|
Kamran Tabaddor, MD - Clinical Professor and Chairman
- Department of Surgery
- Our Lady of Mercy Medical Center
- Clinical Professor of Neurosurgery
- Albert Einstein College of Medicine
- Bronx, New York
Crestor dosages: 20 mg, 10 mg, 5 mg
Crestor packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

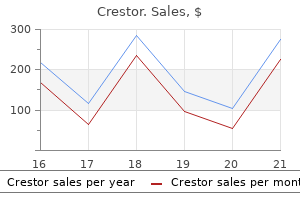
Buy crestor australiaSecond heart sound (S2): outcomes from the closing of the aortic and pulmonary valves cholesterol medications and alzheimer's cheap crestor 5mg without a prescription. Necrosis normally happens approximately 20 to half-hour after coronary artery occlusion. Anterior infarct Anterolateral infarct Occlusion of proximal left anterior descending a. Infarct Infarct True posterior infarct Diaphragmatic or inferior infarct Occlusion of distal circumflex a. Sounds are finest heard by auscultating the realm the place turbulent blood flow radiates. Major problems embrace stenosis (narrowing) or insufficiency (compromised valve operate, typically resulting in regurgitation). Minimally vasoconstricts the coronary resistance vessels (via alpha adrenoceptors). In the posterior mediastinum, a bilateral thoracic sympathetic chain of ganglia (sympathetic trunk) passes across the neck of the upper thoracic ribs and, because it proceeds inferiorly, aligns itself closer to the lateral our bodies of the decrease thoracic vertebrae. Each of the eleven or 12 pairs of ganglia (number varies) is related to the anterior ramus of the corresponding spinal nerve by a white ramus communicans (the white ramus conveys preganglionic sympathetic fibers from the spinal nerve). A gray ramus communicans then conveys postganglionic sympathetic fibers again into the spinal nerve and its anterior or posterior rami (see Chapter 1, Nervous System). Additionally, the upper thoracic sympathetic trunk conveys small thoracic cardiac branches (postganglionic sympathetic fibers from the higher thoracic ganglia, T1-T4 or T5) to the cardiac plexus, where they mix with preganglionic parasympathetic fibers from the vagus nerve. Sympathetic ibers arise from the higher thoracic cord levels (intermediolateral cell column of T1-T4/T5) and enter the sympathetic trunk. Cervicothoracic (stellate) ganglion Ansa subclavia Superior cervical ganglion Left vagus n. Thoracic (sympathetic) cardiac branches Cardiac plexus (deep) Thoracic (sympathetic) cardiac branches Thoracic cardiac branches of vagus n. Implantable cardiac pacemaker (dual-chamber cardiac pacing) the endocardial leads are usually introduced by way of the subclavian or the brachiocephalic vein (left or proper side), then positioned and tested. A pocket for the heartbeat generator is usually made below the midclavicle adjacent to the venous entry for the pacing leads. The incision is parallel to the inferior clavicular border, roughly 1 inch under it. The pulse generator is positioned either into the deep subcutaneous tissue just above the prepectoralis fascia or into the submuscular area of the pectoralis major. Coracoid course of Atrial and ventricular leads 130 Chapter 3 Thorax Clinical Focus 3-20 Cardiac Defibrillators An implantable cardioverter defibrillator is used for survivors of sudden cardiac demise, patients with sustained ventricular tachycardia (a dysrhythmia originating from a ventricular focus with a heart price usually higher than one hundred twenty beats/min), these at excessive risk for creating ventricular arrhythmias (ischemic dilated cardiomyopathy), and other indications. In addition to sensing arrhythmias and providing defibrillation to cease them, the gadget can perform as a pacemaker for postdefibrillation bradycardia or atrioventricular dissociation. The distal coil is in the proper ventricle, and the proximal one is within the superior vena cava/right atrial position. Lesser splanchnic nerve: preganglionic fibers normally arise from the T10-T11 spinal wire ranges. Least splanchnic nerve: preganglionic fibers normally come up from the T12 spinal wire degree. Visceral aferents for ache or ischemia from the center are conveyed back to the higher thoracic spinal twine, often ranges T1-T4 or T5, through the sympathetic fiber pathways (see Clinical Focus 3-13). Aortic arch and its three arterial branches (brachiocephalic trunk, left widespread carotid artery, and left subclavian artery) and pulmonary trunk. Cardiac plexus Anterior pulmonary plexus Sympathetic trunk Thoracic aortic plexus Esophageal plexus Greater thoracic splanchnic n. Posterior mediastinum: the area posterior to the center and anterior to the our bodies of the T5-T12 vertebrae; accommodates the esophagus and its nerve plexus, thoracic aorta, azygos system of veins, sympathetic trunks and thoracic splanchnic nerves, lymphatics, and thoracic duct. Esophagus and Thoracic Aorta he esophagus extends from the pharynx (throat) to the stomach and enters the thorax posterior to the trachea. As it descends, the esophagus steadily slopes to the left of the median airplane, mendacity anterior to the thoracic aorta. Bronchial arteries: arteries that offer blood to the lungs; usually one artery to the proper lung and two to the left lung, however variable in number. Mediastinal arteries: small branches that offer the lymph nodes, nerves, and connective tissue of the posterior mediastinum. Superior phrenic arteries: small arteries to the superior surface of the respiratory diaphragm; anastomose with the musculophrenic and pericardiacophrenic arteries (which come up from the interior thoracic artery). Subcostal arteries: paired arteries that lie under the inferior margin of the final rib; anastomose with superior epigastric, lower intercostal, and lumbar arteries. A small left superior intercostal vein (a tributary of the left brachiocephalic vein) can also join with the hemiazygos vein. As it approaches the diaphragm, the aorta shifts nearer to the midline of the decrease thoracic vertebrae. Collateral branch Dorsal ramus Lateral cutaneous branch Medial mammary department Anterior intercostal a. While most of those veins are valveless, recent proof suggests that some valves do exist in variable numbers in a few of these veins. An ascending lumbar vein from the upper stomach cavity collects venous blood segmentally and often from the left renal vein; it is a vital connection between these abdominal caval veins and the azygos system within the thorax. A variety of mediastinal veins exist in the posterior mediastinum and drain the diaphragm, pericardium, esophagus, and major bronchi. Ascending lumbar vein (left) Posterior intercostal veins (left 8�12th) Esophageal veins Mediastinal veins Superior phrenic veins (left) 2. Inferior vena cava Ascending lumbar vein (right) Posterior intercostal veins (right 5�11th) Esophageal veins Mediastinal veins Pericardial veins Bronchial veins (right) Right superior intercostal vein 3. About midway within the thorax, the hemiazygos vein crosses the midline and drains into the azygos vein (3), though the hemiazygos usually maintains its reference to the accessory hemiazygos vein as well. Veins tend to connect with one another where potential, and many connections are small, variable, and not readily recognizable. Flow within the azygos system of veins is pressure dependent; as a result of the veins are basically valveless, the circulate can go in either direction. As with different regional veins, the variety of veins of the azygos system could be variable. Thoracic Lymphatics he thoracic lymphatic duct begins in the abdomen at the cisterna chyli (found between the stomach aorta and the best crus of the diaphragm), ascends by way of the posterior mediastinum posterior to the esophagus, crosses to the left of the median plane at roughly the T5-T6 vertebral degree, and empties into the venous system on the junction of the left internal jugular and left subclavian veins. Lymph from the left hemithorax and left lung typically drains into tributaries that vacant into the thoracic duct. Lymph 138 Inferior deep cervical (internal jugular) nodes Thoracic duct Paratracheal nodes Superior and inferior tracheobronchial nodes Posterior mediastinal nodes Intercostal nodes Posterior parietal nodes Chapter 3 Thorax mesoderm varieties the stroma of every lung. By 6 months of gestation, the alveoli are mature enough for fuel exchange, however the production of surfactant, which reduces surface rigidity and helps prevent alveolar collapse, may not be suicient to support respiration.
Syndromes - For males, place the entire penis in the bag and attach the adhesive to the skin.
- Blisters
- Have you had eye surgery or injuries?
- Xanthelasma -- raised yellow patches on your eyelids that can happen with age. These are harmless, although they are sometimes a sign of high cholesterol.
