|
Mayank V. Patel, MD - Department of Surgery
- Our Lady of Mercy Medical Center
- Westchester Square Medical Center
- Bronx, New York
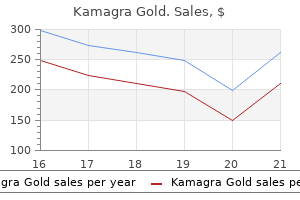
Kamagra Gold dosages: 100 mg
Kamagra Gold packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills

Purchase generic kamagra goldThe rostral end begins to enlarge and types the three successive primary brain vwioles: forebrain (prosencephalon) erectile dysfunction causes and symptoms generic 100 mg kamagra gold overnight delivery. As an anterior a half of the hindbrain, the m8lencephalon evolves beneath the mesencephalon; later its primary components would be the pons and cerebellum. Caudally the posterior part of the hindbrain follows, the myelencephalon; it includes the fourth ventricle and the Medulla oblongata and transitions into the spinal wire. The optic cups (or eve cups[become visible between the telencephalon and diencephalon. The improvement of the cerebellum begins with a lateral extension of the rhombencephalon. At the dorsal facet of the metencephalon, the growing cerebellum can already be seen. In this process the alar and basal plates lie next to each other, separated by the Sulcus limitans. The future nuclei of the cranial nerves are positioned symmetrically subsequent to each other. As a consequence, the primordial buildings of the cerebellum expand additional dorsally and, by uniting in the median line. The sagittal sections through the rhombencephalon in weak 8 (c) and in weak 17 (d) clearly show the ongoing development of the pons and cerebellum. C8Phalic veek:le (pnmonlial cerebral hemisphere) Decussation of fibres in the Pedunculua carabelll suparicr Subatentia nigra d Crus cerebrt Fossalnterpeduna. In week 5, the primordial mesencephalon emerges in the space of the Flexura mesencephalica. In relation to different components of the brain, the realm of the mesencephalon vesicle undergoes only minimal adjustments. The centrally positioned lumen narrows, because of the robust development of the lateral partitions. The surrounding tissue forms a roofplate (tectum) and a bigger ventral masking (tegmentum), which with its most anterior half because the Par-. From the alar plates which have arisen from the dorsal-lateral elements of the neural tube, neuroblasts migrate into the Tectum mesencephali and kind the paired Colliculi superiores and inferiores here. It is debatable whether the Nucleus ruber and the Substantia nigra originate from differentiated neuroblasts of the alar plates or roofplates (presented here is the formation of the Substantia nigra from the basal plates). Neuroblasts of the previous basal plates migrate into the Tegmentum mesencephali and kind the group of motor nuclei. In week 11, the construction of the mesencephalon has already developed to its definitive kind. Due to the increasing size/ growth of the telencephalon, the diencephalon is visible solely at a number of points from the skin. The former vesicle of the diencephalon differentiates additional into the parts of the diencephalon, including the hypothalamus with pituitary gland, thalamus, epithalamus and subthalamus. Grooves or depressions (Sulcus epithalamicus, Sulcus hypothalamicus) are shaped between the areas of the nuclei. The pituitary gland emerges from two kinds of tissue: (11 Around the 36111 day of improvement. Due to the considerably slower growth of the quilt plate, the quickly rising cerebral hemispheres arch over the duvet plate. Thereby, the Fissura longitudinalis superior is created between them; the former cowl plate is situated in the space of the later Corpus callosum. Thickening of the basal plate offers rise to the basal ganglia at the bottom of the lateral ventricles. The internal (subarachnoid) spaces of the cerebrospinal fluid emerge from the lumen of the neural tube. The ventricles and their speaking ducts are created by the quicker and slower growth charges in several parts. In the telencephalon, the crescent- or C-shaped growth path of the 2 cerebral hemispheres ends in the everyday construction of the primary and second ventrioles. The Plexus choroideus of the 2 lateral ventricles and of the third ventricle emerge from the cover plate. The ingrowing Capsula interne divides the Corpus striatum into Putamen and Nucleus caudatus. All afferent and efferent nerve fibres (tracts) to or from the telencephalon have to cross through the diencephalon. The nuclei situated here in the fields of the subthalamus are pushed apart by the fibres (tracts). In the area