities, developed in 34 (76%) sufferers. Differences in the charges of development between these research could also be the outcome of differences in patient populations, presumably because of referral bias, the definition of "asymptomatic," and the duration of clinical follow-up. Similar findings have been reported in a large Swedish study; sufferers who had been symptomatic at the time of entry into the examine had a considerably worse-than-expected survival (9. The illness could additionally be considered to progress through the following four scientific phases, although some phases may not develop or be obvious in an individual patient: 1. Asymptomatic phase: Patients remain asymptomatic but have biochemical abnormalities, typically elevation of serum alkaline phosphatase levels with variable elevations of serum bilirubin and aminotransferase ranges. Pruritus, fatigue, signs of cholangitis, and jaundice may occur, usually together. Decompensated cirrhosis: the final part is characterised by worsening signs and problems of end-stage liver illness, corresponding to ascites, encephalopathy, and variceal bleeding. In settlement with this research, a large population-based research from the Netherlands that included 590 patients estimated median transplant-free survival time to be 21. Several studies indicate that sufferers in whom the serum alkaline phosphatase level stays persistently normal or at least lower than 1. Interestingly, eight kids developed cholangiocarcinoma at a median of 6 years after their diagnosis. With this mannequin, three risk teams (low, intermediate, high) had been recognized, and predicted survival curves were shown to be much like observed survival curves.
Order secnidazole with visaHowever symptoms bipolar disorder 500 mg secnidazole for sale, such injections should be carried out with great care, as a result of inadvertent corneal penetration and traumatic cataract have been not often recognized as complications of corticosteroid injection (16). Chapter 12 Eyelid Inflammatory Lesions Simulating Neoplasms 209 Selected References 1. Warming lignocaine reduces the pain of injection during native anaesthetic eyelid surgery. Eyelid tumors in youngsters: a clinicopathologic examine of a 10year evaluate in southern Taiwan. Photomicrograph of chalazion showing lipid globule surrounded by acute and persistent inflammatory cells. Photomicrograph of chalazion showing big cell in area of granulomatous irritation. It can erode by way of the skin or tarsal plate, producing an erosive or ulcerated look. A ruptured chalazion can assume a diffuse configuration and not utilizing a distinct nodule. In some cases, it can trigger diffuse thickening of the eyelid, simulating a blepharoconjunctivitis or sebaceous carcinoma. Chalazion of proper decrease eyelid in a baby exhibiting typical erosion of overlying pores and skin. Same child 1 month later after therapy with antibiotic ointment and compresses, exhibiting decision of the lesion. Elderly patient with persistent chalazion of upper and decrease eyelids and a few loss of cilia. In this case, sebaceous carcinoma was entertained, however the prognosis of chalazion was confirmed histopathologically. Sarcoidosis is an idiopathic illness characterised by noncaseating granulomatous inflammation. It can appear in the eyelid as an initial manifestation or in a affected person with identified systemic or ocular sarcoidosis (1�6). Clinical Features In the eyelid, sarcoidosis typically appears as a quantity of irregular, agency subcutaneous nodules (3,4). The adjacent conjunctiva show quite a few nodules or diffuse thickening, simulating a lymphoid infiltrate or viral conjunctivitis. On event, sarcoidosis has been reported to produce a extra aggressive "damaging" lesion within the eyelid (5,6). Management A biopsy is mostly required to make the diagnosis of eyelid sarcoidosis. It is also well known that a biopsy of suspicious areas of the adjacent conjunctiva can set up the analysis (7,8). Gallium scan could show lacrimal gland that will help the analysis of the eyelid lesions. Sarcoidosis of the eyelid, like sarcoidosis elsewhere, is generally responsive to oral or intralesional corticosteroids. The damaging eyelid variant could also be harder to manage, however can show some response to corticosteroids and different immunosuppressive agents. There has been a suggestion that such lesions may also respond to thalidomide (6). Conjunctival biopsy as an assist within the analysis of the patient with suspected sarcoidosis. Chapter 12 Eyelid Inflammatory Lesions Simulating Neoplasms 213 Eyelid Pseudorheumatoid Nodule (Granuloma Annulare) General Considerations Pseudorheumatoid nodule (granuloma annular) is an idiopathic, benign, self-limited, granulomatous illness that affects the top area of children and younger adults (1�7). It is so named due to its histopathologic similarity to the subcutaneous nodule of rheumatoid arthritis or rheumatic fever. The eyelid and adjoining ocular buildings can be involved, with a predilection for the higher eyelid and lateral canthus. Clinical Features Pseudorheumatoid nodule can seem as one or more agency, movable, subcutaneous, tan-colored