- Saliva
- Muscle weakness, stiffness, or soreness
- Starts to share
- Time it was swallowed or touched the skin
- Poor blood supply to the legs
- CT scan of the head
Purchase crestor in indiaOpening of auditory tube Nasopharynx Uvula Location of tonsils Epiglottis Pharynx Oesophagus Larynx Trachea Nasal cavity Nostril Hard palate Oral cavity Tongue � Viruses then invade the mucosal floor cholesterol levels when not fasting order crestor from india, producing an inflammatory response. Clinical features Symptoms � the main signs tend to be mild and non-specific, and embody: � nasal obstruction and sneezing � nasal discharge (often clear) � a sore throat � a headache. This is extra pronounced in infants and may be the presenting symptom in this group. Signs � It should be famous that the heterogeneity of this condition implies that signs may be current or absent, and found in numerous mixtures. Lift the tip of the nostril gently and, using the most important attachment of the auroscope, gently place the tip contained in the naris. If this upsets the patient and they begin crying, be savvy: use this as an opportunity to visualize the pharynx. Where this proves ineffective, alternate administration of both medications and ask the dad and mom to start a therapy diary. Epidemiology and threat components � Epiglottitis accounts for about 600 admissions in England yearly. Clinical features Symptoms (The four Ds) � Early: Drooling and Dysphagia/Odynophagia � Late: Dysphonia and Dyspnoea � Rapidly progressing sore throat (hours) ought to immediate consideration of this analysis. These sufferers are vulnerable to reflex laryngospasm and subsequent acute airway obstruction. Whilst typically gentle with no long-term sequelae, it could present as life-threatening airway compromise. Pathophysiology the most common causal organism is parainfluenza virus (~80%), which is usually transmitted by respiratory droplets or via contamination of hands. Parainfluenza virus impacts the larynx and trachea (� the bronchi) Swelling limits airflow by way of the higher respiratory tract Tissue oedema and swelling Epidemiology and danger factors � Affects kids between the ages of 6 months and 3 years � Most prevalent in late autumn � There is a slight male preponderance of 1. In these patients, the next therapy is suggested: � Give oxygen to preserve saturations between 94 and 98%. It is predicated on the medical features including: (i) inspiratory stridor (ii) intercostal muscle recession (iii) lowered air entry (iv) presence of cyanosis and (v) altered consciousness. Pathophysiology � An inflammatory cascade is triggered, leading to elevated vascular permeability, with: � subsequent loss of plasma into the alveoli, leading to lowered airspace and consolidation � airway narrowing because of tissue oedema and increased production of mucus. Although classically productive of purulent sputum, this is generally absent in younger kids. Ix � Investigations are primarily required to determine the causal organism and subsequently enable focused therapy. Pathophysiology � Spread through respiratory droplets, Bordetella pertussis is a extremely contagious organism. This exudate can compromise the small airways, predisposing to atelectasis and pneumonia. Note, the kid will usually flip red in the face and flail their limbs throughout episodes. The clinical picture seen is just like that of adult illness; nonetheless, administration is completely different and paediatric pointers must be used. Pathophysiology � Asthma is a persistent inflammatory situation affecting the airways, characterised by paroxysmal, reversible airway narrowing and airway hyper-responsiveness. Trigger issue Airway in ammation Hypersecretion of mucus Airway muscle constriction Swelling bronchial membranes Narrow respiration passages Airway wall Thickened airway wall Mucus Muscle Airway cross-section Muscle. Before 5 years, definitive diagnosis is difficult and due to this fact often deliberately delayed. Ex � Acutely, the kid is in obvious respiratory misery and has widespread polyphonic wheeze. To promote movement of chloride (Cl-) ions down their concentration gradient: � They are found on the apical membranes of epithelial cell (in the lungs, pancreatic ducts, gastrointestinal tract, biliary tree and vas deferens) and so, in most cases, the Cl- gradient drives Cl- out of cells and into the secretions. To inhibit the impact of the epithelial sodium channel, an ion transporter which strikes Na+ (and subsequently water, which follows it) from the secretions and into the cells. This promotes bacterial colonization leading to recurrent infection and in ammation. Chronically, this can result in biliary cirrhosis and impaired absorption of the fat-soluble nutritional vitamins. This impairs supply of pancreatic secretions to the gastrointestinal tract (malabsorption) and causes stagnation inside the pancreas (autodigestion pancreatic insu ciency and diabetes mellitus (50% of adults)). Secretions are reduced and thickened in addition to the low biliary and pancreatic secretions. This leads to thickening of the bowel contents, which can lead to: � Obstruction due to constipation (meconium ileus in newborns) � Intussusception � In ammatory strictures or adhesions There is a congenital absence of the vas deferens, rather than this being sequelae of thickened secretions. High concentrations of Cl� in the sweat, as a end result of impaired re-absorption down its focus gradient. The most typical options for every age group are indicated as follows: infants (*), early childhood and late childhood/adolescence in Table 8. Management � the administration of those children is advanced and requires tertiary referral and involvement of the multidisciplinary team, with the overall aims being to slow lung illness progression and guarantee sufficient diet. As the kid turns into more assured and better capable of coordinate chewing and swallowing, firmer meals may be introduced. Children sometimes current with posseting or vomiting, with out any other symptoms. On examination, the kid is properly, gaining weight normally, nicely hydrated and has no findings on examination. In the developing world, it accounts for ~20% of childhood deaths beneath 5 years old, thus illustrating the importance of excellent management of these sufferers. Pathophysiology � Viral causes account for ~60% of instances and are answerable for winter epidemics, with rotavirus (55%) and norovirus the main brokers. Infection causes irritation and injury to villous border, decreasing absorptive capacity Dehydration and loss of electrolytes If left, electrolyte disturbance and hypovolaemic shock with end-organ failure Epidemiology and threat components Clinical options Symptoms � Usually begins with non-specific signs corresponding to low grade fever, followed by vomiting and/or diarrhoea. Investigation and analysis Hx � Regurgitation/vomiting, classically post-prandially. It typically begins within the first few weeks of life and resolves spontaneously by 4�5 months of age. Diagnosis and investigations Hx � Paroxysms of crying, typically worse in the afternoons and evenings. Pathophysiology and threat factors Functional constipation will usually start with a low-fibre, low-fluid food regimen leading to hardening of the stool. Ix � Usually a clinical analysis; nevertheless, if ongoing, contemplate: � blood tests for coeliac disease and hypothyroidism � plain belly X-ray or ultrasound � rectal biopsy (if Hirschsprung illness is suspected). Clinical pharmacology: Commonly used laxatives in kids Class Macrogols Name Polyethylene glycol 3350 (Movicol) Lactulose Mechanism of motion Induces effect by retaining water in the stool.