of the cerebral hemispheres, the Lobi frontalis, parietalis, occipitalis and tamparalis have already been formed. Only elements of the pons, cerebellum and Medulla oblongata are still seen structures of the brain stem. The Thombencephalon has differentiated into the metencephalon and the Medulla oblongata (myelencephalonl. Subsequently, convolutions (Gyril and grooves (Sulci) of the brain deve- lop incrementally [gyrlflcatlon, floor enlargement, combined with the formation of the Insula and its overlapping by the Lobi frontalis, parietal is and temporalis. The higher red circle marl<s the defect in the space of the small fontanelle, the lower purple circle indicates the defect in the space of the Foramen magnum. The term encephalocele (hernia cerebri, cerebral hernia, outer brain prolapse, skull bifidum) summarises faulty developmental malformations with a median gap of the cranium (at the basis of the nose, forehead, cranial base. This leads to the formation of the Fissura medians anterior and of the Sulcus medianus posterior. The lumen of the neural tube hardly enlarges and remains because the central canal [Canalis centralis). The efferent fibres emerge from the basal plata (later: the motor anterior hom) and form the Radix anterior. Afferent fibres assemble in the direction of the alar plate (later: the sensory posterior horn) and form the Radix posterior. The vertebral cleft often outcomes from the failed fusion of one or two vertebrae. Functionally, the nervous system is split into an autonomic (vegetative, visceral, to management visceral exercise, largely involuntary) and a 110matic (animalic, innervation of skeletal muscles, voluntary perception of sensory input. In addition to the nervous system, the endocrine system additionally participates in the regulation of the entire organism. Thereby the longitudinal axis of the forebrain (prosencephalon= diencephalon and telencephalon[tilts ahead. Consequently, a novel nomenclature is generated for the brain, as is proven in the determine. The scientific neurological examination features a bodily examination and a medical historical past to get hold of information in particular on earlier neurological illness, cranial-a~rebral trauma, congenital or familial neurological disorders, threat factors and autonomic features. This is complemented by a symptom-focused historical past and particular diagnostic methods to evaluate the cranial nerves and 1heir corresponding functional techniques. Disorders of the consciousness are clinically divided into somnolence (abnormal sleepiness.
Buy kamagra gold 100mg otcBelow the lesser trochanter erectile dysfunction usmle buy cheap kamagra gold 100 mg on-line, the Linea pectinea is positioned as the attachment of the M. The femoral shaft is largely round in diameter; only on the dorsal side is there a bony ridge known as the Linea aspera with a Labium mediale and a Labium laterale. Distally the shaft widens to the Epicondylus medialis and lateralis and ends in the two cylindrically-shaped joint surfaces of the knee joint (Condyli medialis and lateralis). Through the neck of the femur, the proximal parts of the shaft are displaced lateral of the axis line, in order that only the distal finish of the femur stays in the axis line. This lateralisation is essential, providing the small gluteal muscular tissues (running from the pelvic ring to the trochanter major) with a larger lever arm. In order to compensate for this loading, the spongious trabaeculae are longitudinally aligned to the arising forces (the trajectories). The antetorsion angle means the twisting of the shaft in relation to the knee joint axis. The neck of the femur, compared to this axis, is rotated by approximately 14� to the front, i. Due to incorrect loading on the cartilage, this leads to elevated put on and often contributes to the event of coxarthrosis (osteoarthritis of the hip). These are very common, particularly in older folks, in combination with osteoporosis. The femoral head and neck are mounted in place in the femoral shaft by the 2 trochanters. A connective tissue lip, the Labrum acetabuli, expands the articular surface and extends 203 5 Lower extremity over the Incisura acetabularis with the Lig. This joint lip extends over the equator of the femoral head, so that roughly two-thirds of the surface area of the ball are lined by the joint cup. This is a particular sort of ball joint known as a cotyloid joint (Articulatio cotylica, enarthrosis). As with the overlaying of the socket, the majority