papules that may develop in a ring sample. It has a predilection for the lateral facet of the higher eyelid and lateral canthus. The lesion pursues a benign course and will slowly regress without remedy in some instances. Pathology As talked about, the lesions resemble the subcutaneous nodules seen with rheumatoid arthritis. There is generally a central area of necrobiotic collagen surrounded by a palisade of histiocytes and epithelioid cells. It can affect the nasal cavity and orbit and secondarily contain the eyelids (1�15). Eyelid involvement happens secondary to vasculitis and may manifest as erythema, edema, irregular thickening, or ulceration of the eyelid (10). There is often severe irritation of the tarsal conjunctiva that leads to secondary scarring of the eyelids (7,14). Severe xanthelasma with a yellow colour to the eyelids has additionally been described (8). Although a number of diagnostic laboratory checks have been used, the antineutrophil cytoplasmic antibody is each sensitive and specific and is optimistic in 60% to 90% of sufferers with this illness (1). Lymphocytes, plasma cells, neutrophils, and occasional eosinophils are also present (1). Orbital exenteration has sometimes been needed for extreme destructive lesions (15). Eyelid and conjunctival manifestations because the presenting function in two individuals. Histopathology of sarcoidosis, exhibiting granulomatous inflammation with a large cell. Pseudorheumatoid nodules (granuloma annulare) of higher eyelid in a 5-year-old girl. They usually originate in the lung and may secondarily contain the pores and skin and eyelids by hematogenous dissemination. Examples of mycotic infections inflicting pseudoepitheliomatous hyperplasia are also depicted in Chapter 1. The North American form is endemic in components of the Eastern and Southern United States, especially Kentucky (2). It can have an result on any area of the skin including the face, eyelids, and conjunctiva (1�5). Management Treatment is with antifungal medicine like amphotericin B in standard doses. Clinical Features Eyelid involvement is characterised by a hyperkeratotic plaque which could be crusted and ulcerated. Eyelid Mucormycosis General Considerations Mucormycosis (phycomycosis) generally happens in sufferers with underlying systemic disease similar to diabetic ketoacidosis, advanced malignancy, and other immunosuppressed states. It usually involves the respiratory tract and might secondarily have an result on the orbit with extension to the eyelids (1,2). Clinical Features Mucormycosis can produce necrosis of the orbital tissues and eyelids, leading to a black eschar.
Order secnidazole with american expressAsymptomatic cholelithiasis in children with sickle cell disease: early or delayed cholecystectomy Incidence of persistent symptoms after laparoscopic cholecystectomy: a potential study medications not to take with grapefruit secnidazole 1 gr discount. Relationship between persistence of stomach signs and successful outcome after cholecystectomy. Retained gallbladder/cystic duct remnant calculi as a cause of postcholecystectomy pain. Diagnosing and treating sphincter of Oddi dysfunction: a crucial literature evaluate and reevaluation. Systematic evaluation: sphincter of Oddi dysfunction-non-invasive diagnostic methods and long-term end result after endoscopic sphincterotomy. Transduodenal sphincteroplasty in the administration of sphincter of Oddi dysfunction and pancreas divisum within the trendy era. Cholecystectomy protects towards extrahepatic bile duct cancer: is that this a results of the removal of gallstones Association between screen-detected gallstone illness and most cancers in a cohort examine. Association between cholecystectomy and intestinal cancer: a nationwide report linkage examine. High incidence of cholelithiasis in older patients with homozygous beta-thalassemia. Increased morbidity in surgical patients undergoing secondary (incidental) cholecystectomy. Nationwide evaluation of tendencies in choledocholithiasis management in the United States from 1998 to 2013. The security and efficacy of laparoscopic widespread bile duct exploration combined with cholecystectomy for the management of cholecysto-choledocholithiasis: an up-to-date meta-analysis. Transcystic frequent bile duct exploration within the administration of patients with choledocholithiasis. Long-term end result of biliary reconstruction for bile duct injuries from laparoscopic cholecystectomies. Three sometimes asymptomatic conditions of the gallbladder-cholesterolosis, adenomyomatosis, and gallbladder polyps-are additionally reviewed. The localization of ache to the right hypochondrium or radiation to the proper shoulder is essentially the most specific discovering for a biliary tract origin. Between assaults, the bodily findings are usually normal, with the attainable exception of residual higher abdominal tenderness. In comparability, the management of acalculous biliary ache represents a significant problem. In patients with acalculous biliary ache, symptomatic improvement following cholecystectomy is variable. In one sequence of greater than a hundred patients, 83% had been female, and the