Generic crestor 10mg otcPatients rapidly turn into delirious; and applicable investigation and therapy ought to proceed expeditiously quitting cholesterol medication safe crestor 5mg, as the situation is associated with poor outcomes. Features include: � Hyperactive state: arousal, restlessness, agitation � Hypoactive state: drowsy, quiet � the aged, those with intercurrent sickness and medical/surgical inpatients are at higher risk for delirium � Diminished cognition, visual or auditory hallucinations E Table 5. P In some circumstances, discovering and stopping a medication-provoked delirium may be tough. When confronted with this possibility, contemplate stopping non-essential medicines so as to assess for indicators of improvement. These drugs can always be re-titrated and re-introduced at a later date when the affected person is secure. The most typical aetiology for dementia is a neurodegenerative process, with vascular aetiologies making up about 20%. There are additionally rarer, doubtlessly treatable causes, such as thyroid problems, nutritional Vascular neurocognitive disorder is a more recent time period used to describe a spread of pathology from mild cognitive impairment to pure vascular dementia. In apply, there may usually be a combined aetiology but evidence of cerebrovascular disease (either on imaging or clinically), in the context of cognitive impairment, is said to confer the prognosis. Lifestyle modification related to threat factors should be pursued as a lot as possible, with aggressive lipid-lowering remedy instituted if necessary. It is a progressive, neurodegenerative condition, characterised by accumulation of neuronal amyloid plaques (as well as phosphorylated tau protein), which form neurofibrillary tangles. Management Epidemiology: � Largely affects older individuals, above the age of 65 � More common in ladies � Thought to have an elevated risk when cardiometabolic danger components are also implicated. Distinguishing between the two might assist in remedy, as acetylcholinesterase inhibitors may improve dementia with Lewy our bodies, while drugs used to treat parkinsonism could yield extra profit in a primarily Parkinsonian diagnosis. There are numerous subtypes of the disease, and classification depends on presenting options. What makes blood unique is its fluidity, which allows it to be circulated all through the physique. Bu y coat: � White blood cells, platelets Haematocrit: � Red blood cells Normal blood: 37�47% haematocrit 42�52% haematocrit Haematopoiesis Haematopoiesis refers to the production of blood cells. This primarily happens in the bone marrow, but extramedullary haematopoiesis can also happen in the liver and spleen (in the case of bone marrow failure). These cells have the distinctive capacity to differentiate into two major hierarchies of stem cell lineages, namely. After division, some cells stay stem cells Multipotent haematopoietic stem cell (haemocytoplast) the remaining cell goes down one of two paths relying on the chemical alerts acquired Myeloid stem cell Lymphoid stem cell Megakaryoblast Proerythroblast Myeloblast Monoblast Lymphoblast Reticulocyte Natural killer cell (large granular lymphocyte) Megakaryocyte Erythrocyte Basophil Neutrophil Eosinophil Monocyte T lymphocyte Platelets B lymphocyte Small lymphocyte. This involves a posh interaction of techniques between the vessel wall, platelets, coagulation components and fibrinolytic enzymes. Disruption of these mechanisms gives rise to bleeding and thrombotic (clotting) disorders. Coagulation � the coagulation cascade is historically divided into extrinsic and intrinsic pathways; each cascades ultimately converge at the activation of issue X that leads to a ultimate widespread pathway. They are incessantly used in the remedy and prophylaxis of venous thromboembolisms and prevention of stroke in atrial fibrillation. The Rh system refers to the presence or absence of the Rh antigens on the erythrocyte surface membrane. P Fondaparinux Xa 14 15 Apixaban, rivaroxaban Dabigatran Problems related to RhD status occur most commonly throughout pregnancy. These are usually delicate reactions, however you will want to pay consideration to severe problems which will occur. The conditioning process often requires high-dose chemotherapy (with or with out radiotherapy), which has the twin function of destroying malignant cells and inducing short-term immunosuppression. This may occur in up to one-third of patients and may be historically categorized as acute (within the first one hundred days) or continual (100 days from transplant). Looking at the morphology of blood cells also presents a clue to the kind of anaemia, i. The commonest causes of a microcytic anaemia are iron-deficiency anaemia and thalassaemia. Common causes of macrocytic anaemias embody excess alcohol, folate and/or vitamin B12 deficiency (from pernicious anaemia or insufficient dietary intake), varied drugs and myelodysplasia. Patients with anaemia may suffer from fatigue, dyspnoea and complications, but different systemic features (particularly weight loss, night time sweats and fevers) ought to prompt a more thorough evaluation, and an try to elicit an underlying cause. A careful evaluation is warranted, as patients with this syndrome are additionally at greater risk of growing oesophageal carcinomas. The illness course of is typically associated with gene deletions and level mutations respectively, resulting in improper synthesis of adult haemoglobin, which consists of two alpha globin chains and two beta globin chains. These may be variations of alpha, beta, gamma or delta globin chains, producing various types of haemoglobin. Some of the extra common variants embody: � Haemoglobin A (HbA): two alpha chains, two beta chains (96�98% of Hb) � Haemoglobin A2 (HbA2): two alpha chains, two delta chains (2�3% of Hb) � Haemoglobin F (HbF): two alpha chains, two gamma chains (1�2% of Hb), primarily produced by the foetus Management Stepwise administration of iron-deficiency anaemia 1 Oral iron substitute is the first-line therapy � Oral ferrous sulphate/fumarate � May take up to 2 months for haemoglobin ranges to normalise the effect of these mutations on signs might vary, depending on the sort and extent of involvement, and thalassaemia might at occasions be categorised as minor, main or intermedia. Beta thalassaemia is extra prone to affect people of Mediterranean origin, while alpha thalassaemia is more more likely to have an effect on Asians. These produce three clinically significant types of beta thalassaemia � beta thalassaemia minor, beta thalassaemia intermedia and beta thalassaemia main (see Table 6. This excess iron is deposited in numerous organs and should cause fibrosis, organ failure and endocrinopathies if endocrine organs are affected. Oral iron chelators (such as deferasirox and deferiprone) are additionally obtainable, and the usage of these agents is proving extra popular due to their route of administration. Outcome/management Usually asymptomatic Patients require lifelong blood transfusions and iron chelation In these sufferers, the need for transfusions is decided by the severity of their illness Hypochromic, microcytic anaemia; elevated levels of HbA2 Severe anaemia begins to develop early on in infancy, when HbF levels start to fall; presents with jaundice, sleepiness and failure to thrive; may have bony abnormalities; elevated levels of HbF and HbA2 Patients sometimes current with anaemia, but could vary in presentation with regard to jaundice, bony abnormalities and other symptoms 6. The resultant cells (megaloblasts) are bigger in size, with disproportionately enlarged nuclei. This disease is clinically indistinguishable from other types of anaemia, however iron studies will show excessive iron ranges. A definitive diagnosis is made on demonstrating ringed sideroblasts on bone marrow research. Pyridoxine (vitamin B6) may be useful in treating congenital types of this disease. As discussed in Chapter 3, dietary vitamin B12 binds to intrinsic factor produced by gastric parietal cells and this complicated is subsequently absorbed in the terminal ileum. Hence, the causes of vitamin B12 deficiency can be divided, based on these factors: � Insufficient dietary vitamin B12 intake �. It is present as polyglutamates which are subsequently transformed into the monoglutamate form in the proximal small bowel (mainly the jejunum) and actively absorbed into the plasma. Megaloblastic anaemia this type of anaemia is attributable to deficiencies in either vitamin B12 or folic acid. The biochemical mechanism of folate and vitamin B12 in megaloblastic anaemia is shown in. Pernicious anaemia Pernicious anaemia is an autoimmune situation characterised by atrophic gastritis and destruction of parietal cells. It is commonly discovered within the aged inhabitants, with a mean age of onset of 60.

Discount 20mg crestor visaStudies counsel that the smaller 37-Fr Combitube can be used safely in patients as a lot as cholesterol levels mayo clinic purchase 5mg crestor with amex roughly 6 ft tall. To insert the Combitube, maintain the gadget within the dominant hand and gently advance it caudally into the pharynx whereas grasping the tongue and jaw between the thumb and index finger of the nondominant hand. A, Approximately 95% of placements are esophageal, so begin ventilation via the longer (blue) airway tube. When the distal tip is within the esophagus, air flow occurs via the vent holes between the distal and proximal cuffs (white arrows). It is crucial to acknowledge this quickly, and use the brief (white) tube for ventilations. The giant pharyngeal balloon serves to securely seat the Combitube in the oropharynx and creates a closed system in the case of esophageal placement. Because approximately 95% of placements are esophageal, begin ventilation through the longer (blue) airway tube. Alternatively, use a Wee-type aspirator device on the shorter (clear) lumen to verify that the tip is in the esophagus before ventilation via the longer (blue) lumen. Easy aspiration with the Wee-type system indicates tracheal positioning of the tube and requires changing the ventilation to the shorter (clear) tracheal lumen. Use a extra caudal, longitudinal path of insertion versus an anteroposterior direction of insertion. The Combitube should also be maintained in the true midline position throughout insertion to avoid blind pockets within the supraglottic area, which may stop passage of the tube. There are many methods and gadgets that can be utilized to manage emergency airways. In tough situations, providers will in all probability have the best success when fundamental expertise are carried out excellently. Complications Inappropriate balloon inflation and incorrect Combitube placement can result in air leaks throughout air flow. Combes X, Jabre P, Margenet A, et al: Unanticipated difficult airway administration in the prehospital emergency setting: prospective validation of an algorithm. Meier S, Geiduschek J, Paganoni R, et al: the impact of chin raise, jaw thrust, and steady optimistic airway pressure on the scale of the glottic opening and on stridor score in anesthetized, spontaneously respiratory youngsters. Guildner C: Resuscitation-opening the airway: a comparative