|
Dr Samuel Ajayi - Consultant Nephrologist
- Department of Medicine
- University of Abuja Teaching Hospital
- Abuja, FCT
- Nigeria
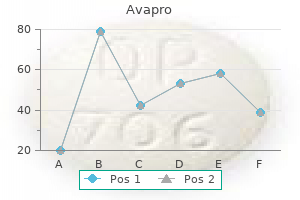
Avapro dosages: 300 mg, 150 mg
Avapro packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills
Discount avapro 300 mg lineIt is crucial to close the deeper fascia (platysma diabetes signs yahoo answers quality 150 mg avapro, superficial musculoaponeurotic system, galea) every time possible to provide energy and take rigidity off of the superficial tissues. We sometimes use 3-0 and 4-0 braided synthetic absorbable suture (Vicryl, Ethicon, Inc. In the galea, 2-0 suture may be more applicable, and 5-0 could additionally be better within the thinner nasal and periorbital tissue. Eversion: In the deep layers, exact suture placement set again from the leading wound edge will lead to eversion when the tie is made. These techniques provide dependable eversion and remove pressure from the healing edge. Skin closure: A number of techniques and materials are available, and the particular selection of fabric will rely upon a wide range of elements together with desire. Alignment and delicate tissue handling: Meticulous technique will improve the final word aesthetic outcome. The tissue depth of the course of the needle and suture should be symmetric on both sides of the wound edge. Further tissue trauma could be minimized with the utilization of skin hooks and fine-toothed forceps. The pores and skin ought to be manipulated by grasping the deeper tissues instead of the epidermis wherever potential. A corner stitch or Gillies stitch may be helpful with acute angles and trifurcations. These include lacerations through the complete thickness of the lip or vestibule from pores and skin to mucosa, as properly as tongue and oropharyngeal lacerations, which extend through the underlying musculature. Mucosal or musculo-mucosal sutures can then be used to loosely re-approximate the superficial wound, but wide spacing must be maintained and watertight closure must be avoided. Full-thickness lip and vestibule accidents should be repaired following the same ideas as above. The deeper muscle (orbicularis, buccinator) is closed, adopted by plastic repair of the pores and skin. The key maneuver is the deep suture, which reestablishes continuity of the orbicularis muscle. The pores and skin and vermillion border should be roughly realigned with some eversion or redundancy. It is worthwhile to minimize and revise this suture if the preliminary try is imperfect. The white roll and vermillion border must be precisely realigned when closing the pores and skin and vermillion. If any pedicle is maintained, an avulsed auricular or nasal section typically must be reattached. In the event of complete amputation, delayed reconstruction or use of a prosthetic is usually the best option. A, Simple interrupted sutures should be placed evenly and much enough away from the laceration edge that eversion of the pores and skin edge is achieved. B, A simple steady suture could additionally be used for lacerations that are easily approximated. C, Horizontal mattress sutures are not often used on skin however may be used for wounds that require further power, such as avulsions or gunshot wounds, and are anticipated to require revision. The surgeon should keep in mind to avoid tying the sutures too tight or the blood supply to the margins of the laceration shall be constricted. D, Running subcuticular sutures could additionally be utilized in wounds which would possibly be well approximated and cleanly lacerated. A very aesthetic closure can be achieved if the wound edges are everted appropriately. Primary reconstruction with that cartilage, a temporoparietal fascia flap, and pores and skin grafting could presumably be thought of. In delayed reconstruction the cartilage is buried underneath the dermis for preservation. Cosmetic outcomes from cartilage grafting, nonetheless, are frequently inferior to prosthetics or reconstruction utilizing a porous polyethylene implant. Due to the a number of sensory nerve contributions, peripheral blockade may be challenging, and additional local infiltration is usually required. Auricular hematoma: these are usually the outcomes of blunt trauma and should be drained acutely to prevent cauliflower ear deformity. Incision and drainage is superior to aspiration to make certain that the consolidated clot is evacuated. We prefer to mold petroleum gauze into the scaphoid fossa and safe it with a mattress suture via the total thickness of the auricle. Scalp Large scalp wounds that end in a large scalp flap can be quite impressive on examination and may find yourself in important bleeding, but restore is usually straightforward. Parallel incisions in the galea made perpendicular to the line of development can improve the stretch of a scalp flap. Care must be taken to avoid any vessels in the pores and skin flap simply superficial to the fascia. Suction drains could additionally be thought of for big potential areas and contaminated wounds. For the above more advanced injuries, oculoplastic expertise should be sought when potential. Failure to identify and handle such an damage may result in obstruction, sialocele, sialadenitis, or salivary fistula. Exploration utilizing lacrimal probes or sialendoscopy along with therapeutic massage of the gland could assist to determine a ductal harm. Ducts may be repaired with diversion and sialodochoplasty or reanastomosis over a stent. A giant angiocatheter may be used in this capability and sutured in place for a matter of weeks. In this case, botulinum toxin injection of the gland might assist to lower obstructive signs. Periorbital Injuries While most eyelid lacerations may be approached with confidence by the facial surgeon, a comprehensive discussion of oculoplastic techniques is beyond the scope of this chapter. Similar to different facial items, periorbital tissues have to be repaired with meticulous attention to the approximation of the native anatomy in layers. In the eyelid this includes the tarsal plate, orbicularis muscle, lid margin, and eyelash line. The deeper layers may be closed with 6-0 Vicryl and the skin with 6-0 nylon or fast-absorbing intestine. The conjunctiva can frequently be left open or closed partially with a few 6-0 fast-absorbing intestine sutures with a buried knot. If a laceration extends near or via the puncta, then the canaliculi should be examined with probing and doubtlessly stented for a prolonged interval. In the occasion of serious loss of tissue, the lid can be reconstructed with primary closure or with small development flaps for defects as much as 50% of the higher or lower lid Facial Nerve Injury Injury to the facial nerve should be suspected based mostly on the sort and location of trauma and confirmed by bodily examination. While older sufferers could reveal a loss of facial tone immediately following a nerve harm, youthful patients might reveal close to regular tone in the acute setting despite a very severed nerve.