of the joint head is lined with cartilage. It is important that the femoral head is already positioned in the centre of the flat cup in infancy. Therefore, in infants the position of the femoral head is examined using ultrasound. If hip dysplasias like these (no overlaying of the femoral head by the Os coxae) remain uncorrected, this could usually lead to osteoarthritis of the hip joint. The femoral head may even exit the socket (hip dislocation) and result in the development of a new however functionally inefficient articular surface above the acetabulum. The joint capsule originates from the Limbus acetabuli and spans the femoral head and the largest a half of the femoral neck. It passes within the joint cavity from the Incisura acetabuli to the Fovea capitis femoris. Movement Extension/flexion Abduction/adduction External rotation/internal rotation Range of movement 10��0��130� 40��0��30� 50��0��40� Clinical remarks the truth that the femoral head is especially provided by blood vessels from the femoral neck is clinically extremely related. In the case of fractures, notably of the femoral neck or dislocations of the joint, these vessels are regularly broken. This can due to this fact result within the destruction of bone tissue and femoral head necrosis because of insufficient blood supply to the femoral head. This complication is also a cause why with femoral head fractures, a total endoprosthesis is normally implanted. In explicit, extension can only be exactly outlined with a hard and fast contralateral hip joint. When making an attempt to transfer the leg so far as attainable dorsally when standing, the contralateral hip joint is always bent. By doing this, the potential of further rotation within the other leg joints is eradicated. The hip joint can solely be very barely prolonged (important for stability when standing), however can be flexed very nicely (important for walking). This is achieved with the ligaments of the hip joint, which are all tensed in extension, but relaxed during flexion, (> Table 5. In addition, the ligaments prevent extreme adduction and abduction, as properly as extreme inner and exterior rotation. This pushes the hip barely forwards, tightening the ligaments as a end result of the slight extension that takes place within the hip. When standing for a protracted time, these ligaments present support, and this protects a substantial quantity of power. There are four teams of muscle tissue which have an effect on the movement of the hip joint: � Ventral muscles � M. Other muscular tissues of the thigh also move the hip joint; nevertheless, since in distinction to the adductor group, their main perform is the motion of the knee they will be dealt with there. The muscular tissues run ventral to the hip joint, so their primary function is the flexion of the joint. The muscle also plays a role in exterior rotation, especially when flexing the thigh. The cranial elements cross the hip joint above the sagittal axis, while the caudal part crosses beneath it. Therefore, the top half of the muscle carries out abduction actions, whereas the underside half takes half in adduction. This is a reinforcement of the thigh fascia (Fascia lata) on the lateral aspect, which inserts under the Condylus lateralis of the tibia. The Tractus iliotibialis is tasked with lowering the flexural stresses that act on the femoral neck, like a rigidity spring. Furthermore, in the case of bilateral paralysis of the muscle, straightening of the higher body with the hip joint from the reclined position is not potential. This is especially evident when climbing stairs, as a end result of here the leg needs to be stretched out from the flexed position. Weakening of the muscular tissues is the long-term effect of hip dysplasia with luxation (see above). They originate to the entrance of and cranial to the Facies glutea of the hip and pull forward laterally to the Trochanter main below. As a majority of the fibres are positioned ventral to the longitudinal axis, these muscles are additionally crucial medial rotators. When strolling, one leg remains secure on the bottom (standing leg), whereas the other leg M. Pelvitrochanteric (medial) muscles the pelvitrochanteric muscle tissue lie caudal to the M. They are all lateral rotators of the hip joint, because they run behind the longitudinal axis. It enters through the Foramen ischiadicum minus, redirected on the Corpus ossis ischii in the area of the Incisura ischiadica minor and inserts on the Trochanter main.