study of strategies for opening an airway obstructed by the tongue. In Calder I, Pearce A, editors: Core subjects in airway management, Cambridge, 2005, Cambridge University Press, p forty three. Morikawa S, Safar P, Decarlo J: Influence of the head-jaw place upon higher airway patency. Ayuse T, Inazawa T, Kurata S, et al: Mouth-opening increases upper-airway collapsibility without changing resistance during midazolam sedation. Kobayashi M, Ayuse T, Hoshino y, et al: Effect of head elevation on passive higher airway collapsibility in normal topics underneath propofol anesthesia. Isono S, Tanaka A, Tagaito y, et al: Influences of head positions and chew opening on collapsibility of the passive pharynx. Langhelle A, Sunde K, Wik L, et al: Airway stress with chest compressions versus Heimlich manoeuvre in recently lifeless adults with full airway obstruction. Gruber P, Kwiatkowski T, Silverman R, et al: Time to equilibration of oxygen saturation using pulse oximetry. Global Initiative for Chronic Obstructive Lung Disease: Global technique for the prognosis, management, and prevention of chronic obstructive pulmonary illness, 2011. Dorges V, Wenzel V, Knacke P, et al: Comparison of various airway administration methods to ventilate apneic, nonpreoxygenated patients. Dorges V, Ocker H, Hagelberg S, et al: Optimisation of tidal volumes given with self-inflatable baggage without further oxygen. Reardon R, Ward C, Hart D: Assessment of face-mask air flow utilizing an airway mannequin. Ikeda A, Isono S, Sato y, et al: Effects of muscle relaxants on mask air flow in anesthetized individuals with regular higher airway anatomy. Harboe M: Lactic acid content in human venous blood during hypoxia at high altitude. Slessarev M, Somogyi R, Preiss D, et al: Efficiency of oxygen administration: sequential gas delivery versus "flow into a cone" methods. Wexler H, Aberman A, Scott A, et al: Measurement of intratracheal oxygen concentrations throughout face mask administration of oxygen: a modification for improved management. In Walls R, Murphy M, Michael F, editors: Manual of emergency airway management, ed 4, Philadelphia, 2012, Wolters Kluwer/Lippincott Williams & Wilkins Heath. Chanques G, Riboulet F, Molinari N, et al: Comparison of three high circulate oxygen remedy supply units: a scientific physiological cross-over study. Tiruvoipati R, Lewis D, Haji K, et al: High-flow nasal oxygen vs high-flow face masks: a randomized crossover trial in extubated patients. Saghaei M, Masoodifar M: the pressor response and airway effects of cricoid strain during induction of basic anesthesia. Asai T, Barclay K, McBeth C, et al: Cricoid stress utilized after placement of the laryngeal mask prevents gastric insufflation but inhibits air flow. Brimacombe J: Laryngeal mask anesthesia: principles and apply, Philadelphia, 2005, Saunders. Frerk C, Mitchell V, McNarry A, et al: Difficult Airway Society 2015 tips for management of unanticipated difficult intubation in adults. Burgoyne L, Cyna A: Laryngeal masks vs intubating laryngeal mask: insertion and air flow by inexperienced resuscitators. Combes X, Le Roux B, Suen P, et al: Unanticipated difficult airway in anesthetized sufferers: prospective validation of a management algorithm. Combes X, Sauvat S, Leroux B: Intubating laryngeal mask airway in morbidly obese and lean sufferers: a comparative research. Asai T, Neil J, Stacey M: Ease of placement of the laryngeal masks throughout handbook in-line neck stabilization. Komatsu R, Nagata O, Kamata K, et al: Comparison of the intubating laryngeal masks airway and laryngeal tube placement throughout guide in-line stabilisation of the neck. Ali A, Canturk S, Turkmen A, et al: Comparison of the laryngeal mask airway Supreme and laryngeal mask airway Classic in adults. Eschertzhuber S, Brimacombe J, Hohlrieder M, et al: the laryngeal masks airway Supreme-a single use laryngeal masks airway with an oesophageal vent. A randomised, cross-over research with the laryngeal masks airway ProSeal in paralysed, anaesthetised patients. Guidelines 2000 for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Part 6: advanced cardiovascular life support: section three: adjuncts for oxygenation, air flow and airway management.
5 mg crestor for saleDrugs and toxins Acute myeloid leukaemia Definition: a malignant disorder of the bone marrow that includes irregular clonal proliferation of cells of the myeloid lineage how do cholesterol lowering foods work cheap crestor 10 mg without prescription. The death (lysis) of irregular cells releases excessive mobile materials into the bloodstream. This often ends in hyperuricaemia, hyperkalaemia, hyperphosphataemia and hypocalcaemia, followed by acute renal failure. A frequent complication of this is differentiation syndrome, which patients should be monitored for. Chronic phase (3�5 years, up to 8) Accelerated section (months) Blastic section (acute leukaemia transformation). Epidemiology: � Most common leukaemia within the West, accounting for 30% of all cases � Annual incidence of 4 per a hundred,000 � Male preponderance of 2:1 and has a median age of onset of 70. These classification methods goal to guide treatment and provide disease prognostic indicators. It has been hypothesised that viral proteins set off abnormal B cells to undergo uncontrolled proliferation and evade apoptosis. However, Cotswold modification of the traditional system is now extra common and is extensively utilized in medical apply (see Table 6. It will increase the elimination of B cells, promoting the development of wholesome B-cell colonies. This makes it particularly efficient in lymphoproliferative issues, involving the B-cell lineage. Chemotherapy and rituximab have been proven to be efficient in inducing remission in up to 50% of sufferers and could additionally be used if clinically acceptable. In simple cryoglobulinaemia (type 1), monoclonal IgM are produced by malignant B cells. The disease is characterised by monoclonal antibody manufacturing and bone marrow infiltration by plasma cells. Hepatitis C infection has been identified as the primary cause in most cases of blended cryoglobulinaemia. Patients are asymptomatic, and analysis is usually made incidentally on biochemical testing. Clinical features: E 80% of patients current with lethargy secondary to anaemia and bony pain, most commonly again ache (secondary to bony lesions). This is normally achieved by weekly venesections, long-term aspirin or hydroxycarbamide (in higher-risk patients). Treatment includes hydroxycarbamide or anagrelide (megakaryocyte maturation inhibitor) to scale back platelet levels, and long-term aspirin. Genetic mutations, mostly V617F, up-regulate the sensitivity in the course of haematopoietic growth factors similar to erythropoietin and thrombopoietin. They can happen primarily (usually because of cytogenetic abnormalities) or secondary to previous chemo-/radiotherapy (10%). The prevalence of those situations has steadily risen and has appreciable impression on the global burden of illness. Hormone-dependent nature of breast most cancers � role of endogenous and exogenous oestrogen in stimulation of mammary tumours. Aetiology/pathophysiology: � Hereditary: genetics (inherited mutations) accounts for less than 2�5% of all breast cancers. Further investigations are warranted if outcomes are inconsistent with the clinical presentation. In younger women, ultrasound is a better modality for evaluating breast plenty because of breast tissue density. P Mammography features suspicious for malignancy embrace irregular spiculated mass, clustered micro-calcifications, linear branching calcifications. Types embrace dysgerminoma (most common), endodermal sinus (yolk sac), teratoma, choriocarcinoma, sarcomas. Krukenberg tumours are bilateral ovarian lots from metastatic mucin-secreting gastrointestinal cancers. Adverse results of radical therapy and administration: P the Gleason score is derived from the sum of the 2 most distinguished tissue varieties on biopsy. Grade 1 signifies essentially the most properly architecturally differentiated tumour, whereas grade 5 signifies probably the most poorly differentiated. Brachytherapy is the transperineal implantation of radioactive seeds instantly into the prostate. Epidemiology: � 1% of all male cancer diagnoses � Peak incidence in males aged 20�40 years � More widespread in white males Table 6. In the course of incurable illness, palliative care extends from prognosis to transition from healing to palliative intent, to ongoing deterioration, terminal stage and bereavement. The palliative care position is influenced by factors such as cultural perceptions of demise and dying, need for treatment, age of the affected person and their familial responsibilities. Opioids are analgesia of choice, spasmolytics corresponding to hyoscine (Buscopan) could additionally be useful in colicky pain. Guidelines for opioid prescribing Palliative care goals neither to hasten nor prolong the dying process and is unambiguously distinct from euthanasia. The precept of double impact focuses on the intent of relieving suffering, however acknowledges that, in terminal phases, abatement of futile life-sustaining therapy could foreseeably but unintentionally alter the time of dying. Non-pharmacological antinausea strategies embody avoiding the scent of cooking meals, frequent and smaller meal parts, nervousness management strategies and acupuncture. Strategies include upright posture, loose clothes, managed expiration, relaxation, chest physiotherapy, ethereal environment. Anticholinergics (such as hyoscine, atropine and glycopyrrolate) reduce the secretions and gurgling. Fatigue Fatigue is often multidimensional and could additionally be as a end result of correctable causes (anaemia, infection, respiratory illness, endocrine cause) or subjectively related to terminal sickness and deconditioning. Strategies corresponding to exercise, exercise planning, sleep hygiene, vitamin and biochemical correction, glucocorticoids could additionally be trialled. Terminal restlessness that is multifactorial (secondary to pain, discomfort, opiate toxicity, psychological distress). Practise good sleep hygiene; drugs of alternative are diazepam, levomepromazine and midazolam. Apart from supportive psychotherapy, there must be a low threshold for initiating pharmacologic measures. Correctable causes ought to be identified and � handled, apart from implementing varied adjunct methods. Legal points might include discussions surrounding resuscitation standing, appointing an influence of attorney and guardianship. Prognostication is challenging however fashions are used to estimate disease trajectories of most cancers, organ failure and dementia. This chapter describes these circumstances in addition to offering a systematic strategy to electrolyte abnormalities.
Standardized Extract of Grapefruit (Grapefruit). Crestor. - Asthma, lowering cholesterol, hardening of the arteries (atherosclerosis), preventing cancer, weight loss, psoriasis, muscle fatigue, promoting hair growth, toning the skin, reducing acne and oily skin, treating headaches, stress, depression, infections, digestive complaints in people with eczema, yeast infections (as a vaginal douche), and other conditions.