Cheap 150 mg avapro fast deliveryFailure to protect the superficial temporal vessels could forfeit the use of a temporoparietal flap for reconstruction diabetes when to test your blood sugar buy generic avapro 300mg. A basal subfrontal method is most well-liked to keep away from extreme retraction of the frontal lobe. If endoscopic resection of pathology of the anterior cranial base is being undertaken, oncologic ideas ought to by no means be compromised, and the same resection should be achieved endoscopically as would be accomplished via a traditional approach. All frontal sinus mucosa should be drilled away to avoid late issues such as the formation of a mucocele. The lateral rhinotomy incision affords excellent publicity of the ipsilateral nasal cavity and paranasal sinuses with a great beauty result. The midfacial degloving approach is beneficial for tumors involving the sinonasal cavity bilaterally. Prior to any intervention, it is suggested to evaluation circumstances with a multidisciplinary tumor board. For the purpose of this chapter, most benign and malignant tumors of the anterior cranial base can be eliminated surgically. After therapy planning is finalized, approaches are determined by the surgical staff. Although limited in method to the ethmoid roof and frontal sinuses, these limitations may be resolved with the addition of a bicoronal strategy. Endoscopic transnasal techniques With improved optics and high-definition decision, endoscopic transnasal techniques could additionally be appropriate for tumors involving the nasal cavity, paranasal sinuses, and cranial base with minimal intracranial involvement or together with the bicoronal method. Bilateral orbital involvement Bilateral cavernous sinus or carotid artery involvement Gross intracranial extension Distant metastatic illness the general functional and well being status of the affected person must be thought of. Medications All drugs and supplements with antiplatelet or anticoagulating properties ought to be discontinued every week previous to surgical procedure. Prophylaxis of deep venous thrombosis with pneumatic compression stockings is provided all through the surgical procedure and hospital keep. Bone: the anterior cranial fossa consists of the frontal bone with orbital roof, the crista galli, cribriform plate, ethmoid bone, chiasmatic sulcus, and the lesser wing of the sphenoid bone including the anterior clinoid course of. Tumors that arise on this region could extend into the orbit, paranasal sinuses, or nasal cavity. Conversely, tumors arising from the paranasal sinuses and nasal cavity may also extend or invade via the anterior cranial fossa to contain intracranial buildings. This relaxes the brain and limits the need for parenchymal retraction in addition to the risk of encephalomalacia. Although the drain is normally eliminated after completion of the case, some surgeons might prefer to go away it in place for forty eight to 72 hours to decrease intracranial strain because the reconstruction heals. The affected person is placed supine on a Mayfield head holder with out pins for ease of rotation and repositioning through the process. If a bicoronal method is planned, the attention are protected with a suture tarsorraphy to forestall inadvertent harm to the corneas. The intranasal cavity, together with the inferior and middle turbinates, basal lamella, and anterior wall of the sphenoid sinus medial to the center turbinate are infiltrated with 1% xylocaine with 1:a hundred,000 epinephrine, and 0. Fellowship: the pinnacle and neck surgeon must be skilled in each open and endoscopic approaches to the anterior cranial base. The group should be prepared to control massive bleeding, although rare, from the carotid artery. Fluid resuscitation: Communication with anesthesiology on blood loss and size of surgery is obligatory for acceptable management of fluid and blood products throughout surgery to prevent hypotension and underperfusion of the brain. Preoperative and scheduled dosing of antiseizure drugs similar to levetiracetam may be helpful in sure circumstances. Scalp and flap necrosis: Protection of the supraorbital arteries and hydration of the pericranial flap with saline-soaked gauze will limit injury. Facial nerve injury: the temporal branches are at risk with elevation of the scalp. Orbital injury: Inadvertent injury to the ophthalmic artery can result in blindness. Vancomycin if the affected person is allergic to penicillin or cephalosporins Monitoring None necessary Instruments and Equipment to Have Available 1. Various handpieces and drill bit sizes are available for open, craniotomy, and skull base entry. Endoscopic pistol-grip Hemoclip applier Surgical Technique Bicoronal Approach � Vasoconstriction the planned incision is infiltrated with 0. Using a curved hemostat to separate the tissue layers, the lateral incision is prolonged to the fascia of the temporalis muscle (deep temporal fascia). The coronal scalp incision could additionally be prolonged in a preauricular skin crease to present further lateral exposure. Preservation of the artery is essential for sustaining the blood supply to the temporoparietal fascial flap and to the scalp in revision surgical procedure and post-radiation therapy. The pericranial flap is incised in a U-shaped trend primarily based on the supraorbital and supratrochlear vessels. If exposure of the lateral orbital rim is critical, a horizontal incision is made in the outer layer of the deep temporal fascia several centimeters above the zygomatic arch. Elevation continues in this adipose layer to the zygomatic arch, thereby avoiding harm to the frontozygomatic branches of the facial nerve. If the orbital rim must be eliminated for a subfrontal method, the periorbita is elevated in a subperiosteal aircraft medially to the frontoethmoid suture line and laterally to the inferior orbital fissure. The temporalis muscle is elevated from the temporal bone toward the temporal fossa. A small cuff of periosteum is left on the margins to reapproximate the muscle during closure. Traction sutures or hooks are then used to reflect the scalp, pericranium, and temporalis muscle and secured to the surgical drapes for consistent exposure. A moist laparotomy towel is placed over these tissues to keep away from desiccation and loss of tissue. Neurosurgical methods for publicity of intracranial contents are past the focus of this chapter but may be present in numerous textbooks on neurosurgery. Exposure permits launch of the septum from the anterior cranial base, and elimination of the lamina papyracea detaches the lateral nasal wall and maxilla from the orbital roof. The pericranial flap is dissected from the galea by sharp dissection to the level of the orbital rim. The scalp is elevated to the orbital rims with preservation of the supraorbital neurovascular bundle (arrowheads). The vascular pedicle of the pericranial flap depends on the supraorbital vessels (arrows).
Buy avapro 150mg amexTongue flap � Available when beforehand talked about techniques have failed � Endoscopic surgery contains removal of polypoid mucosa and any foreign our bodies in the sinus diabetes symptoms over 50 buy avapro 300 mg visa, together with enlargement of the maxillary sinus ostium to ensure enough sinus drainage. The bone is recessed superiorly to ensure removing of all necrotic bone and epithelial components of the fistulous tract. Purulent drainage from oroantral fistula famous in alveolar crest associated with tooth #3. Avelox, if history of antibiotic-associated colitis to clindamycin and resistance to penicillins d. Use of acrylic, clasp-retained postoperative splint, if fabricated, to defend the palatal tissues for 14 days four. If closure fully opens, plan for secondary closure with various flap design. Implement an appropriate antibiotic after incision and drainage, tradition, and assessment of the sensitivity of purulence. The well-known Caldwell-Luc process, which was first described in the Complications 1. The resulting mucosal defect within the palate is allowed to granulate and heal by secondary intention. An acrylic splint fabricated preoperatively can enhance patient comfort over the palate, particularly throughout eating. Additional analysis of the anterior ethmoid cells is critical to ensure removal of residual illness and to stop recurrence. True inflammatory polyps and international our bodies such as tooth roots are subsequently removed from the maxillary sinus. Computed tomography scan demonstrating an oralantral fistula with obstruction of the maxillary sinus. Adequate intranasal drainage to either the middle meatus or the inferior meatus should be achieved to ensure success when the fistula is closed. Untersuchungen uber Massverhaltnisse des Oberkiefers mit spezieller Berucksichtigung der Lagebeziehungen zwischen den Zahnwurzeln und der Kieferhohle. Correlation between the development of an oroantral fistula and the size of the corresponding bony defect. Editorial Comment In bigger oroantral fistula defects, vascularized tissue reconstruction is important to long-term success. Similar to fistulas current in the upper aerodigestive tract and skull base, the utilization of vascularized reconstruction has elevated the overall success fee of the procedure. In the case of a palatal rotational finger flap, the exposed exhausting palate will re-epithelialize shortly if the appropriate postoperative precautions are taken. The position of concurrent maxillary antrostomy is increasingly acknowledged in bigger defects, as this allows for physiologic management of the sinus and prevents postoperative mucosal irritation and secondary obstruction from hindering the repair. Reasons for failure of oroantral fistula repair embrace each of the following, except a. A slender flap base because of converging releasing incisions in the flap design d. Scoring the periosteum to enable for development of the flap in a tension-free method 2. Each of the next postoperative instructions improves successful closure of the defect, except a. Not reestablishing drainage of the sinus by widening the ostium within the center meatus c. Management of an oroantral fistula should take into accounts the degree of disease within the involved maxillary sinus. Maxillary sinusitis of dental origin because of oroantral fistula, treated by endoscopic sinus surgery and first fistula closure. The presence of intranasal plenty, ulcers, or areas of contact bleeding may suggest a malignant tumor. Soft tissue swelling of the face may indicate tumor extension by way of the anterior bony confines of the nose and sinuses. Inferior extension towards the oral cavity could current with an ulcer or a submucosal mass in the palate or the alveolar ridge. Middle ear effusion may indicate tumor involvement of the nasopharynx, Eustachian tube, or tensor veli palatini muscle. Extension of the tumor to the skull base might result in involvement of the cranial nerves producing anosmia, blurred