Cheap kamagra gold 100 mg without a prescriptionThe oesophagus emerges by way of the oesophageal hiatus in the lumbar a part of the diaphragm smoking causes erectile dysfunction through vascular disease discount kamagra gold 100 mg fast delivery. It is accompanied by an autonomic nerve plexus (Plexus oesophageus), the parasympathetic components of which turn out to be condensed above the oesophageal hiatus to the vagal bunks. The Truncus vagal is posterior visible here emerges throughout growth, predominantly from the fibres of the right N. The autonomic Plexus pulmonalls is formed notably strongly dorsally and accompanies the main bronchi to the hilum of the lung. Most difficult to identify is the brief Ductus lymphaticus dexter, which drains into the best venous angle (between the V. Before reaching its outlet it receives the Truncus bronchomediastinalis, the Truncus subclavius and the Truncus jugularis (not shown). A distinction is made between a systemic cln:ullltlon I= massive circulation) and a pulmonary cin:ullltion (=small circulation), which are related in a sequence. The heart is the father or mother organ of the cardiovascular system and drives the circulation as a suction and pressure pump. Accordingly, the heart is split into two halves, which each encompass an atrium and a ventricle (Ventriculus). In this way, blood is pumped from the center into arteries and returned via veins back to the heart. Oxygen content material for this division is negligible I In the systemic circulation, oxygenated blood from the left ventricle (Ventriculus sinister) is directed by way of the principle artery (aorta) and downstream arteries into outlying areas, the place the oxygen is used and carbon dioxide absorbed. The venous blood is correspondingly deoxygenated and is returned to the heart by way of the veins, which be part of to the sucavae superior and inferior) prior to perior and inferior venae cavae coming into the proper atrium (Atrium dextrum). This blood is then pumped from the right ventricle (Ventriculus dexter) via the Truncus pulmonalis and the pulmonary arteries into the pulmonary circulation, the place renewed oxygen absorption into the blood and exhalation take place. The pulmonary veins transport the oxygenated blood back into the left atrium (Atrium sinistrum) so that the circulation is completed. As the center circulates blood around the physique, its functions are equivalent to those of blood. The most important features of the cardiovascular system are: � oxygen and nutrient provide of the organism (transport of respiratory gases and nutrients) � thermal regulation (heat transfer in blood � defence perform (transport of immune cells and antibodies) � hormonal management (transport of hormones) � haemostasis (transport of blood platelets and coagulation factors) the heart is split right into a left and rfght half by the cardiac septum. The two halves of the guts are each subdivided by valves (atrioventricular valves) into a proper and left atrium and a right and left ventricle. Pars membranacea, whereas the biggest part consists of cardiac muscle (Pars muscularis). Within the periphery of the physique and the organs the vessels of microcirculation are related between aFteries and veins. Here blood pressure is decreased in the arterioles in order that oxygen and gasoline change can take place within the capillaries. The light margin of the guts tasks from the third to sixth costal cartilage in a line which is 2 em lateral to the right sternal border. Thellrft margin of the guts initiatives onto a connecting line between the lower rim of the three 111 rib (2-J em parasternal) and the midclavicular line on the left. Its dimension corresponds to the fist of each respective individual; the burden is on common 25o-. The heart has 4 aides: the ventrally oriented Facies stemocostalis corresponds predominantly to the proper ventricle. The caudally pointing Facies dlaphragmatlc:a is composed of elements from each ventricles. The Facies pulmonalia is shaped to the best by the right atrium and to the left predominantly by the left ventricle. Since the atria were considered for a long time as part of the upstream veins, naming the posterior side was apparently distributed with. The largest a half of the Facies sternocostalis is covered on each side by lung and pleura. These areas correspond to the Recessus costamediaatlnales of the Cavitas pleuralis. Underneath the 41h rib, the pleural edges move other than each other and