- Are there any interactions with medications?
- Are there safety concerns?
- Dosing considerations for Grapefruit.
- How does Grapefruit work?
- What is Grapefruit?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96909
Crestor 5mg with amexIt is preferable that loss of quantity be detected earlier than lack of physiologic compensation and clinical shock happen cholesterol levels uk chart order crestor mastercard. Physiologic Response to Changes in Posture When an individual assumes the upright posture, complicated homeostatic mechanisms compensate for the effects of gravity on the circulation to keep cerebral perfusion with minimal change in vital signs. These responses embody (1) baroreceptormediated arteriolar vasoconstriction; (2) venous constriction and increased muscle tone within the legs and the abdomen to increase venous return; (3) sympathetic-mediated inotropic and chronotropic results on the guts; and (4) activation of the renin-angiotensin-aldosterone system. The usually elevated sympathetic tone on standing is paradoxically inhibited, and an exaggerated enhancement of parasympathetic activity (bradycardia) occurs and may result in syncope. One research of 23 younger adult volunteers from whom 500 to 1200 ml of blood was withdrawn discovered no reliable change in postural blood pressure, and a constant postural improve in pulse of 35% to 40% was famous after 500-ml blood loss. Following phlebotomy of 450 to a thousand ml of blood from wholesome volunteers, the criterion of a rise in pulse of 30 Typical pressures in a normal particular person. The findings, based mostly on resting pressures, show no evidence of occlusive disease of the large- or medium-sized arteries. The findings are suggestive of right popliteal occlusion or right anterior and posterior tibial occlusion, or each. An inadequate quick compensatory response will result in dizziness, altered psychological status, or loss of consciousness. This causes arteriolar vasoconstriction, conservation of salt and water by the kidneys, and a shift in fluid from the interstitium to the intravascular area. Blood pressure and pulse are recorded after the patient has been supine for two to 3 minutes. Blood strain, pulse, and signs are recorded after the patient has been standing for 1 minute; the affected person ought to be permitted to resume a supine position instantly if syncope or near-syncope develop. This instructed guide is based on the flexibility of the change in pulse and affected person signs to distinguish between no acute blood loss and 1000-mL acute blood loss in healthy, beforehand normovolemic volunteers (sensitivity of 98% for detecting 1000-mL acute blood loss. The sensitivity and specificity of utilizing the aforementioned criteria for detecting 1000-ml blood loss (Box 1. The investigators were unable to constantly detect blood loss of 500 ml with these standards. Of notice, these authors discovered that a change in coronary heart rate of 30 beats/min or higher was 13. The discovering of a major rise in pulse, although insensitive for 500-ml blood loss, was comparatively particular in these wholesome grownup blood donors. Most of the situations that have an effect on postural blood strain regulation involve a pathologic condition that impacts the sympathetic nervous system or the usage of medications that alter regular cardiovascular compensatory capabilities. Even in regular individuals, passive tilting generates a excessive incidence of orthostatic syncope. These changes may be severe sufficient to produce frank syncope, particularly within the elderly. Patients with orthostatic hypotension as the purpose for syncope have been older, had extra comorbid conditions, and had been discovered to be extra regularly taking antihypertensive drugs. The investigators concluded that an orthostatic enhance in pulse of higher than 25 beats/min constitutes a optimistic tilt test and fewer than 20 beats/min constitutes a negative take a look at (sensitivity of 75%, specificity of 95%, and predictive worth of 92% when using near-syncope or an increase in heart fee greater than 25 beats/min). Bradycardia in the face of hemorrhage has usually been thought of a preterminal finding of irreversible shock, and bradycardia has been documented in hypovolemic, conscious trauma patients as properly. This paradoxical bradycardia could also be extra regularly associated with speedy and massive bleeding. Indications and Contraindications When the amount status of a affected person is assessed with the utilization of orthostatic vital signs, several factors must be remembered. Many elements affect orthostatic blood stress, including age, preexisting medical circumstances, medications, and autonomic dysfunction. It must be emphasised that information relating the impact of blood loss to orthostatic vital indicators are limited to phlebotomized healthy volunteers. Orthostatic important indicators can be considered an adjunct for the analysis of any patient with identified or suspected loss of blood quantity or a history of syncope. Contraindications to orthostatic measures embody supine hypotension, the medical syndrome of shock, severely altered mental standing, the setting of attainable spinal injuries, and decrease extremity or pelvic fractures. The use of medicines that block the normal vasomotor and chronotropic response to orthostatic tests is also a contraindication to using this take a look at for the evaluation of quantity status. In these situations, the primary discovering may be the sensation of near-syncope with little or no change in very important indicators. In sufferers receiving intravenous rehydration therapy, serial orthostatic very important signs are broadly used to judge the tip point of remedy earlier than launch. In one examine, individual orthostatic important sign response to saline infusion in ladies with hyperemesis gravidarum was related to other measures of rehydration, together with weight achieve and decreased urine specific gravity. A number of studies have been performed on normotensive, normovolemic sufferers to assess finish factors for orthostatic very important sign parameters. Such research have included sitting-tostanding methods and varying rates of postural adjustments,181 together with lying occasions of 5 to 10 minutes and standing instances of 0 to 2 minutes. Interpretation the most delicate criteria for orthostasis are tachycardia or symptoms of cerebral hypoperfusion. Specific population-based thresholds for adjustments in pulse fee and blood stress have some worth in figuring out patients at high risk for important loss of blood volume, but nice individual variability limits using this system as a screening check. That is, a lack of 500 ml, and infrequently extra, may be associated with a unfavorable orthostatic vital signal assessment. The scientific interpretation of orthostatic changes in blood pressure and pulse varies extensively. Technique To acquire orthostatic important signs, record the blood pressure and pulse after the affected person has been in the supine position for 2 to 3 minutes (see Box 1. Next, ask the affected person to stand and be ready to help if extreme signs or syncope develop.
[newline]If severe signs develop on standing, defined as syncope or excessive dizziness requiring the patient to lie down, the test is considered optimistic and should be terminated. If not symptomatic, allow the patient to stand for 1 minute after which record the blood pressure and pulse. A 1-minute interval resulted within the best distinction between management and 1000-ml phlebotomy groups in a single examine. Delayed capillary refill is an indication of reduced skin turgor, usually on account of volume depletion or restricted perfusion. The minimum strain necessary to produce blanching yields the most reproducible values. Release the nail mattress and start timing with a stopwatch or simply by counting out "one-thousand-one, one-thousand-two" for an approximation of the interval. Interobserver reliability has been shown to be reasonable, with kappa values of lower than zero. An incapability to preserve regular body temperature is indicative of a vast number of probably critical disorders, including infections, neoplasms, shock, poisonous reactions, and environmental exposures. Whether taken by the oral, rectal, or tympanic routes, reports of fever at residence are very difficult to interpret in the clinical setting. Environmental circumstances corresponding to ambient air temperature can falsely alter capillary refill. Measurements obtained from the nail mattress were extra reproducible than those from the heel.