imaginative and prescient, diplopia, or hypothesia along the branches of the trigeminal nerves. Visual loss secondary to optic nerve involvement is often a late sign, although extra refined signs of optic nerve dysfunction, together with afferent pupillary defect, lack of colour vision, and visual subject defects, are more regularly encountered. Medial maxillectomy is mostly indicated for resection of tumors of the nasal cavity, lateral nasal wall, and medial maxillary sinus. This offers one of the best publicity for a medial maxillectomy and can be combined with a transcranial approach for an anterior craniofacial resection generally used for removing of superior tumors of the anterior skull base. The midfacial degloving method is mostly used within the management of enormous benign lesions of the sinonasal region and cranium base similar to juvenile nasopharyngeal angiofibroma, for selected malignancy in this space, and to afford entry to the nasopharynx and infratemporal fossa. The main benefit of the "degloving" approach is that an exterior facial incision is averted. Another advantage is providing simultaneous exposure to the inferior and medial maxilla, bilaterally. This is especially helpful when approaching tumors with bilateral involvement of the nasal cavity and maxillary sinus. A main drawback, however, is the restricted superior and posterior publicity and the necessity for fixed retraction of the gentle tissue envelope for continued enough exposure. Endonasal endoscopic medial maxillectomy and sphenoethmoidectomy may be also performed and supply wonderful visualization for appropriately selected tumors. Regardless of the approach, medial maxillectomy contains elimination of the lateral nasal wall and the medial aspect of the maxillary bone bounded laterally by the infraorbital nerve. Imaging � Imaging is very helpful in obtaining pretreatment data regarding the location, measurement, and extent of the first tumor, in addition to the presence of regional and distant metastasis. Such information is important in deciding on therapeutic choices and for proper preoperative planning of the optimum surgical strategy. Coronal images finest delineate involvement of the orbital walls and invasion of the skull base, notably the cribriform plate. Axial images are notably helpful in demonstrating tumor extension by way of the posterior wall of the maxillary sinus into the pterygopalatine fossa and infratemporal fossae. Sagittal pictures are particularly helpful in evaluating extension alongside the cribriform plate, planum sphenoidale, and clivus. Bone destruction and invasion of soft tissue counsel an aggressive lesion, normally a malignant neoplasm.
Buy avapro pills in torontoFor most maxillary tumor surgical procedure blood sugar problems purchase discount avapro, the patient may be managed with an oral intubation and extubation. Exceptions to this rule could embrace patients with extreme trismus, sufferers who require giant pharyngeal or taste bud resections, and patients that may want free flap reconstructions of the palate defect. These patients could require an awake or elective tracheostomy for safe airway management. The inside maxillary artery is the primary blood supply on this space; nevertheless, the inferolateral trunk of the carotid artery can also present blood provide into the infratemporal fossa. Paralysis is usually acceptable unless a parotidectomy or neck dissection is needed with the maxillectomy, in which case it will be contraindicated. We also try to be considerate in regards to the fluid intake over the course of these operations, since they are often prolonged. Either a hundred and eighty levels rotation (our preferred) or somewhat past ninety levels to the side of the proposed maxillectomy. This removes the anesthesia staff from the top and allows the surgical group to be on all sides of the top, permitting for higher sight traces and retraction. The neck is always prepped into the sphere in case proximal vessel management or neck dissection is needed. Incisions are marked with the pure pores and skin creases in mind, together with the planned wants for publicity. Perioperative antibiotic prophylaxis: Standard first- or second-generation cephalosporin or penicillin-based antibiotics are given 30 minutes earlier than the incision. Monitoring: Usual basic anesthesia monitoring Instruments and Equipment to Have Available � � � � � � � � Soft tissue and neck dissection set Small bone saws Side chopping pencil drill Bone chisels Dental extraction set Oral retractors Monopolar and bipolar cautery Endoscopic equipment: 0- and 30-degree Hopkins-rod nasal endoscopes and endoscopic tower must be out there Key Anatomic Landmarks En bloc resection and attaining adverse margins remain a steadfast principles in oncologic surgery and are sometimes the vital thing to one of the best patient outcomes. However, achieving this goal may be difficult within the orbit and alongside the periorbita, if the cancer has extended either intraconally or posteriorly into the infratemporal fossa. As outlined later in this chapter, a eager understanding and awareness of crucial landmarks within the maxillectomy method enable for an easier dissection when working with superior tumors. Fully expose the anterior bony surface of the midface, inferior and lateral orbit, and buccal area. Make an incision alongside the piriform aperture into the intranasal cavity, and retract the nostril to the opposite side. Closely study the orbital flooring and periorbita to be sure that the most cancers has not invaded into these constructions. Using a 1-mm facet chopping pencil grip drill and copious irrigation, the anterior and periorbital osteotomies can be made. These osteotomies normally lengthen from the superior piriform aperture through the orbital rim for a complete maxillectomy. At the identical time as the globe is retracted superiorly, a thin, sharp osteotome is used to connect the medial and lateral orbital rim osteotomies extending posteriorly into the orbit liberating the ground of the orbit. Using the same pencil drill, an osteotomy is created from the lateral orbit, through the rim, and increasing throughout the malar process or occasionally through the zygomatic arch. This osteotomy extends posteriorly towards the pterygoid plates and all through the lateral buttress. Using a skinny reciprocating saw, the palatal osteotomy is made in a posterior to anterior direction and subsequently extended into the anterior nasal cavity. The normal approach to remove the plates is through the use of a curved osteotome placed behind the plates and angled up into the infratemporal fossa. This technique has two limitations, including lack of proximal management of the internal maxillary artery and inadvertent fracture at the stage of the pterygopalatine fossa instead of behind the plates. Using blunt dissection, the pterygoid plates and muscle tissue can be recognized, and infrequently the inner maxillary artery could be palpated and instantly managed with a hemostat if necessary. The junction of the fused portion of the pterygoid plates can be palpated at the base of the middle cranial fossa. Using a sharp straight osteotome, this fused portion could be fractured from the underside of the sphenoid bone, and the complete maxilla may be rocked medially and inferiorly. The infratemporal fossa is now uncovered so that the internal maxillary artery could be absolutely managed and the pterygoid muscular tissues could be dissected from the bone with bipolar electrocautery, which permits for liberating of the entire maxilla and pterygoid plates from the infratemporal fossa. V3 can typically be recognized, and, if wanted, neural margins could be taken from the cranium base. Using large curved scissors, the rest of the medial maxillary wall is cut posteriorly from the medial orbital osteotomy, across the duct and inferiorly toward the torus tubarius, and the complete specimen is removed. Intraoperative delicate tissue margins are then despatched for frozen part examination, and bleeding is subsequently managed. A medium-thickness cut up thickness pores and skin graft is taken from the thigh, placed over the exposed buccal contents, and draped posteriorly into the infratemporal fossa defect. The facial incisions are then closed in a quantity of layers, with care taken to reapproximate the orbicularis oris and oculi. Common Errors in Technique � Obtaining insufficient and superficial bony margins (which should extend at least 1 to 1. A and C, Lateral rhinotomy incision, B, lateral rhinotomy with lip split incision and D, modified Weber-Ferguson incision. Several modifications of the incisions can be made: B is a lip-splitting extension with dart, and the dart offers some potential benefits for lip notching. This has potential cosmetic benefits, in addition to placing the incision over the nasal bones, an area that can have much less contact with the intranasal air containing areas. D is the periocular extension (a Weber-Ferguson incision) that enables for lateral and orbital access. In the aged, corresponding to in this cadaveric specimen, the writer makes this incision on the inferior orbital rim; nevertheless, in a youthful affected person, a subciliary or transconjunctival incision is most well-liked (dashed blue line). Wound problems from facial incisions Free flap failure Corneal ulceration Bleeding or hematoma formation Vision loss and/or diplopia this requires emergent ophthalmology consultation to consider for elevated pressures or optic neural loss. If orbital pressures are greater than 30 and the patient has lack of visible acuity, an emergent canthotomy and cantholysis could additionally be warranted. Additionally, imaging may be required to evaluate for a retrobulbar hematoma and plan for any wanted decompressive operations. Lastly, beginning trismus therapy early within the postoperative period is essential, for the rationale that muscles of mastication can scar during the therapeutic interval. A, Healed frontal view of a affected person 5 years after a WeberFerguson incision and complete maxillectomy. Note the nice alignment of the nose and lip and the dental rehabilitation that the ultimate obturator offers. One of the central rules of oncologic surgery is that tumor resection should be complete at each the microscopic and macroscopic level, which is mostly achieved intraoperatively by way of acquiring frozen sections to verify adverse surgical margins. With regard to sinonasal and anterior cranium base malignancies, obtaining surgical margins can be technically challenging and sometimes is most likely not possible given the proximity of important neurovascular constructions. Subsequently, it has been shown that in 30% and 24% of sinonasal neoplasms resected via open and endoscopic approaches, respectively, residual microscopic disease has been left due to the proximity to such constructions as the internal carotid artery and optic nerve.