imply age was roughly 30 years. Stimulated duodenal bile from sufferers with acalculous biliary ache is extra dilute with respect to each bile acids and phospholipids than bile from patients with gallstones or from management ladies with out biliary signs. The decrease molar share of phospholipids supports the hypothesis that biliary phospholipids are hydrolyzed to free fatty acids, which incite inflammation. Although gallstones and their issues account for most cholecystectomies,1 a constant 15% of these operations are carried out in patients without gallstones. Acute acalculous cholecystitis is often a illness of immobilized and critically ill older males with coexisting vascular illness. The hanging preponderance of younger, fertile ladies amongst sufferers with acalculous biliary ache carefully parallels the epidemiology of cholelithiasis, suggesting that the two circumstances have comparable threat components. Several studies have proven that a subset of sufferers with acalculous biliary ache have histologic evidence of cholesterolosis of their resected gallbladders (see later). In other sufferers, the resected gallbladder demonstrates significant irritation, attribute of chronic acalculous cholecystitis. The robust hyperlink between acalculous biliary pain and different functional bowel issues suggests that visceral hypersensitivity may be a standard cause of biliary ache in sufferers with a normal gallbladder. If cholecystectomy is performed in these sufferers, histologic proof of chronic cholecystitis is found in approximately 90%, cystic duct narrowing in 80%, and cholesterolosis in 30%. The 10 patients in the group randomized to no surgery continued to experience signs. Some are found to have a nonbiliary cause of the signs, and in others the ache resolves with time. As a basic rule, typical biliary ache tends to resolve extra reliably following cholecystectomy than do atypical signs corresponding to bloating or dyspepsia. This statement raises the query as to whether or not surgical procedure should be recommended primarily based on signs, with out scintigraphy, and suggests a period of remark or medical administration earlier than a decision to operate is made, to allow the possibility that the symptoms will resolve. An apparent consequence of the diagnostic uncertainty related to acalculous biliary pain is a dramatic improve within the price of cholecystectomy for acalculous biliary ache, particularly in young and insured individuals and for the reason that introduction of laparoscopic surgery. The rate of cholecystectomy for gallstone disease has declined in the identical inhabitants. The gallbladder epithelium, though normally a strong tissue, is uncovered continuously to some of the noxious agents within the body: a concentrated answer of bile acid detergents. In the course of a traditional day, the gallbladder empties the concentrated bile a number of instances and is replenished with dilute (and presumably much less noxious) hepatic bile. In animal models, tissue destruction can be attenuated by inhibiting prostaglandin synthesis with indomethacin. Expression of tight junction proteins in the gallbladder epithelium of sufferers with acute acalculous cholecystitis differs from that in patients with calculous cholecystitis, maybe reflecting the position of increased gallbladder wall permeability within the systemic inflammatory response. One postulated rationalization for the rising incidence of acute acalculous cholecystitis, particularly in younger sufferers, is obesity and the accompanying enhance in gallbladder wall fats, which has been demonstrated to interfere with gallbladder emptying in animal fashions. In one research, sixteen patients with acute acalculous cholecystitis had significantly extra gallbladder wall fat than regular subjects without cholecystitis. The time period acalculous cholecystitis has been questioned as incorrectly suggesting that the illness is simply cholecystitis with out stones. Instead, the term necrotizing cholecystitis has been proposed to mirror the distinct etiology, pathology, and prognosis of the illness. In reality, of the cholecystectomies performed in postoperative or hospitalized patients recovering from trauma or burns, greater than half are for acalculous illness. Unexplained fever, hypotension, leukocytosis, or hyperamylasemia will be the only clue that one thing is amiss. Compared with the scientific course of typical calculous cholecystitis, that of acute acalculous cholecystitis is more fulminant. By the time the analysis has been made, at least half of the patients have experienced a complication of cholecystitis, similar to gangrene or a confined perforation of the gallbladder. Because the illness typically occurs in debilitated patients and complications happen rapidly, the mortality price of acute acalculous cholecystitis is excessive, starting from 10% to 50%, as in contrast with a 1% mortality price in patients with calculous cholecystitis. Unfortunately, the shortage of particular medical findings that time to the gallbladder, mixed with a complicated medical image associated to antecedent surgery or trauma, makes early prognosis troublesome.