Cheap crestor 5 mg mastercardPain usually begins as soreness after working that worsens after which occurs while strolling or climbing stairs cholesterol levels of seafood discount crestor 20 mg otc. Clinical Focus 6-23 Osteosarcoma of the Tibia Osteosarcoma is the most common malignant bone tumor of mesenchymal origin. It is extra frequent in males and often happens earlier than 30 years of age, usually in the distal femur or proximal tibia. The tumors often invade cortical bone on this region due to its wealthy vascular supply and then infiltrate surrounding gentle tissue. Tibia Fibula Interosseous membrane Osteosarcoma of proximal tibia presents as localized, tender prominence. Area of pain Posterior view Anterior view (muscle in phantom) Tibialis posterior muscle originates at posterior floor of tibia, interosseous membrane, and fibula and inserts on undersurface of navicular bone, cuboid, all three cuneiform bones, and 2nd, third, and 4th metatarsal bones. Upper arrows point out course of excessive traction of tendon on tibial periosteum and interosseous membrane attributable to hypereversion (lower arrows). Are supplied by the posterior tibial artery (the popliteal artery divides into the anterior and posterior tibial arteries) with some provide from the ibular artery (a branch of the posterior tibial artery). Anterior Compartment Leg Muscles, Vessels, and Nerves he muscles of the anterior compartment exhibit the next options. Several of those muscles can invert the foot, and one muscle (ibularis tertius) can weakly evert the foot. Are innervated by the deep ibular nerve (the common ibular nerve divides into the supericial and deep branches). Lateral Compartment Leg Muscles, Vessels, and Nerves he two muscular tissues of the lateral compartment exhibit the following options. Leg in Cross Section he interosseous membrane and intermuscular septae divide the leg into three compartments. Fibula Superior extensor retinaculum Inferior extensor retinaculum Extensor digitorum longus tendons Fibularis tertius tendon Dorsal digital nn. Medial malleolus Tibialis anterior tendon Extensor hallucis longus tendon Extensor hallucis brevis tendon Dorsal digital aa. Lateral malleolus and arterial network Extensor digitorum brevis and extensor hallucis brevis mm. Moreover, the leg is ensheathed in a tight deep fascia, and a few of the underlying muscle ibers actually connect to this fascial sleeve. Anterior compartment: muscle tissue that dorsilex (extend) and invert/evert the foot at the ankle and lengthen the toes, are innervated by the deep ibular nerve, and are supplied by the anterior tibial artery. Lateral compartment: muscle tissue that evert the foot on the ankle and weakly plantarlex the foot, are innervated by the supericial ibular nerve, and are supplied by the ibular artery. Fibula Posterior intermuscular septum Superficial posterior compartment Superficial flexor mm. Deep fascia of leg Tibia Interosseous membrane Deep posterior compartment Deep flexor mm. Valgus is used to describe the bone distal to the examined joint; a valgus angulation refers to a slight lateral angle. Excessive valgus angulation is called genu valgum, or knock-knee, and an excessive varus angulation is identified as genu varum, or bowleg. These deformities happen in growing kids and are often associated to rickets, skeletal dysplasia, or trauma. Two brothers, youthful (left) with bowleg (genu varum), older (right) with knock-knee (genu valgum). Clinical Focus 6-25 Exertional Compartment Syndromes Anterior (tibial) compartment syndrome (or anterior or lateral shin splints) happens from extreme contraction of anterior compartment muscle tissue; pain over these muscle tissue radiates down the ankle and dorsum of the foot overlying the extensor tendons. Lateral compartment syndrome occurs in people with excessively mobile ankle joints in which hypereversion irritates the lateral compartment muscles. These conditions are often continual, and enlargement of the compartment might result in nerve and vessel compression. In the acute syndrome (rapid, unrelenting expansion), the compartment could need to be opened surgically (fasciotomy) to relieve stress. The five Ps of acute anterior compartment syndrome are: Pain Pallor Paresis (footdrop, attributable to compression of deep fibular nerve) Paresthesia Pulselessness (variable) Anterior compartment syndrome Lateral compartment syndrome Tibialis anterior Extensor digitorum longus Fibularis longus Extensor hallucis longus Fibularis brevis Area of ache Area of ache Chapter 6 Lower Limb 331 6 Clinical Focus 6-26 Achilles Tendinitis and Bursitis Tendinitis of the calcaneal (Achilles) tendon is a painful irritation that often happens in runners who run on hills or uneven surfaces. Repetitive stress on the tendon happens as the heel strikes the ground and when plantarflexion lifts the foot and toes. Retrocalcaneal bursitis, an inflammation of the subtendinous bursa between the overlying tendon and the calcaneus, presents as a tender space just anterior to the tendon attachment. Tendinitis Uphill working, especially in footwear with poorly versatile soles, places pressure on Achilles tendon at toe-off. Bursitis Achilles tendon Palpating for tenderness in front of Achilles tendon Retrocalcaneal bursa Tuberosity of calcaneus Fat pad Achilles tendon (tendo calcaneus), with irritation at its insertion into tuberosity of calcaneus Achilles tendon 7. A variety of actions are attainable at these joints, and the ankle and foot can provide a stable however lexible platform for standing, walking, and running. Because of the form of the talus (the anterior portion of its superior articular facet is wider), the ankle is more secure when dorsilexed than when plantarlexed. Transverse arch: extends from lateral to medial across the cuboid, cuneiforms, and base of the metatarsals; is higher medially than laterally. Supporting muscular tissues embody the tibialis anterior, tibialis posterior, and fibularis longus. Chapter 6 Lower Limb Right foot: lateral view Tibia 335 6 Fibula Anterior and Posterior tibiofibular ligs. Flexor digitorum longus tendon to 2nd toe (cut) Posterior view with ligaments Tibia Fibula Interosseous membrane Posterior tibiofibular lig. Fibularis (peroneus) longus tendon Tibialis anterior tendon (cut) Plantar cuneonavicular lig. Phalangeal bones Distal Middle Proximal Joint capsule Metatarsal bone Plantar calcaneocuboid (short plantar) lig. Flexor hallucis longus tendon (cut) Flexor digitorum brevis tendon to 2nd toe (cut) Plantar metatarsal ligs. Fibularis (peroneus) brevis tendon Capsules and ligaments of metatarsophalangeal and interphalangeal joints: lateral view Plantar lig. A affected person with footdrop should raise the knee in the course of the swing part of gait to avoid dragging the affected foot on the ground or to keep away from tripping. This distinctive gait pattern is known as "steppage" gait, and at the finish of the swing phase, the foot slaps right down to the ground. Typically, footdrop outcomes from injury to the widespread fibular nerve or deep fibular nerve. The frequent fibular nerve is weak to injury as a result of it lies superficially beneath the pores and skin where the nerve passes around the fibular neck (coffee desk or automotive bumper height). This nerve additionally could also be affected by a herniated disc that compresses the L5 nerve root (L4-L5 herniated disc; see Chapter 2). Clinical Focus 6-28 Ankle Sprains Most ankle sprains involve an inversion harm when the foot is plantarflexed, putting stress on the elements of the lateral collateral ligament. Often the severity of the injury happens from anterior to posterior, involving first the anterior talofibular ligament, then the calcaneofibular ligament, and at last, if particularly extreme, the posterior talofibular ligament.
5mg crestor otcArtificial Airway Placement the only and most widely out there synthetic airways are the oropharyngeal and nasopharyngeal airways cholesterol lowering food today tonight purchase discount crestor line. Both are meant to forestall the tongue from obstructing the airway by creating a passage for air between the bottom of the tongue and the posterior pharyngeal wall. In cases of extreme upper airway edema, such as angioedema, these devices might not perform correctly or be ready to bypass the obstruction. A second approach is to open the mouth widely, use a tongue blade to displace the tongue, after which simply advance the bogus airway into the oropharynx. Some clinicians insert a nasopharyngeal airway to dilate the nasal passages for 20 to Oropharyngeal and Nasopharyngeal Artificial Airways Indications and Contraindications Once the airway has been opened with guide maneuvers and suctioning, synthetic airways, such as nasopharyngeal and Oropharyngeal and Nasopharyngeal Airways Indications Facilitation of spontaneous breathing and bag-valve-mask ventilation in sufferers requiring head-tilt/chin-lift or jawthrust maneuvers Equipment Contraindications Nasopharyngeal Significant facial and basilar cranium fractures Complications Oropharyngeal Vomiting (in sufferers with an intact gag reflex) Airway obstruction (if the tongue is pushed towards the posterior pharyngeal wall during insertion) Nasopharyngeal Epistaxis Deterioration requiring intubation (semiconscious patient) Nasopharyngeal airway Oropharyngeal airway Review Box three. An airway of right measurement will extend from the nook of the mouth to the earlobe or the angle of the mandible. Simply advance it into the nostril and direct it alongside the floor of the nasal passage in the direction of the occiput, not cephalad. Advance it fully until the flared external tip of the airway is situated at the nasal orifice. An oropharyngeal airway of the proper size will prolong from the nook of the mouth to the tip of the earlobe. Both oropharyngeal and nasopharyngeal airways present airway patency similar to that achieved with the head-tilt/ chin-lift maneuver. Complications the nasopharyngeal airway may cause epistaxis and may be dangerous in sufferers with significant facial and basilar skull fractures. Semiconscious patients with nasopharyngeal airways may deteriorate and require intubation, so they need to be monitored carefully. The oropharyngeal airway could induce vomiting when placed in patients with an intact gag reflex. It can also cause airway obstruction if the tongue is pushed against the posterior pharyngeal wall during insertion. The best factor to manipulate is the partial strain of inspired O2, which is completed by rising the fraction of inspired oxygen (FiO2) with supplemental O2. The half-life of carboxyhemoglobin is four to 5 hours in a patient breathing room air however can be decreased to roughly 1 hour by the administration of 100% O2 by non-rebreather face masks at atmospheric pressure. Never withhold oxygen remedy from a hypoxemic patient for fear of problems or scientific deterioration. Rather, it demands that the clinician administer O2 rigorously and recognize the potential for respiratory acidosis and clinical deterioration. Indications and Contraindications Resuscitate all sufferers in cardiac or respiratory arrest with 100% O2. The most sure indication for supplemental O2 is the presence of arterial hypoxemia, outlined as an arterial oxygen partial strain (PaO2) lower than 60 mm Hg or arterial oxygen saturation (SaO2) less than 90%. Whatever the cause of the shock state, administration of O2 is indicated until the scenario can be thoroughly evaluated and cause-specific remedy instituted. It is reasonable to administer O2 to hypotensive patients and those with extreme trauma until tissue hypoxia can definitively be excluded. Patients with normal respiratory rates and tidal volumes will require much less outside air than these in respiratory distress, and due to this fact patients not in respiratory distress typically obtain a better FiO2 than sufferers in respiratory distress, assuming equivalent supplemental oxygen move rates. The prongs of a