Order avapro lineThe posterior incision in the pericranium is positioned a couple of centimeters posterior to the initial pores and skin incision diabetes symptoms in toddlers order avapro with american express. This dissection reduces the chance of injury to the temporal department of the facial nerve. This is very important if the superior sagittal sinus is adherent to the cranium. The frontal sinus infundibulum is obliterated using a combination of items of temporalis muscle, fascia, and fibrin glue. A, A high-speed drill is used to create three burr holes, as described within the "Surgical Technique" section. The image shows the creation of a midline burr gap at the level of the hairline. Notice the perpendicular orientation of the drill shaft and continuous irrigation. A, the frontal sinus is exposed, and, B, the posterior wall of the frontal sinus is eliminated utilizing rongeurs and a high-speed drill as needed. A, the posterior wall of the frontal sinus has been eliminated, and both frontal sinus infundibula are exposed. The frontal bone flap is changed in the anatomic position and is secured with mini-plates. Attempts to go lower than what the sinus will enable will merely erode the anterior aspect of the frontal bone, leaving an ugly gap upon alternative of the bone flap. Patients may also complain of decreased visual fields and tension complications and report seeing their eyebrows in their visible field. The pericranial flap should relaxation on bony structures such as the roof of the orbita and planum. If not infected, the advice is to take away the mucocele to forestall problems in the future. Despite the arrival of endoscopic methods, extreme traumatic disruption of the posterior table and malignancies that stretch anteriorly in the frontal sinus are often best managed with this procedure. While conceptually straightforward, the many nuances highlighted on this chapter, together with careful placement of the craniotomy, differential dissection to preserve the adipose tissue pad containing the frontal department of the facial nerve, and allowing adequate house for the vascular pedicle of the pericranial flap below the anterior desk, are critical for the useful and aesthetic consequence of the procedure. Meticulous removing of the entire posterior table and the mucosa from the frontal sinus is crucial and is usually essentially the most difficult in extremely pneumatized frontal sinuses with giant supraorbital ethmoid cells. Finally, obliteration of the frontal outflow tract can be performed with quite so much of substrates and is commonly surgeon dependent. However, autologous grafts are usually favored, as publicity of porous foreign materials to the sinonasal cavity may find yourself in long-term infectious issues. Twenty-six-year experience treating frontal sinus fractures: a novel algorithm primarily based on anatomical fracture sample and failure of typical techniques. Cranialization in a cohort of 154 consecutive sufferers with frontal sinus fractures (1987-2007): evaluate and replace of a compelling process within the chosen patient. Cranialization of the frontal sinus for secondary mucocele prevention following open surgery for benign frontal lesions. There is a scarcity of literature evaluating the outcomes between frontal sinus obliteration and cranialization. The frontal sinus lesions handled had been osteoma, mucocele, encephalocele, and fibrous dysplasia. Patients who developed mucocele in the obliteration group had been handled with frontal sinus cranialization, and none of those sufferers required a second revision surgical procedure. Malignant tumor of the anterior cranium base with erosion of the posterior table of the frontal sinus. Which of the following is the least doubtless complication following frontal sinus cranialization Etiologic classification can be subdivided into traumatic and nontraumatic origin. Most methods yield comparable ends in experienced arms, as confirmed by a meta-analysis of the literature by Hegazy et al. Imaging � Biochemical testing is indicated to verify the true nature of the nasal drainage and ought to be carried out prior to ordering expensive imaging tests. Coronal computed tomography cisternogram demonstrating a posttraumatic cerebrospinal fluid fistula (arrow) of the proper cribriform plate. Coronal computed tomography cisternogram demonstrating bilateral tegmen defects with distinction penetrating existing defects (arrows). Sagittal magnetic resonance imaging demonstrating a large meningoencephalocele (arrows) of the anterior cranial base. Positioning � the affected person ought to be supine, in reverse Trendelenburg position, to lower bleeding and improve visualization. Key Anatomic Landmarks � the positioning of the leak determines which landmarks are most essential. Prerequisite Skills � the surgeon should have the power to carry out an intensive endoscopic sinus operation, including a large sphenoidotomy and frontal sinusotomy. Endoscopic Management of Cerebrospinal Fluid Leaks 771 � � � � � � � Anteriorly the uncovered adipose tissue is covered with a layer of Surgicel (Ethicon, Neuchatel, Switzerland) followed by Gelfoam, and the nose is filled with �-inch nasal strip that has been impregnated with antibiotic ointment or with the inflated balloon of a Foley catheter. Alternatively, commonplace techniques corresponding to inlay grafts with fascia lata, adopted by the previously described nasoseptal flap, have been very efficient in repairing these defects. The risk of unintentional damage to adjoining neurovascular structures is a critical consideration when coping with defects of the lateral wall of the sphenoid sinus; sufficient visualization of this area is necessary. Repair often requires ligation of the sphenopalatine artery and extension of the sphenoidotomy towards the pterygopalatine fossa. The transpterygoid strategy could be mixed with an endoscopic medial maxillectomy as necessary, to allow sufficient vary of motion and visualization of even probably the most lateral of sphenoid defects. Failure to use the complete length of the nasal septum could lead to a flap of insufficient size. Coronal computed tomography scan of the sphenoid sinus depicts the boundaries of visualization of a conventional sphenoidotomy (green dots). The medial pterygoid plates (yellow arrows) are helpful anatomic landmarks and a defect within the cranium base (grey arrow). The lateral recess of the sphenoid sinus can be visualized with a trans-pterygoid approach (red dots), and dissection is facilitated with a bilateral method with removing of the sphenoid rostrum and posterior septum. High-Pressure Hydrocephalus � Normal intracranial stress ranges from 5 to 15 cm of water when the affected person is in supine place. Axial computed tomography scan of the head in a patient with high-pressure hydrocephalus and ventriculomegaly of the temporal horns. Endoscopic Management of Cerebrospinal Fluid Leaks 773 Complications � Postoperative epistaxis could require packing if ongoing and uncontrolled with topical decongestants. For bigger defects, superior outcomes are achieved using vascularized tissue for reconstruction. A novel reconstructive approach after endoscopic expanded endonasal approaches: vascular pedicle nasoseptal flap. Management of cerebrospinal fluid rhinorrhea: an evidence-based evaluate with recommendations. A mucosal inlay graft is an efficient first-line repair and should be covered with a vascularized flap if attainable.