Black Elderberry (Elderberry). Secnidazole. - Cancer, constipation, nerve pain, chronic fatigue syndrome (CFS), hayfever, HIV/AIDS, and other conditions.
- How does Elderberry work?
- "The flu," also called influenza.
- Are there any interactions with medications?
- What other names is Elderberry known by?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96444
Cheapest secnidazoleIn contrast treatment lyme disease cheap secnidazole 1gr without prescription, a strong neoplasm typically appears in adults as a progressive, firm, subcutaneous mass, normally, but not always superior to the medial canthus. Secondary epiphora, typically tinged with blood, is a standard presenting function (2). Diagnostic Approaches Most tumors of the eyelid and conjunctiva may be appreciated clinically by direct visualization. However, these within the Chapter 14 Tumors of the Lacrimal Drainage System 233 Selected References 1. Clinicopathologic findings from lacrimal sac biopsy specimens obtained during dacryocystorhinostomy. Unlike the benign, noninvasive papilloma of the eyelid skin described previously, papilloma of the lacrimal sac is usually of the inverted sort, also referred to as transitional cell carcinoma or schneiderian papilloma, and is extra invasive. It can arise primarily from the lacrimal sac or can prolong into the sac from the nostril or maxillary sinus. Invasive transitional cell carcinoma of the lacrimal sac arising in an inverted papilloma. Clinical Features Both inverted papilloma and squamous cell carcinoma are slowly invasive and frequently recur after excision. Local intracranial extension can develop in more aggressive tumors, similar to mucoepidermoid carcinoma (13). Transformation of inverted papilloma into squamous cell carcinoma happens in 10% to 15% of instances, at which era the tumor becomes extra regionally invasive and might often exhibit orbital recurrence, mind invasion, and distant metastasis (2). Pathology the histopathology of squamous papilloma and squamous cell carcinoma had been mentioned within the section on squamous neoplasms of the conjunctiva. Squamous cell carcinoma can even arise within the lacrimal sac de novo, without a prior papilloma. The mucoepidermoid variant of squamous cell carcinoma has also been discovered to arise primarily within the lacrimal sac (7,8,13). Management Management of lacrimal sac neoplasms was mentioned within the previous part. Inverted papilloma of the lacrimal sac, the paranasal sinuses and the cervical region. Squamous cell papilloma of the right lacrimal sac appearing as a subcutaneous mass inferior to the medial canthus in a 68-yearold African-American patient. Squamous cell carcinoma of proper lacrimal sac presenting as an erosive mass in right medial canthal area of an elderly man who had in depth publicity to daylight. Histopathology of inverted squamous papilloma or early invasive squamous cell carcinoma of lacrimal sac, displaying papillomatous lobules of tumor cells with intracellular mucin. Although its origin is disputed, it probably arises from melanocytes located in the epithelium of the lacrimal drainage system or the underlying stroma (7). This might be more doubtless following surgical manipulation of the conjunctival lesion. Clinical Features Lacrimal sac melanoma has the identical medical options as described in the part on clinical elements of lacrimal sac tumors. Bleeding