confine between them the Trigonum pericardiacum, in which the pericardium lies instantly against the ventral thoracic wall. Tapping of the center lpen:ussion) may give an initial indication of the dimensions of the heart. The projection of the heart contours, which are lined by the pleura of the costomediastinal recess. When this area extends to the left over the midclavicular line, it is an indication of left ventrieuler hypertrophy. However, this measure is relatively dangerous and has therefore largely been abandoned. In most circumstances an enlargement to the left aspect (left pulmonary surface) is present, which points to damage to the left ventricle. This can be brought on by excessive blood pressura (hypertension) within the systemic circulation or a stenoel� or aortic or mltrallnaufflclancy. The epicardium develops from cells which migrate from the septum transversum and the liver primordium. Through varied lengthening of the person elements and through redistribution, the tubular heart is transformed into the S-shaped heart loop in the fourth to fifth week. The connection between atrium and ventricle is restricted to the unpaired atrioventricular canal which firstly flows into the left a half of the left ventricle. The conus arteriosus of the outflow tract is divided spirally and, together with the adjoining saccus aorticus, forms the Truncus pulmonalia and the aorta. The pulmonary arteries and the Ductus arteriosus develop from the sixth pharyngeal arch artery. Endocardial pillow -lop -bottom Oa1lum lllriowntriaare - dexlrum -einiellum Ostium atr1ovanlrlaJiara -daxlrum -U! Uara intarvanlriculara, Clinical Remarks - - - - - - - - - - - - - - - - - - - - - - - - - -. If the spira~like subdivision of the outflow tract fails to appear, the Aorta ascendens and Truncus pulmonalis move directly subsequent to each other. Thereby the aorta originates incorrectly from the best ventricle and the Truncus pulmonalis from the left ventricle(= transposition of the nice vessels). This malformation leads to the systemic and pulmonary circulations being utterly separated from each other with no oxygenated blood going into the systemic circulation and thereby reaching the organs. It is possible to survive with out these openings I these heart defects, comprising 5% of all heart defects, are nonetheless comparatively uncommon. In this illustration, the oxygen content of the blood is represented by colours: oxygenated (rad, deoxygenated (blue). Breathing inflates the lungs and pulmonary circulation is opened, so that pressure within the left atrium increases.
Discount kamagra gold expressThe varied sections of the big intestine surround the small intestine like a picture frame surrounds an image; however impotence from stress purchase kamagra gold with a visa, the size of the sections and the place of the colon flexure, and thus additionally the shape of the large intestine, are very variable. The left flexure usually extends further cranially and, as a end result of the change in the course of direction of the gut by virtually 180�, could be tough to overcome when performing enteroscopy. In addition, the Colon ascendens and Colon descendens also can lie intraperitoneally and then have their very own Mesocolon ascendens and Mesocolon descendens. The Rectum and anal canal lie in the pelvis and because of various peculiarities in topography, their construction and vessels and nerves shall be covered along with the pelvic organs in (> Chap. Of these the Taenia libera is seen, while the Mesocolon transversum is attached to the Taenia mesocolica and the Omentum majus is hooked up to the Taenia omentalis. Bulges of the peritoneal cavity typically happen right here (Recessus duodenales superior and inferior). Behind the Pars ascendens are the left kidney with its ureter, as properly as the left Vasa testicularia/ovarica. The jejunum and the ileum have a positional relationship to both kidneys and completely different sections of the large intestine and lie on the pelvis of the urinary bladder and in women, the intraperitoneal sections of the inner genitalia (womb, ovaries and fallopian tube). This classification is of clinical relevance since for both forms of haemorrhage experiences can be found on probably the most frequent causes and essentially the most meaningful diagnostic steps for clarification. Behind the Pars descendens of the duodenum, albeit separated by their different fascial systems, are the proper kidney and adrenal gland. The