Syndromes - Might be pregnant
- Muscles are very tense, then very relaxed
- Numbness
- Tell someone to call 911 while you begin first aid.
- Muscle twitches
- Yellow skin or eyes
Purchase avapro 150 mg otcWhich of the following is an absolute contraindication to a surgical intervention in cervical esophageal cancer Endobronchial ultrasound could additionally be used to evaluate intrathoracic lymph node metastasis diabetes symptoms early discount generic avapro uk. Reconstruction of the pharyngeal wall by free switch of greater omentum and stomach. Long-term outcomes of definitive radiochemotherapy in domestically advanced cancers of the cervical esophagus. Larynx-preserving restricted resection and free jejunal graft for carcinoma of the cervical esophagus. Functional outcomes and donor web site morbidity following circumferential pharyngoesophageal reconstruction utilizing an anterolateral thigh flap and salivary bypass tube. Experimental use of free gastric flaps for the repair of pharyngoesophageal defects. Review of 346 patients with free-flap reconstruction following head and neck surgical procedure for neoplasm. Surgical administration of carcinoma of the hypopharynx and cervical esophagus: analysis of 209 cases. One-stage reconstruction of complex pharyngoesophageal, tracheal, and anterior neck defects. Population-based studies have been contradictory relating to the impact of snoring on mortality, cardiovascular disease, metabolic syndrome, and stroke. Snoring is the most common presenting symptom in sleep-disordered respiration sufferers, and due to this fact otolaryngologists ought to pay attention to the correct workup in addition to procedures and therapies obtainable to deal with this condition. Oral appliances have been shown to significantly reduce loud night breathing, theoretically by growing the size of the pharyngeal airway in each the lateral and the anterior-posterior dimensions. Snoring is attributable to the vibration of soppy tissues within the higher airway during respiration; these vibrations are exacerbated by sleep-related rest of upper airway dilator muscles. The source of vibration is typically the flutter of the soft palate but can theoretically be anywhere alongside the upper airway. As a majority of snoring originates at the taste bud, the main target of the remainder of this chapter shall be on awake, office-based palatal procedures. All of those procedures have the tip goal of stiffening and/or reorienting the palate such that inhalation-induced vibration might be less more doubtless to occur. Aggravating elements 1) Position 2) Medications 3) Alcohol consumption 4) Weight acquire c. Sleep historical past: A full sleep historical past is warranted to assess for attainable underlying and/or accompanying sleep issues. Medical sickness: the patient have to be wholesome enough to tolerate an in-office process. Social history 1) Nicotine use: Abstaining from nicotine may assist preserve a regular general sleep-wake cycle. Snoring procedures must minimize morbidity and protect operate, especially as snoring is mostly thought-about to be medically benign. Relative contraindication: Obesity is related to decrease success rates for loud night time breathing procedures; this must be discussed preoperatively. Comorbid sleep disorders also needs to be addressed previous to procedures for primary snoring. In the following years, a number of much less invasive, functional versions of the process had been developed. Though this procedure served to successfully stiffen the palate, the resulting scar was shown to slender the space between the tonsillar pillars laterally. This process appears to be particularly fitted to patients with obstruction at the genu of the soft palate. Allergy testing: In loud night breathing sufferers with symptomatic nocturnal nasal obstruction and symptoms of allergic rhinitis, allergy testing might indicate a reversible trigger. Anesthesia � Local: If the patient requires solely soft palate and uvula interventions, this process may be carried out underneath local anesthesia in the office setting. When tonsillectomy is required, the anterior palatoplasty may be carried out under general anesthesia on the time of tonsillectomy. Positioning � Seated: the affected person must be sitting upright, at a degree the place the surgeon can comfortably visualize the oral cavity and oropharynx. The cooperative patient may assist with exposure by holding his or her personal tongue depressor(s). Primary snoring within the setting of serious burden on the affected person or bed companion Contraindications 1. The redundant mucosa could additionally be grasped with forceps and truncated at the distal aspect of the musculus uvulae. This step could serve to widen the gap between the tonsillar pillars laterally. B Operative Risks and Common Errors in Technique � Over-resection of the uvula: It is prudent to depart the muscular facet of the uvula intact for max preservation of function. A, Preoperative, B, intraoperative, and C, postoperative look of anterior palatoplasty. Thus this procedure may be significantly advantageous for the patient with a thick taste bud. Additionally, the most secure space to deal with is at or close to the midline, the place the palatal bulk is the greatest. For information on anesthesia, positioning, and perioperative antibiotic prophylaxis, see part "Anterior Palatoplasty. The first mark ought to be positioned in the midline 1 cm beneath the border of the hard palate; the lateral lesions should each be positioned approximately 1 cm away from the preliminary mark, just above the superior pole of the tonsil on both side. Adjacent radiofrequency purposes should be placed a minimal of 8 mm apart to avoid lesion overlap and subsequent mucosal harm. Generous native injection serves to enhance interstitial volume and thus lower the chance of tissue injury. The superior surface of the soft palate may be visualized with a versatile scope throughout lesion technology; any mucosal blanching during ablation signifies that the needle is too deep and must be withdrawn. For the temperature-controlled units, an power level of four hundred to seven-hundred joules must be used for midline/paramedian lesions; 300 to 350 joules will suffice for lateral lesions, where the palate is typically thinner. When utilizing plasma-mediated ablation, 10 to 15 seconds of coblation at an influence setting of 6 is acceptable for every lesion. The implants themselves as properly as associated scarring serve to stiffen the soft palate. There are some anatomic preprocedure considerations for sufferers present process palatal implantation.