inside the tumor can give it a darker blue look and bloody discharge from the punctum. Pathology Histopathologically, the tumor consists of malignant melanocytes, equivalent to conjunctival melanoma, previously mentioned. Malignant melanoma of the lacrimal sac complicating major acquired melanosis of the conjunctiva. Chapter 14 Tumors of the Lacrimal Drainage System 237 Lacrimal Sac Melanoma Melanoma of the lacrimal sac is similar histopathologically to melanoma of the conjunctiva. As mentioned, benign papilloma can develop in the lacrimal sac; it can evolve in some circumstances into squamous cell carcinoma. Other reported lesions embrace leukemia and lymphoid hyperplasia lymphoid (1,2), oncocytoma (3�6), hemangiopericytoma and solitary fibrous tumor (7�15), peripheral nerve tumors (16,17), cysts (18�21), and others (22�38). The clinical and histopathologic options of all lacrimal sac tumors and pseudotumors are comparable and had been discussed elsewhere. The management varies with the kind of lesion, but is generally surgical removing by dacryocystectomy and subsequent reconstruction of the lacrimal drainage system. Oncocytic adenomatous hyperplasia of the lacrimal sac: a case report and review of the literature. A rare solitary fibrous tumour of the lacrimal sac presenting as acquired nasolacrimal duct obstruction. Adenocarcinoma expleomorphic adenoma of the lacrimal sac and nasolacrimal duct: a case report. Granular cell tumor of the lacrimal sac and nasolacrimal duct: no invasive conduct with incomplete resection. Primary lacrimal sac B-cell immunoblastic lymphoma simulating an acute dacryocystitis. Leiomyoma of the orbit and periocular area: a clinicopathologic study of four cases. Mucosa-associated lymphoid tissue lymphoma in lacrimal sac of 10-year-old boy with mass in left medial canthal area. Pyogenic granuloma of lacrimal sac presenting as an outgrowth through the superior canaliculus. Histopathology of a dacryolith in an aged affected person with dacryocystitis secondary to actinomyces. It entails data of eyelid anatomy and experience with dealing with tumor tissue and beauty reconstruction. It is beyond the scope of this textbook and atlas to describe the fine details of surgical administration of eyelid tumors. In this chapter, we define some of the fundamental surgical approaches to eyelid tumors. A small trephine punch is ideal for such a biopsy, although an incisional biopsy with a scalpel is also acceptable particularly for suspected basal cell carcinoma. An incisional diagnostic biopsy is usually acceptable for malignant tumors with low metastatic potential, corresponding to basal cell carcinoma and squamous cell carcinoma. Frozen sections or chemosurgery are usually advisable to insure that margins are free of tumor before closure of the wound. A skin graft or flap may be needed in some circumstances to close the defect and minimize practical eyelid issues, corresponding to cicatricial ectropion. Donor skin may be obtained from the higher eyelid of the ipsilateral or contralateral eye, retroauricular pores and skin, or other sites, depending on the desire of the surgeon and the clinical circumstances. Larger malignant tumors could require broad surgical removing and extensive eyelid reconstruction. Some malignant eyelid tumors that invade the orbital soft tissues may require a subtotal or total orbital exenteration.