nasal cannula deliver a constant circulate of O2 that accumulates within the nasopharynx and offers a reservoir of oxygen-enriched air for inspiration. Oxygen is important to these goals, and during cardiac arrest blood move is the most important limiting factor to sufficient oxygen supply to the heart and brain. Thus, 100 percent FiO2 must be administered during cardiac arrest for adults, kids, and neonates to maximize oxygen delivery to vital organs. It is acknowledged that titration of impressed oxygen will not be attainable immediately after out-of-hospital cardiac arrest until the patient is transported to the emergency department or, in the case of in-hospital arrest, the intensive care unit. The optimal FiO2 in the course of the immediate period after cardiac arrest remains to be debated. The helpful effect of high FiO2 on systemic oxygen supply ought to be balanced with the deleterious effect of producing oxygen-derived free radicals in the course of the reperfusion part. Data from human studies is mixed, with no clear proof of harm or profit from hyperoxia. The goal oxyhemoglobin Oxyhemoglobin saturation might normally remain in the 70% to 80% vary for several minutes following birth, thus ensuing in the appearance of cyanosis during that point. Clinical evaluation of pores and skin shade is a very poor indicator of oxyhemoglobin saturation through the quick neonatal period and that lack of cyanosis seems to be a really poor indicator of the state of oxygenation of an uncompromised child following start. Optimal administration of oxygen throughout neonatal resuscitation becomes notably important because of the evidence that either insufficient or excessive oxygenation can be dangerous to the newborn toddler. Two metaanalyses of a quantity of randomized controlled trials evaluating neonatal resuscitation initiated with room air versus 100 percent oxygen showed increased survival when resuscitation was initiated with air. It is beneficial that the aim in babies being resuscitated at delivery, whether or not born at time period or preterm, should be an oxygen saturation worth within the interquartile vary of preductal saturations measured in wholesome time period babies following vaginal delivery at sea level (see later). These targets may be achieved by initiating resuscitation with air or blended oxygen and titrating the oxygen focus to obtain an SpO2 within the goal range utilizing pulse oximetry. If the child is bradycardic (heart fee <60 beats per minute) after ninety seconds of resuscitation with a decrease focus of oxygen, oxygen concentration must be increased to 100% until recovery of a traditional heart rate. Most importantly, at a relentless O2 move rate, FiO2 varies inversely with the respiratory rate. They can be used with higher flow charges for transient periods of time, but are uncomfortable to use in this manner and trigger nasal dryness and irritation. Nasal cannulas are usually set to 2 to 4 L/min, which offers approximately 30% to 35% FiO2. Simple masks obtain a continuing flow of O2 from the O2 supply and have a number of vent holes. During inspiration the oxygen-enriched air that has accumulated within the mask, along with room air entrained via the vent holes, is inhaled. During expiration, 200 mL (the approximate quantity of the mask) of exhaled gasoline is deposited in the masks, with the rest exiting through the vent holes. The steady move of O2 then partially washes out the mask earlier than the subsequent inspiration. Flow meters able to exactly measuring move up to 70 L/ min are commercially out there, which permit the clinician to deliver greater move charges and thus greater FiO2. A complex interaction between masks quantity, tidal volume, respiratory fee, and O2 move determines the FiO2 delivered to the patient. A partial non-rebreather mask incorporates a bag-type reservoir to improve the quantity of O2 obtainable throughout inspiration, thereby requiring less outside air to be entrained. Nonrebreathing masks are similar to partial rebreathing masks however have a series of one-way valves. One valve lies between the mask and the reservoir and prevents exhaled gas from getting into the reservoir. Two valves in the facet of the masks allow exhalation while preventing the entry of outside air.

Best crestor 10 mgPatients may be unaware of their inability to scent adequately and that is normally picked up on routine investigation cholesterol levels mayo clinic order 20mg crestor with amex. The condition can be related to other congenital abnormalities, similar to cleft palate and hearing loss, but these symptoms vary from patient to patient. Characteristics embody: � Tall, slender, long-limbed � Infertility with small testes � Decreased facial, pubic hair � Learning disabilities four. Associations embody: � Short stature � Webbed neck (appears in 20�25% of circumstances; see. To arrive at an correct analysis, the doctor needs to use a combination of thorough history-taking, scientific examination (with the goal of localising the lesion if possible), appropriate imaging investigations, and a degree of sample recognition. Bridge to clinical medicine the neuron and action potential � the basic structural and useful unit of the nervous system is the neuron, a cell designed to transmit and receive chemical and electrical indicators, permitting for speedy communication. Each axon is myelinated in such a method that there are gaps between every myelinated area, often identified as nodes of Ranvier. These properties make impulses that journey by way of myelinated axons a lot quicker than those travelling via their unmyelinated counterparts. A score is given, ranging from 0 to 5, relative to the utmost effort expected for that muscle (see Table 5. The anterior spinothalamic tract fibres specialize in transmitting the sensations of crude touch and pressure. Distributed on the orbital floor and the whole medial floor of each hemisphere, it curves again and over the roof of the corpus callosum, as far as the parieto-occipital sulcus. This might trigger: � Contralateral hemiparesis/hemiplegia � Contralateral sensory deficit � Apraxia � Anosmia � Urinary incontinence. It travels in the lateral sulcus, supplying the insular cortex, posterior limb of the inner capsule and basal ganglia. Their brief preganglionic fibres synapse with lengthy postganglionic neurons (in ganglia) in the sympathetic ganglion chain (alongside the spinal cord). Postganglionic fibres carry on from the ganglion chain until they attain their effector organ. Heart rate, respiratory fee and blood stress improve, as does sweat gland activity. Their longer preganglionic fibres synapse with shorter postganglionic fibres at a terminal ganglion, which lies close to the effector organ. They promote bodily actions that happen in relaxed situations, such as digestion. Hence, they transmit sensory information from sensory organs to the spinal cord, in addition to motor info from the spinal cord to the effector organ � the cranial nerves are 12 pairs of peripheral nerves acting between the brainstem and effector organs. Most organs are innervated with each sympathetic and parasympathetic nerves, or dual autonomic innervation. Muscles just like the diaphragm remain depolarised, unable to return to their resting situation. This will result in swollen optic head with excessive axoplasm, leading to papilloedema. A fourth nerve palsy features a mixture of vertical diplopia and excyclotorsion, with an occasional presentation of compensatory head tilt/turning to the opposite side of the palsy. A patient with right fourth nerve palsy will show a rise in hyperdeviation (of the affected side) on ipsilateral head tilt. This hyperdeviation is absent when the head is tilted to the contralateral side (positive test). Sixth nerve palsy leads to esotropia of the affected aspect due to unopposed action of the medial rectus, and limited abduction of the affected eye, resulting in horizontal diplopia. P Parinaud syndrome (also generally recognized as dorsal midbrain syndrome) refers to a disease process characterised by vertical gaze palsy (impaired capability to look up or down), convergence nystagmus or diplopia. Patients with a quantity of sclerosis are also at higher threat of developing Parinaud syndrome. Vertigo itself implies a false sense of movement or a spinning sensation, versus the sensation of being off-balance or blacking out. Helpful considerations include the presence of hearing loss as a symptom, as nicely as the duration of symptoms. Vertigo with hearing loss is more often brought on by M�ni�re disease or labyrinthitis. Persistent vertigo may also point in direction of a analysis of labyrinthitis or vestibular neuronitis. Investigations Stepwise plan: 1 Ask for any history of rheumatoid arthritis or neck or back pain, which can complicate further investigations � Examine the ear and the realm round it 2 Arrange a Dix�Hallpike take a look at Management Advise the patient not to drive or carry out work that might be adversely affected by vertigo. Epidemiology: � Typically affects individuals above the age of 50 � Affects more girls than males Brandt�Daroff exercises Instruct the individual on tips on how to perform these exercises at house. This is caused by herpes zoster and is related to a painful rash and herpetic vesicles. Note the right facial paralysis (with higher face involvement) when the affected person was requested to smile. Patients with syncope require thorough evaluation so as to determine the underlying trigger. Asking for options of the syncopal occasion (including period and associated symptoms), notably from witnesses, is exceptionally useful. Todd paresis refers to focal weakness of a physique half post-ictally (after a seizure). It most commonly impacts the upper or decrease limbs and is consigned to either the left or right half of the body, but may also affect speech or vision. The situation was noticed by Robert Bentley Todd, a popular Irish-born London physician, in 1849. This manifests itself as a disturbance of consciousness, behaviour, emotion, motor perform or sensation. The International League Against Epilepsy (2014) defines epilepsy as a disease of the brain, defined by any of the following situations: � At least two unprovoked seizures occurring more than 24 hours apart � One unprovoked seizure and a likelihood of additional seizures just like the general recurrence risk after two unprovoked seizures, occurring over the following 10 years � Diagnosis of an epilepsy syndrome (various types) Only one-third of sufferers are mentioned to have an attributable trigger. Patients with a constructive household history, studying disabilities and former neurological infections are at increased threat. Status epilepticus is a continuous seizure for 30 minutes or longer, or recurrent seizures with out regaining consciousness lasting 30 minutes or longer (see Chapter 12). Broadly, seizures may be grouped into: � Simple focal (partial) � Focal motor or sensory symptoms � Usually arises from one area of the brain � Consciousness retained � Most common type of partial seizure arises from the temporal lobe � patients could describe an aura (vague gastric discomfort) � Complex focal (partial) � May have previous aura (unexpected tastes, smells, paraesthesias or a rising abdominal sensation) earlier than loss of consciousness 5. Lamotrigine is the drug of choice in this case, as sodium valproate is associated with the event of neural tube defects. P Patients may also present with a conversion disorder related to epilepsy, generally identified as a psychogenic non-epileptic seizure. Patients with this situation have a variable presentation, could have relapsing jerking actions (sometimes related to pelvic movement) and will have a historical past of trauma or abuse. The International Headache Society (2013) differentiates headaches into major and secondary classes. A secondary headache normally has an attributable trigger, and is prone to be of greater severity.