Order avapro 150mg on-lineOther: Are there any other related signs diabetic honeymoon discount avapro 150 mg on line, like autophony or the Tullio phenomenon Medical sickness 1) Is there a previous history of perforated tympanic membrane, pressure equalization tubes, otitis externa, otitis media, or cholesteatoma Surgical historical past 1) If the affected person has undergone earlier otologic surgery, determine the extent and type. Evaluation of each ears 1) the integrity of the tympanic membrane and middle ear house is evaluated. Diffusion weighted imaging methods can be utilized for prognosis of cholesteatoma in difficult circumstances. Indications Conductive hearing loss may result from trauma, chronic Eustachian tube dysfunction, congenital anomalies, chronic otitis media, cholesteatoma, tumors of the center ear area, or ossicular chain fixation resulting from tympanosclerosis. When the ossicular chain have to be disarticulated for access to other middle ear pathology 3. Hydroxyapatite partial ossicular replacement prosthesis making direct contact with the tympanic membrane. Tuning fork testing with 256-, 512-, and occasionally a 1024-Hz fork is performed to decide whether conductive hearing loss is current and to estimate the diploma of loss. Primary inflammation of the skin of the external canal or inflammation secondary to illness from the middle ear requires medical management to optimize postoperative therapeutic. Patients with an intact tympanic membrane, no historical past of persistent ear disease, and progressive conductive hearing loss most probably have otosclerosis (see Chapter 133). The patient is in supine place with the top rotated away from the affected ear. Adjust the height of the table and microscope so that the surgeon is snug in a seated position, with his or her arms in a relaxed position and never totally prolonged. Cefazolin is mostly used as a result of wonderful staphylococcal and streptococcal coverage. The tympanomeatal incision for exploratory tympanotomy should be 4 to 5 mm away from the posterosuperior annulus. Binocular microscope Complete mastoid and center ear set Monopolar and bipolar electrocautery Full complement of otologic prostheses in stock 7. Postoperative canal stenosis Surgical Technique the approaches to and strategies for tympanic membrane grafting are reviewed in Chapter 131. Frequently, the preoperative standing of the ossicular chain is unknown when correction of conductive listening to loss is undertaken. This might embody ankylosis of the top of the malleus and body of the incus to the scutum, immobility of the incudomalleal joint, or calcification of the anterior malleus ligament limiting its movement. Binocular microscopic otoscopy Thorough understanding of temporal bone anatomy Tympanoplasty strategies Stapedectomy and/or stapedotomy techniques Operative Risks 1. The body of the incus is disarticulated from the top of the malleus and extracted with cup forceps. More generally, the long course of and lenticular means of the incus are eroded or linked by a fibrous union. A variety of methods are available for modification of the incus to provide a mobile yet firm connection from the stapes superstructure to the malleus. The surgeon ought to note the status of the center ear mucosa and the connection of the malleus to the stapes. The position of the malleus relative to the stapes determines how the incus might be sculpted to perform an interposition. Right, Reconstruction requires augmenting the vertical height of the stapes and its anterior span to the malleus. The body of the incus can be sculpted in a wide range of types to accommodate every particular relationship between the malleus and stapes. The height and floor area of the pinnacle of the stapes may be augmented to make higher contact with the tympanic membrane. Reconstruction from the undersurface of the malleus to the cell stapes footplate provides a safer connection of the ossicular chain. An autograft incus sometimes provides sufficient length to meet these requirements. The size of the sculpted incus may be varied based on use of the quick or long process from the footplate to the body of the incus. The identical philosophy applies to intensive tympanosclerosis of the footplate when a tympanic membrane perforation or continual otitis media is present. B, the sculpted incus has an oval aperture that fits snugly on the stapes (arrow). C, In a left ear, the incus has been positioned superior to the stapes and medial to the malleus handle. Intraoperative photograph of an Applebaum prosthesis placed between the stapes and an eroded lengthy process of the incus. B, the long process is flattened, and the notch for the malleus handle is on the superior surface of the incus. Ossicular Chain Reconstruction 899 � It is uncommon to have such intensive illness but nonetheless have an intact incus. Patients requiring lateral graft tympanoplasty (tympanic membrane reconstruction) normally have an outer and inside rosebud packing in place. Bleeding, infection, ache, scar, harm to adjacent buildings, want for revision procedures 2. Patients are instructed to hold the ear freed from water and avoid blowing the nostril or other forms of Valsalva maneuvers. Patients should keep away from significant adjustments in atmospheric stress, similar to during an air flight, for a quantity of weeks postoperatively. Parents are inspired to limit pediatric sufferers from partaking in gymnastic or other excessive bodily activities. Patients undergoing a sort V reconstruction (prosthesis to the vestibule) are to avoid heavy lifting. The procedure has been executed for the previous sixty five years, with the most important change being the design and materials of the prostheses used. Time has proven this to be an evolving course of making an attempt to maximize successful surgery and hearing outcomes. The concept of staging a procedure for the purpose of optimizing the place of the tympanic membrane and well being of the middle ear space has turn into more and more necessary in sufferers with persistent otitis media or cholesteatoma. The ongoing influence of Eustachian tube operate have to be anticipated in the course of the postoperative and long-term durations following tympanoplasty and ossicular reconstruction. The learning curve for execution could be temporary, however reaching constant well-healed outcomes, with excellent hearing outcomes, is the profession focus of otolaryngologists performing this surgery. Ossicular reconstruction for incus long-process defects: bone cement or partial ossicular alternative prosthesis.
Buy avapro pills in torontoAfter the navigatable catheter has been moved into position the probe is removed diabete in pregnancy buy avapro 300 mg with mastercard, and biopsies can be obtained by way of the catheter. Bronchoscopy can be used for placement of endobronchial catheters for brachytherapy. Bronchoscopy can be utilized to facilitate placement of oral or nasal endotracheal tubes, significantly in patients with a tough airway because of upper airway abnormalities or restricted neck flexion or in sufferers who must bear an awake intubation. Bronchoscopy can be routinely used to verify the right positioning of double-lumen endotracheal tubes. Patients present process inflexible bronchoscopy have to have the power to tolerate general anesthesia. Patients with restricted neck flexion may not be ready to be positioned adequately to enable secure passage of the rigid bronchoscope. In patient with hypoxia requiring excessive concentrations of oxygen, laser ablation of endobronchial lesions is contraindicated because of the chance of airway fireplace. The patient must be fluid resuscitated and hemodynamically secure for anesthesia. Any coagulopathy must be treated with vitamin K and blood elements, as appropriate, previous to intervention. Appropriate imaging must be performed and instantly out there for evaluation within the operating room during the process. Depending on the diagnosis, the patient and his or her family need to pay attention to the gravity of the state of affairs, potential morbidity or mortality associated with the procedure, and potential need for postoperative ventilation. Connection of rigid scope to ventilator circuit with occluding window on the end of the bronchoscope. In sufferers present process bronchoscopy for retained secretions and respiratory insufficiency when one is making an attempt to keep away from intubation, normally local remedy alone is undertaken. Rigid bronchoscopy requires common anesthesia, and several choices of air flow can be found. In such circumstances, anesthesia is saved light enough that the patient is spontaneously breathing until such time as the inflexible scope is in place in the airway. The drawback is the shortage of muscular leisure, which can preclude protected atraumatic passage of the inflexible scope. With this system the ventilatory circuit is intermittently connected to the scope to ventilate the patient. If a big air leak is current, one might have to occlude the mouth and nose with a hand or pack the oropharynx with moist gauze packing. The viewing end of the scope is covered with a glass lens, and the ventilatory circuit is attached to a aspect port on the scope. It permits for uninterrupted viewing through the scope, however opening the port for interventions will interrupt the ventilation as it opens the ventilatory circuit. This is the preferred and the most common mode of ventilation during the efficiency of rigid bronchoscopy. For versatile bronchoscopy, one should be facile with operation of a flexible endoscope. For endobronchial ultrasound, one have to be acquainted with the ultrasound look of mediastinal lymph nodes and adjacent vascular buildings. For rigid bronchoscopy, one ought to be facile with laryngoscopy and oral tracheal intubation. Preoperative Antibiotic Prophylaxis Prophylactic antibiotics are generally not required. Risk of hemorrhage with endobronchial biopsy that will overwhelm the restricted suction capacity of the flexible bronchoscope. Tracheal damage, significantly if dilating the airway, which might produce a pneumothorax or pneumomediastinum Monitoring 1. An assortment of endotracheal tubes Lidocaine and a slip tip syringe for airway topicalization and aerosolization of the pharynx Suction catheters and biopsy forceps and graspers for the rigid bronchoscope. If appropriate for the process, olive tip tracheal dilators also wants to be available. An assortment of