Cheap secnidazole 500 mg otcOrbital plasmacytoma can range from nicely differentiated mature plasma cells to poorly differentiated anaplastic plasma cells medications jaundice order secnidazole pills in toronto. Associated multiple myeloma is often treated with high-dose chemotherapy radiation to native lesions, systemic chemotherapy, and bone marrow transplant. Solitary orbital plasmacytoma could be treated with radiation with a positive response. Clinical Features the medical features of orbital plasmacytoma are much like those of non-Hodgkin lymphoma. It typically presents in a middle-aged to aged patient as proptosis and displacement of the eye; it has been seen in children, without myeloma (6). Orbital plasmacytoma has been the preliminary signal of inadequate chemotherapy in sufferers with recognized a number of myeloma (25). Diagnostic Approaches A patient with suspected or biopsy-proven orbital plasma cell tumor ought to undergo systemic evaluation to exclude a number of myeloma or other dysproteinemias. Like orbital lymphoma, computed tomography or magnetic resonance imaging of orbital plasmacytoma shows a diffuse or ovoid mass. Bleeding in areas of necrosis of orbital plasmacytoma can simulate orbital cellulitis clinically (5). It is more probably, however, to show erosion of bone, significantly in sufferers with a quantity of myeloma. It is possible that some instances really originate in orbital bone and secondarily affect the orbital delicate tissue. Pathology Multiple myeloma is a plasma cell neoplasm characterised by plasma cell infiltration of bone marrow and monoclonal Chapter 39 Orbital Lymphoid Tumors and Leukemias 755 Selected References 1. Inadequately irradiated solitary extramedullary plasmacytoma of the orbit requiring exenteration. Extramedullary plasmacytoma of the orbit: case report with outcomes of immunocytochemical research. IgA-associated lymphoplasmacytic tumor involving the conjunctiva, eyelid, and orbit. A 50-year-old man with a 20-year history of Waldenstrom macroglobulinemia developed a progressively enlarging, painless mass superotemporal to the left eye. Coronal magnetic resonance imaging of identical patient reveals bilateral superotemporal orbital plenty. Review of a prior small biopsy revealed diffuse non-Hodgkin B-cell lymphoma in keeping with marginal zone lymphoma of mucosa-associated lymphoid tissue. It tends to involve orbital bone however can generally be confined to gentle tissue. A 76year-old girl with a 3-year historical past of immunoglobulin G lambda a number of myeloma treated with chemotherapy developed proptosis of the left eye. Left proptosis and eyelid swelling in a 52-year-old patient with recognized a number of myeloma. Early descriptions of Burkitt lymphoma characterized it as a rapidly progressive, strong lymphoma with a predilection for the jaw and abdomen of sure African youngsters. It accounts for approximately 50% of childhood malignant tumors in East Africa (4). Only one case (American type) was identified in the series of 1,264 orbital lesions reported by the authors (5). Non-African Burkitt lymphoma presenting with oral thrush and an orbital mass in a baby. Clinical Features In the African type, orbital involvement is common secondary to invasion from the maxillary bone. Diagnostic Approaches An belly and orbital mass with proptosis and upward displacement of the globe unilaterally or bilaterally in an African child is very suggestive of the analysis. Orbital computed tomography and magnetic resonance imaging demonstrate a maxillary mass with secondary orbital involvement. Imaging of the American form normally reveals an irregular mass within the paranasal sinuses with secondary orbital invasion. Interspersed histiocytes containing phagocytosed particles trigger the basic "starry sky" appearance on low-magnification microscopy (3). Chromosomal abnormalities, notably a translocation of chromosome 8 to the long arm chromosome 14, happens in many circumstances. In common, a biopsy must be accomplished combined with tried debulking of the lesion. The tumor is extraordinarily sensitive to chemotherapeutic brokers and cyclophosphamide, vincristine, methotrexate, and prednisone are usually recommended. External irradiation (30 Gy to the affected area) can be used in circumstances that seem immune to chemotherapy. Massive bilateral orbital involvement with secondary exposure keratopathy and corneal ulceration in an African child. It occurs in about 2% of organ transplant recipients who endure intensive immunosuppression (1). It can affect a spread of tissues including central nervous system, gastrointestinal tract, cervical lymph nodes, and tonsils. It should be suspected in any immunosuppressed transplant affected person who presents with a lymphoid lesion within the orbital region. Pathology Although histopathologic and immunohistochemical traits differ, the cells are of lymphocytes of B-cell lineage. An attempt should be made to decrease the immunosuppression and allow the host immune system to recuperate. Like other orbital lymphoid tumors, small localized lesions can be excised and enormous lesions can be confirmed by biopsy and handled with irradiation. The prognosis varies with the extent of disease; some patients expertise full restoration and others have a deadly consequence. Epstein-Barr virus-associated publish transplant lympho-proliferative illness of donor origin in liver transplant recipients. Iris lymphoma in a pediatric cardiac transplant recipient: clinicopathologic findings. Correlative morphologic and molecular genetic analysis demonstrates three distinct categories of posttransplantation lymphoproliferative issues. Orbital presentation of posttransplantation lymphoproliferative dysfunction: a small case collection. Closer view shows multinodular, fleshy mass in medial aspect of conjunctiva and caruncle. Marked proptosis and conjunctival and eyelid edema in a 61-year-old man who underwent heart transplantation forty two months earlier. Axial computed tomography showing large nasal orbital mass inflicting proptosis and displacement of the globe. Histopathology confirmed an infiltrate of large B lymphocytes with immunoblastic and plasmacytic differentiation. Although the classification of leukemia is complex and continues to change, the main types are acute lymphoblastic leukemia, chronic lymphocytic leukemia, acute myelogenous myeloid leukemia, and continual myelogenous leukemia. Any form of leukemia can often have an effect on the orbit; orbital involvement is typically the primary sign of systemic disease (1�23).