Pars horizontalis of the duodenum crosses the spine below the pancreatic head, the aorta and the V. The Pars horizontalis is thereby covered ventrally by the jejunum and ileum, the Colon transversum and the mesenteric root (with A. The Pars ascendens rises to the Flexura duodenojejunalis and is fixed through a peritoneal duplicature (Lig. In the transition area between the caecum and the terminal ileum, there are sometimes bulges in the peritoneal cavity (Recessus ileocaecales superior and inferior). In this space, the pendulous kind of Appendix vermiformis may are available shut proximity to the ovaries and fallopian tubes. The Colon ascendens then rises, covered by the small intestine convolute and in front of the Nn. The Colon transversum is connected by way of the Mesocolon transversum with the posterior stomach wall and by way of the Lig. From the Taenia omentalis of the Colon transversum hangs the apronshaped section of the Omentum majus and covers the small and enormous intestines. Behind the Colon transversum to the proper lies the Pars descendens of the duodenum and the pancreatic head, in the middle the small gut convolute from the jejunum and ileum, and the Flexura duodenojejunalis to the proper. Behind the left colic flexure are the pancreatic tail and, separated by their sheaths, the left kidney. Arteries of the jejunum and ileum the small intestine convolute of jejunum and ileum is equipped by the A. The vessels form a series of 3 (jejunum) to 5 arcades (ileum) in descending order of measurement alongside the gut, from which the vascular branches lengthen up to the gut wall. The innervation and supply areas correspond to the evolutionary divisions of the intestine within the foregut, midgut and hindgut and not the macroscopic divisions into the small and enormous intestines. It is subsequently simple to understand why anastomoses are found between the vessels in the space of the duodenum and the left colic flexure. At the borders in the space of the duodenum and the left colic flexure, anastomoses enable sufficient bypass circulations. Clinical remarks In the case of excessive stress within the portal vein (portal hypertension). Even complete occlusion of one of the three unpaired belly arteries (Truncus coeliacus, A. Circulatory problems of the gut are often characterised by belly ache which occurs after eating (postprandial pain). The collateral circulations by way of the rectum not solely serve to provide the large gut however on the closure of the distal aorta or the A. In the case of a tumour within the Colon descendens, throughout the context of a left-sided hemicolectomy, the Colon descendens, along with the whole A. In distinction, in a right-sided hemicolectomy for remedy of a tumour within the Colon ascendens, the intestine with the complete A. In contrast, the lymph from the duodenum is routed through the Nodi lymphoidei pancreaticoduodenales and the Nodi lymphoidei hepatici along the respective arteries either to the Nodi lymphoidei coeliaci or even the Nodi lymphoidei mesenterici superiores. In the case of a tumour in the Colon ascendens or in the Colon transversum, lymph nodes in the drainage space of the Nodi lymphoidei mesenterici superiores must be seemed for; nonetheless, for tumours within the Colon descendens, the lymph nodes in the drainage area of the inferior mesenteric lymph nodes are relevant, which, based mostly on the retroperitoneal course of the A. The parasympathetic nervous system promotes the peristaltic movement and the secretion of the glands of the intestinal mucosa. The sympathetic nervous system, then again, inhibits this operate, in addition to the circulation of the mucosa and thus nutrient absorption, however activates the muscle tissue of the ileocecal valve. The intestine is innervated by the Plexus coeliacus as nicely as the Plexus mesenterici superior and inferior (Plexus aorticus abdominalis with sympathetic ganglions). The particular person groups of lymph nodes are colored differently in accordance with their catchment areas. Section of the intestine Duodenum Innervation Sympathetic (T5�12) and parasympathetic (N. While the sympathetic neurons descend from the Plexus coeliacus to the Plexus mesentericus superior from cranial to caudal and for the Plexus mesentericus inferior also receive extra nerve fibres from the Nn. The left-sided colon sections obtain nerve fibres from the sacral parasympathetic nervous system (S2�4) where they depart as Nn. The perivascular nerve