graspers and retrieval baskets for removing of foreign bodies Flexible biopsy forceps for the flexible bronchoscope Adjustable peak stool on wheels for rigid bronchoscopy Laser and laser fiber for instances of hemoptysis Fluoroscopy tools for instances of endobronchial stent deployment or electromagnetic navigational bronchoscopy Surgical Technique 1. Endobronchial ultrasound Need to be acquainted with endoscopic ultrasound visualization of the mediastinal structures, as nicely as passing the needle sheath apparatus and aspirating three. Electromagnetic navigational bronchoscopy Need to be facile with driving the directable catheter to the location of curiosity with the help of the program software. Also must be competent in passing the various biopsy needles, brushes, and forceps by way of the directable catheter once locked in place four. Operative Otolaryngology: Bronchoscopy a hundred thirty five is breathing spontaneously, after which the bronchoscope can be safely eliminated. While drawing back the rigid bronchoscope on termination of the procedure, the proximal trachea, larynx, and pharynx may be examined. Not adequately topicalizing the pharynx and cords with peroral bronchoscopy prior to introduction of the bronchoscope 3. Passage of the rigid scope by way of the mouth with protection of the higher teeth with the thumb. Patients must be monitored postoperatively in the recovery room or the intensive care unit, if indicated, for any indicators of airway compromise because of laryngeal edema or pharyngeal or lingular damage secondary to introduction of a rigid bronchoscope. A chest radiograph must be carried out to rule out pneumothorax or pneumomediastinum following instrumentation with the rigid bronchoscope. Using a Yankauer suction, the pharynx is cleansed of any saliva that may obscure visualization of the epiglottis and the vocal cords. Advance the bronchoscope posterior to and distal to the epiglottis and then raise the bronchoscope anteriorly to visualize the arytenoids and the vocal cords and the glottic opening. External strain may be positioned on an anteriorly positioned larynx to facilitate visualization of the vocal cords. An alternative approach is to visualize the vocal cords with a handheld laryngoscope in the left hand after which cross the inflexible bronchoscope with the laryngoscope in place with the best hand. After the glottis is in view, the inflexible bronchoscope is advanced towards the glottic opening. The bronchoscope is handed through the larynx into the trachea and rotated back to the correct orientation. A inflexible telescope may be handed via the rigid bronchoscope for higher visualization, or alternatively the flexible bronchoscope may be handed by way of the rigid bronchoscope for higher visualization of the distal airway. It could additionally be essential to temporarily hold air flow to keep away from movement of overseas bodies whereas grasping them with forceps. Small foreign bodies less than the diameter of the inflexible scope may be drawn out via the lumen of the scope. Larger overseas our bodies require withdrawal of the rigid scope while holding the international body on the tip of the scope with grasping forceps. On conclusion of the process, the patient could be ventilated using the rigid bronchoscope until such time because the anesthetic agent is cleared and the patient Complications 1. Injury to the tooth Lacerations, contusions, or edema of the pharynx or tongue Damage to the vocal cords or dislocation of the arytenoid Massive hemorrhage that may overwhelm the ability to clear endobronchial blood, inflicting secondary hypoxemia.
Purchase avapro 150 mg free shippingThe narrowest a half of the ethmoid labyrinth is positioned between the anterior portion of the center turbinate and the uncinate and lacrimal processes diabetes type 2 eating guide order avapro on line amex. Care should be taken on this space to avoid injury to the mucosa and subsequent formation of synechia. After confirming the placement of the free edge of the uncinate course of, retrograde dissection is performed approximately one-third of the means in which from the attachment of the uncinate course of to the ethmoidal process of the inferior turbinate. Uncinate window created by retrograde dissection on the left aspect with pediatric back-biting forceps to reveal pure os (arrow). The inferior portion consists of the remaining uncinate connected to the ethmoidal means of the inferior turbinate and the mucosa medially and laterally. Submucosal dissection of the uncinate process on the left facet with a double-ball probe seeker. The portion inferior to the uncinate window then consists of the nasal mucosa, the residual bone of the uncinate course of, which inserts into the inferior turbinate, and the mucosa on the sinus side. Removing the uncinate process on this submucosal trend permits the natural ostium of the maxillary sinus to be enlarged without damage to the entire mucosal circumference of the ostium. Care is taken not to damage any of this mucosa, which may end in a minimum of obstruction and edema with resultant an infection and, at worst, stenosis of the maxillary ostium. Irrigation can be performed via an accessory ostium if current or by way of an inferior meatal puncture. This technique is used for normal instances of recurrent acute sinusitis and chronic maxillary sinusitis (Video 103. In instances during which a maxillary antrostomy is prudent, the verified natural ostium may be enlarged posteriorly into the posterior fontanelle while preserving the maxillary sinus mucosa 270 levels anteriorly across the ostium. Once the decision has been made to create an antrostomy, it should be a large one. A tear-shaped antrostomy may be best for the restoration of regular mucociliary clearance. Care should be taken when dissecting posteriorly as injury to branches of the sphenopalatine artery or the descending palatine nerve can happen. Depending on the pathology of the maxillary sinus, the degree of required access might differ. Studies have demonstrated that small-hole strategies severely restrict the accessibility to the sinus. Similarly in our personal study, we discovered that instruments with increasing curvatures allowed for higher access to the sinus, but no single instrument could reach the whole maxillary sinus wall by way of an endoscopic antrostomy. A maximal maxillary antrostomy allows full view of the sinus element and usually the stalk, which has a variable location within the sinus however is most frequently found connected to the lateral wall of the sinus. The polyp often has a "neck," which can be grasped with a 90-degree ethmoid forceps to remove the majority of the antrochoanal polyp. A commonplace curved 4-mm soft tissue shaver is used to get rid of the rest of the polyp. A commonplace 4-mm delicate tissue shaver can thus be placed with visualization of the sinus with an angled transnasal endoscope, or a 30-degree telescope can be launched through the puncture and a curved instrument positioned transnasally with a minimally invasive approach. In some cases a double-barrel canine fossa puncture is performed to permit both the shaver and scope to be launched, the scope by way of the trocar sleeve and the shaver directly by way of the entrance face of the maxilla. For the shaver, a regular canine fossa puncture is performed above the gingivobuccal sulcus superior to the canine tooth within the palpated fossa. An extended finger on the cheek prevents perforation of the posterior wall of the maxillary sinus after breeching the anterior wall. The nondominant hand may be saved on the orbital rim to forestall the trocar complex from sliding too superiorly on the entrance face of a dense maxilla and damaging the orbit. Once the trocar and sleeve are throughout the sinus, the trocar can be eliminated and a telescope positioned for full publicity. Best outcomes with the shaver occur with removing of each the sleeve and trocar and placement of the device by way of the created surgical tract. A 30-degree scope is good for complete inspection of the maxillary sinus through the canine fossa. No packing or dressings are needed, and extra surgery on the ethmoid sinus is sort of never required. Though more and more much less widespread, external approaches using a Caldwell Luc operation may be employed for antrochoanal polyp (see Chapter 104). Postoperative ache should be minimal and is usually managed with Tylenol or low-dose narcotics. Nasal steroid sprays and different intranasal medications are sometimes started 1 week after surgery or after the completion of systemic steroids if used. There is at present no strong proof to assist the routine use of postoperative antibiotics. Certainly, if an infection is encountered, a tradition ought to be taken, and the patient ought to be positioned on empiric antibiotic therapy. Generally, the affected person is cautioned against nose blowing and weight lifting is limited to lower than 10 kilos postoperatively. For the endoscopic method, nasal saline irrigation usually serves as sufficient postoperative care. Wide postoperative analysis of the surgical site is afforded by the maxillary antrostomy. In circumstances of recurrence, performing a maximal maxillary antrostomy aids in irrigation, medication supply, and postoperative surveillance. In many patients, the dearth of a transparent prognosis and indication for surgical procedure may find yourself in unwarranted and unsuccessful surgery. The patients should be re-evaluated during exacerbation of symptoms so that an accurate analysis could be made. Patients with facial pain within the absence of different signs are hardly ever provided surgery except each other avenue has been undertaken and the affected person understands that no assure may be made. This may be continued infection, recurrence of polyposis, retained secretions, and a residual fungus ball or antrochoanal polyp. Formation of synechia remains the main pitfall, and the use of powered instrumentation has minimized mucosal trauma and thus has averted the vast majority of these issues. Powered instruments permit preservation of most or the complete mucosal ring of the pure ostium. Furthermore, stripping of the mucosal lining creates a positive environment for osteitis and postoperative scarring. Thus, all present endoscopic sinus procedures are predicated on an improved ability to preserve the mucous membrane. Patients may have multiple openings in their posterior fontanelle (accessory ostia).