Order secnidazoleBoth illnesses may cause proptosis medications descriptions secnidazole 500mg mastercard, eyelid swelling, ocular dysmotility, or a palpable mass. Angiolymphoid hyperplasia with eosinophilia of the orbit associated with obstructive airway disease. It generally happens as a diffuse, ill-defined mass in the anterior aspect of the orbit (1). It generally involves the superior orbit, although it can often have an result on the entire orbit and even extend to the other orbit (4). It has occurred within the anophthalmic orbit following enucleation for uveal melanoma and the authors speculated that its improvement was associated to the presence of the orbital implant (6). Imaging studies show a diffuse, ill-defined, gentle tissue mass which may be impossible to differentiate from nonspecific orbital inflammation lymphoma or metastatic carcinoma. The histopathologic differential analysis contains angiosarcoma, Wegener granulomatosis, Churg-Strauss syndrome, pyogenic granuloma and different comparable entities. Chapter 26 Inflammatory Lesions That Simulate Neoplasms 473 Orbital Kimura Disease A clinicopathologic correlation of orbital involvement with angiolymphoid hyperplasia with eosinophilia (Kimura disease) is depicted. Axial computed tomography exhibiting massive soft tissue involvement of the best orbit and less severe involvement of the left orbit. Note the diffuse enhancing lesions in superior lacrimal glands and surrounding tissue in each eyes. The affected person was treated with corticosteroids with poor response; the tumors have been eliminated surgically from both orbits in separate operations. Higher energy photomicrograph of same lesion, higher depicting admixture of eosinophils and small lymphocytes. Dermoid cyst was the most typical, accounting for 26 circumstances, or 37% of all cystic lesions (4). Overall, about 61% of head and neck dermoid cysts happen within the periorbital region (24). It is a congenital lesion that types from epithelial cells which are entrapped throughout embryogenesis beneath the surface epithelium, typically near bony sutures. Orbital dermoid cysts have been categorized into juxtasutural, sutural, and gentle tissue variants, with subcategories of every (5). In a clinicopathologic collection of 197 circumstances from the Oncology Service and Pathology Department of Wills Eye Hospital, it was discovered that about 70% had been positioned superotemporally at the zygomaticofrontal suture, 20% superonasally on the maxillofrontal suture, and 5% within the nasal delicate tissue; different areas had been less frequent (5). The cyst lumen accommodates desquamated epithelial cells, sebaceous materials, and hair (5). Management Management of orbital dermoid cyst ranges from remark to surgical excision, with most being eliminated surgically as a end result of the affected person presents with a visual lesion or ocular signs owing to rupture of the cyst and secondary orbital irritation. An anteriorly located orbital dermoid cyst may be excised by means of a cutaneous or conjunctival approach. If rupture happens, vigorous irrigation and instillation of antibiotics or corticosteroids is advisable to prevent postoperative inflammation. Clinical Features Orbital dermoid cyst classically occurs as a firm, fastened subcutaneous lesion near the orbital rim superotemporally in a younger youngster. Less usually, it develops at the orbital rim superonasally or in the deeper orbital gentle tissues. Such a delicate tissue nasal cyst is mostly derived from conjunctival epithelium and is sometimes call a "conjunctivoid" (8). The less common deep orbital cyst causes proptosis and/or displacement of the globe and is sometimes referred to as a "giant dermoid cyst" (12,19). The anterior dermoid can rupture spontaneously or after trauma and produce a subcutaneous inflammatory reaction that resembles cellulitis or dacryoadenitis. Diagnostic Approaches the basic dermoid cyst can usually be diagnosed based on the scientific appearance of a