Discount crestor amexAfter needle placement is confirmed cholesterol medication drinking alcohol buy crestor with american express, a temporary drain can be positioned by the Seldinger method, described in Chapter 22. Remove the syringe from the needle, advance a guidewire via the needle, after which remove the needle. Remove the dilator and slide an introducer sheath dilator (6 to 8 Fr Cordis) over the wire. Insert the pigtail angiocatheter by way of the introducer sheath, and aspirate fluid to verify placement. Attach the catheter to a three-way stopcock and connect it to a water seal to drain by gravity. The pigtail catheter permits extended drainage and protected access into the pericardial sac without requiring the introduction of one other needle. Blood retrieved from the ventricle usually clots faster than bloody fluid aspirated from the pericardium. In basic, hemorrhagic pericardial effusions have native fibrinolytic exercise, which prevents clot formation. The hematocrit of pericardial fluid ought to all the time be decrease than that of a pattern from the systemic vascular system, except in sufferers with aortic dissection or acute myocardial rupture. These circumstances apart, a hematocrit value similar to that for systemic blood should increase concern for an intracardiac needle location. Several different simple laboratory tests can differentiate regular from abnormal pericardial fluid, however they require the supply of a centrifuge system and time. Immediately following the process, get hold of a chest film to make certain the absence of pneumothorax and free air beneath the diaphragm. C, the shaft of the pigtail catheter (arrowhead, two discrete parallel echogenic lines replicate the catheter walls; the echo-free space represents the catheter lumen) lying within the pericardial area after the majority of fluid has been drained. Prepare a saline echocardiographic contrast medium by utilizing two 5-mL syringes, one with saline and the opposite with air. Monitor the doorway of the agitated saline into the pericardial house sonographically- it seems as a brightly echogenic stream. Suture the pigtail catheter to the skin, however be careful to not occlude the catheter by tying it too tightly. It is critical for the emergency doctor to pay consideration to each the standard and up to date methods of performing the procedure and the problems that could be related to these methods (see Review Box sixteen. Complication rates as low as 4% have been reported in large observational research. Earlier studies of blind pericardiocentesis documented morbidity rates of 20% to 40% and mortality charges as high as 6%. Cardiac arrest and demise are not often associated with echocardiographically guided pericardiocentesis. When blind or electrocardiographically guided pericardiocentesis is carried out, the patient is normally already in full arrest and attributing the cause of dying to the process is almost impossible. In a sequence of 52 sufferers the only demise occurred in a affected person in cardiogenic shock in whom pericardiocentesis was nonproductive and who was discovered to have severe arteriosclerotic coronary heart disease, not tamponade, on postmortem examination. The two deaths occurred during or after the process, but whether or not they might be attributed to the process is unclear. One affected person with aortic rupture that penetrated into the pericardial space died of cardiac arrest instantly after the puncture. One of the most frequent problems is a dry tap, particularly when a blind strategy is used. A dry tap is commonly attributable to blockage of the needle with clotted blood or a skin plug. With the parasternal strategy, the needle can turn out to be blocked by vigorous probing of the anterior costal cartilage. Preventricular contractions are frequently noted after the needle enters the pericardial sac; however, no severe dysrhythmias leading to hemodynamic compromise have been talked about within the literature. A minor pneumopericardium is inconsequential; a bigger assortment could cause tamponade. Maggiolini and colleagues reported transient third-degree heart block in a single affected person. Fortunately, inadvertent needle passage into the liver has not been reported to trigger important hemorrhage or dying. There have additionally been rare stories of pneumopericardium after removing of a pericardiocentesis catheter. The explanation for the pneumopericardium is thought to be the formation of a bronchopericardial fistula, however the actual mechanism is unclear. The mortality rate related to pressure pneumopericardium is approximately 50%, so contemplate pneumopericardium when patients complain of dyspnea and hypotension after removing of their catheter. These problems occur extra regularly during blind or electrocardiographically guided procedures. In patients taking anticoagulants, it is necessary to examine coagulation factors and monitor them closely after a seemingly insignificant pericardiocentesis as a outcome of hemopericardium may develop just from the process itself. In the series compiled by Krikorian and Hancock,126 hemopericardium developed in 13 of 123 patients as a end result of pericardiocentesis, one because of a lacerated coronary artery. In their series of 352 procedures, duvernoy and associates168 reported 23 penetrations. Researchers differ in their opinions concerning the adverse results of ventricular puncture. In a collection of sufferers who underwent ultrasound-directed pericardiocentesis, ventricular puncture occurred in 1. Rare cases of severe left ventricular pseudoaneurysm after pericardiocentesis have been reported. This imbalance could cause vital penalties for both proper and left ventricular function. Three of six patients in whom giant effusions had been removed by pericardiocentesis experienced proper ventricular dilation and overload, irregular septal motion, and both no enhance or a lower in the right ventricular ejection fraction. Rotate rescuers aggressively (approximately each 2 to 3 minutes) to keep away from deteriorating high quality of compressions due to exhaustion. Minimize pauses in chest compressions as a end result of even short pauses have profound effects on coronary perfusion stress and outcomes. Cardiopulmonary Resuscitation and Artificial Perfusion During Cardiac Arrest Benjamin S. Each minute with out treatment, nonetheless, is associated with a 10% to 15% lower within the likelihood of survival. For instance, shallow chest compressions have an antagonistic influence on the success of defibrillation. These pointers are formulated through a formalized knowledge evaluation process and are up to date each 5 years, final up to date in 2015. In addition, pauses in chest compressions are too lengthy, and hyperventilation of arrest patients is frequent. The group chief must be vigilant in the statement of delivery of ventilations and ought to be ready to verbally immediate rescuers to ventilate the affected person at the acceptable fee if hyperventilation is performed. Attempt pulse detection on the location of the carotid or femoral artery as a result of peripheral pulse checks throughout profound shock or cardiac arrest states are notoriously unreliable.
References - Chiang PM, Yuan RH, Hsu HC, et al. Frequent nuclear expression of betacatenin protein but rare beta-catenin mutation in pulmonary sclerosing haemangioma. J Clin Pathol 2008;61:268-71.
- Fitch D. The small bowel see-through: an improved method of radiographic small-bowel visualization. Can J Med Radiat Tech 1995; 26:167-171.
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994; 149:818-24.
- Li Y, Sabatine MS, Tong CH, et al. Genetic variants in the KIF6 region and coronary event reduction from statin therapy. Hum Genet 2011;129:17-23.
- Savides TJ, Perricone A. Impact of EUS-guided FNA of enlarged mediastinal lymph nodes on subsequent thoracic surgery rates. Gastrointest Endosc. 2004;60(3):340-346.
- Kass EJ, Freitas JE, Salisz JA, et al: Pituitary gonadal dysfunction in adolescents with varicocele, Urology 42:179n181, 1993. Kass EJ, Marcol B: Results of varicocele surgery in adolescents: a comparison of techniques, J Urol 148(2 Pt 2):694n696, 1992.
|