Order avapro 300 mg with amexHemorrhage: the most common and usually the one complication that leads to rehospitalizations and wish for reoperation 2 diabetes test strips gold avapro 300mg with mastercard. Patient selection: At the time of panendoscopy, previous to definitive surgical procedure, examination of the mobility of the tumor (especially with regard to the carotid artery) must be noted. Additionally, issues with mouth opening ought to be noted right now as a end result of they could preclude the use of the mouth gag/visualization. Poor exposure: Placing the mouth gag in one of the best configuration for exposure of the palate, the tonsil, and about 1 cm of the bottom of the tongue. This includes pulling the oral tongue toward the contralateral facet and utilizing a tongue blade long enough to expose the bottom of the tongue. Failure to do this can lead to the necessity for repositioning halfway by way of the case or growing the risk of optimistic margins. Transoral robotic surgical procedure: a multicenter examine to assess feasibility, safety, and surgical margins. Influence of condition of surgical margins on native recurrence and disease-specific survival in oral and oropharyngeal cancer. Influence of close resection margins on local recurrence and disease-specific survival in oral and oropharyngeal carcinoma. Do constructive resection margins after ablative surgery for head and neck cancer adversely affect prognosis A research of 352 sufferers with recurrent carcinoma following radiotherapy treated by salvage surgery. The surgical assistant offers retraction of the endotracheal tube to the contralateral facet as needed in the course of the operation. The bedside assistant plays a key position in offering countertraction that can facilitate the secure and efficient dissection and en bloc resection. For cancers that invade the bottom of the tongue, the lingual artery is usually encountered while performing resection of the lateral base of the tongue. It lies lateral to the intrinsic muscular tissues of the tongue and medial to the hyoglossus muscle, coursing superior to the hyoid bone. Should the surgeon inadvertently enter the lingual artery, control is aided by suctioning from the bedside assistant as properly as exterior strain being utilized to the neck by the assistant above the ipsilateral greater cornu of the hyoid. It is important to embrace some palate and constrictor musculature within the horizontal mattress suturing or the mucosal approximation will probably tear and the lateral tissue gap might reopen. In cases the place there stays a lateral tissue hole and communication with the nasopharynx after the pharyngoplasty, the recommendation is to use a pedicled pad of buccal adipose tissue for ultimate closure. The boundaries of the usual radical tonsillectomy embody all of the following except which possibility Transoral robotic surgical procedure alone for oropharyngeal cancer: an evaluation of local control. Selective neck dissection and deintensified postoperative radiation and chemotherapy for oropharyngeal cancer: a subset analysis of the University of Pennsylvania transoral robotic surgery trial. In addition, wound healing and vascularity are compromised, and these sufferers could take many months to heal by secondary intention. Patients with severe cardiac or pulmonary illness could not be ready to tolerate major surgery and postoperative rehabilitation. Likewise, sufferers with identified hereditary coagulopathies are predisposed to postoperative bleeding. Anticoagulants including Coumadin, Plavix, and aspirin should be discontinued preoperatively and ideally for at least 2 weeks after surgery. It should be recognized that the use of dietary supplements corresponding to Ginkgo biloba, fish oil, and vitamin E might pose an elevated danger for postoperative bleeding. Historically, most surgical resections in this region have involved open approaches, corresponding to suprahyoid pharyngotomy or lip-split mandibulotomy. Given the morbidity of those approaches, organ preservation protocols initially developed for cancer of the larynx have been tailored to the oropharynx. Long-term treatment-related sequelae from chemoradiation, significantly pertaining to swallowing dysfunction, have turn out to be increasingly acknowledged over time. Accurate staging and assessment of histologic risk factors can thus be definitively decided, rather than counting on imaging alone. With comprehensive pathologic staging, patients can then be danger stratified to receive applicable adjuvant therapy, if indicated. Two of essentially the most difficult elements of the procedure are acceptable affected person choice and maximizing exposure during the resection. Appropriate docking and setup of the surgical robot, together with proper choice and then positioning of the retractor, are the keys to optimizing exposure. The dorsal lingual department of the lingual artery is usually encountered in the lateral side of the resection and have to be managed appropriately to prevent postoperative hemorrhage. Appropriate suctioning, traction, and countertraction greatly facilitate surgical access and visualization. Evaluation of the base of the tongue is performed by each direct examination and versatile laryngoscopy. The glossotonsillar sulcus, vallecula, and epiglottis are assessed for grossly visible cancer. Palpation, if tolerated, is important to estimate depth of invasion into the tongue. Care is taken to observe the variety of lymph node metastases and whether or not obvious contralateral metastasis is current. Oral aperture together with mandibular dimensions and positioning, tongue measurement and shape, and dentition are evaluated to determine if sufficient transoral exposure is possible. Elicitation of symptoms together with dysphagia, otalgia, odynophagia, aspiration, weight loss, and dyspnea. In addition, these symptoms might recommend deep submucosal infiltration of the most cancers that is in all probability not clinically apparent. Obvious involvement of deep parapharyngeal area constructions, extrinsic tongue musculature, and the hyoid bone might preclude transoral resection. Airway hearth is a probably life-threatening complication of oropharyngeal surgery. Fraction of impressed oxygen ought to be kept lower than 30%, and an acceptable sized endotracheal tube must be positioned to forestall leakage around the cuff. All patients require full neuromuscular paralysis to facilitate placement of the retractor and allow for maximum publicity. The working table is rotated one hundred eighty degrees and lowered to the maximum extent to accommodate placement of the robotic arms. The surgical robot (Intuitive Surgical da Vinci Si) is docked to the right and positioned at a 30-degree angle to the operating table, making sure that the robotic foot is touching the bottom of the table. The robot is positioned in order that the pivot level of the camera arm is approximately at the stage of the oral commissure. The pivot point of the central scope arm is rotated inwards and then lifted as a lot as its most peak. At this point, the scope arm is moved down till the digital camera touches the posterior pharyngeal wall.
References - Hart SC, Nguyen-Tu BL, Hould F: Restoration of myolelectrical propagation across a jejunal transection using microsurgical anastomosis. J Gastrointest Surg 3:524, 1999.
- Purohit RS, Wu DS, Shinohara K, et al: A prospective comparison of 3 diagnostic methods to evaluate ejaculatory duct obstruction, J Urol 171:232n235, discussion 235n236, 2004.
- Ryu ES, Kim MJ, Shin HS, et al. Uric acid- induced phenotypic transition of renal tubular cells as a novel mechanism of chronic kidney disease. Am J Physiol Renal Physiol 2013; 304(5):F471-80.
- Rovina N, Dima E, Gerassimou C, et al. Interleukin-18 in induced sputum: association with lung function in chronic obstructive pulmonary disease. Respir Med 2009;103:1056-62.
- Hashimoto K, Mayahara H, Takashima A, et al. Palliative radiation therapy for hemorrhage of unresectable gastric cancer: a single institute experience. J Cancer Res Clin Oncol 2009;135(8):1117-1123.
- Raitt MH, Connor WE, Morris C, et al: Fish oil supplementation and risk of ventricular tachycardia and ventricular fibrillation in patients with implantable defibrillators. A randomized controlled trial. JAMA 2005;593:2884-2891.
|