subcutaneous mass superotemporally on the orbital rim. Imaging studies present a cystic lesion with enhancement of the wall but no important enhancement of the lumen. Adjacent bone modifications, usually a smooth fossa, are demonstrated in about 85% of instances (17). In some cases, a dermoid cyst can have extraorbital and intraorbital components that are connected via a defect in bone (dumbbell dermoid) (7). Pathology Histopathologically, orbital dermoid cyst is lined by floor epithelium (epidermis or conjunctiva). Cysts lined by conjunctival epithelium are more usually discovered within the orbital delicate tissue nasally (8,9). The cyst wall can comprise dermal appendages, Chapter 27 Orbital Cystic Lesions 477 Selected References 1. The frequency and medical significance of bone involvement in outer canthus dermoid cysts. The posterior aspect of the cyst is commonly adherent to the periosteum, requiring meticulous dissection to take away the cyst intact. The cyst is lined by keratinizing epithelium and has dermal elements (hair follicles and sebaceous glands) within the wall (below) and in the lumen (above). It is feasible that they originate from primitive epithelium destined to form the adult caruncle. In distinction with the typical dermoid cyst proven in Plate 250, this type is generally acknowledged in older kids or adults. Photomicrograph showing wall of cyst with nonkeratinizing epithelium with goblet cells, hair shafts, and sebaceous glands. Photomicrograph exhibiting wall of cyst with nonkeratinizing epithelium containing Periodic acid-Schiff�positive goblet cells. Slight blepharoptosis and inferotemporal displacement of left eye in a 50-year-old man. Axial magnetic resonance imaging in T1-weighted picture, exhibiting temporal displacement of left eye by cystic mass. The cyst is lined by nonkeratinizing epithelium with goblet cells and has dermal components within the wall and in the lumen. Axial computed tomography exhibiting osseous defect in zygoma of left eye (to the right in the image). Surgical photograph exhibiting subcutaneous component of the cyst (retracted with forceps to the left) and the tubular part of the cyst passing by way of the bony defect (in the center). After removal of the dermoid cyst, the oval hole in the bone is clearly visualized. The part up and to the left represents the tubular intraosseous component of the lesion. Chapter 27 Orbital Cystic Lesions 483 Orbital Dermoid Cyst: Deep Orbital Type Large dermoid cysts situated in the posterior orbit pose extra of a diagnostic and therapeutic challenge. Such cysts can slowly grow to a big size at a younger age and can recur after excision. Although a lot of the cyst was lined by nonkeratinizing epithelium just like conjunctiva, a small portion of it confirmed keratinizing epithelium.
References - Stone, N., Potters, L., Davis, B. et al. Customized dose prescription for permanent prostate brachytherapy: insights from a multicenter analysis of dosimetry outcomes. Int J Radiat Oncol Biol Phys 2007;69:1472-1477.
- Matin SF: Determining failure after renal ablative therapy for renal cell carcinoma: false-negative and false-positive imaging findings, Urology 75:1254, 2010.
- Galie N, Beghetti M, Gatzoulis MA, et al. Bosentan therapy in patients with Eisenmenger syndrome: a multicenter, doubleblind, randomized, placebo-controlled study. Circulation. 2006;114:48-54.
- Rana SS, Bhasin DK, Srinivasan R, Singh K. Endoscopic ultrasound (EUS) features of mediastinal tubercular lymphadenopathy. Hepatogastroenterology. 2011;58(107-108):819-823.
- Motola JA, Urivetsky M, Molia L, et al: Transmembrane oxalate exchange: its relationship to idiopathic calcium oxalate nephrolithiasis, J Urol 147:549n552, 1992.
- Patel RA, Brolin RE, Gandhi A. Revisional operations for marginal ulcer after Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2009;5:317.
- Garnis C, MacAulay C, Lam S, Lam W. Genetic alteration on 8q distinct from MYC in bronchial carcinoma in situ lesions. Lung Cancer 2004;44:403-4.
|