plexus then attain the respective intestinal sections (> Table 7. A blow to the abdomen can mean that visceral reflexes result in a drop in blood stress and shortness of breath. For the analysis of appendicitis, the standard modifications to the projection of pain are essential. Initially, the pain will diffuse periumbilically or within the central epigastrium as a result of the mapping of vegetative afferents to specific sections of the stomach wall could be very vague. Functions: � Central metabolic organ and nutrient storage (glycogen, fats, amino acids, vitamins, metals) � Detoxification and excretion perform � Production of bile (exocrine gland) � Production of plasma proteins (coagulation, oncotic pressure, hormones) � Formation of hormones (endocrine gland) � Immune defence � Breakdown of purple blood cells (in the event of haemolysis), as properly as formation of blood (foetal period) 322 7. The liver takes up the vitamins absorbed in the intestines, that are predominantly transported via the portal vein (glucose, amino acids, fatty acids, vitamins) or in the same way as lipids are transported as lipoproteins by way of the systemic blood circulation. The importance of the liver because the central metabolic organ is also evident from the fact that some metabolic processes. Glucose is transformed into glycogen as needed, which is how various nutritional vitamins (vitamin A, vitamin B12, folic acid) and iron and copper are saved. A extensive number of plasma proteins, such as albumin, blood coagulation components, hormones and their precursors, and complement proteins of the non-specific immune system, are synthesised from the amino acids. Cholesterol is also transformed to bile acids, which as the primary parts of bile undertake various duties. In addition to plasma proteins, there are additionally specific cell varieties in the liver.

Purchase kamagra goldThe hyoid bone has no connection to other bony constructions and is stretched between the muscles of the base of the mouth (suprahyal muscles) and the infrahyoid muscle tissue zyrtec impotence buy 100mg kamagra gold. Subdivision Trigonum submandibulare (paired) Trigonum submentale (unpaired) Trigonum caroticum (paired) Delimitation � Lower rim of the mandibula � Venter anterior and Venter posterior of the M. View from upper entrance Os hyoideum, Cornu majus Os hyoideum, Corpus Membrana thyrohyoidea Lig. Superficial layer of the cervical muscle tissue the superficial neck muscles embody the platysma and the M. Platysma the platysma is a thin, broad muscle plate located immediately underneath the skin. It originates variably with its fibres in the skin under the Clavicula in the upper chest and inserts at the lower margin of the Mandibula. There is a superb variation within the extent of individual platysmas; in rare circumstances it extends only to the neck midline or is completely missing. From a topographical viewpoint, the muscular tissues of the nape of the neck as nicely as the M. The neck muscles could be divided into a superficial, medium and deep muscle layer (> Table 10. Due to its course, the platysma tenses the pores and skin of the neck by contraction, so has an influence on facial expressions (threatening gestures). The trigger is often a congenital malformation of the muscle; nonetheless, traumatic or inflammatory processes (myositis) may result in scarring and shortening of the muscle. Muscle contraction and the associated slanted place of the pinnacle can result in facial and cranial asymmetry. It originates with a head for each muscle on the upper fringe of the Manubrium sterni (Caput sternale) and on the sternal finish of the Clavicula (Caput claviculare). The Caput sternale and the Caput claviculare be a part of together in their course right into a broad muscle belly, which rises obliquely from the chest to the head and is inserted with a powerful tendon on the Proc. Between the two sternal heads of the right and left muscular tissues, the Fossa jugularis is well visible on the surface (jugular fossa). A unilateral contraction of the muscle causes a sideways tilting of the top to ipsilateral and a rotational motion to the Middle layer of the cervical muscular tissues the middle layer of the neck muscle tissue form the suprahyoid and infrahyoid muscle tissue (> Table 10. Both muscle teams are hooked up to the hyoid bone and their interplay determines the position of Table 10. Suprahyoid muscular tissues the muscular tissues summarised by the term suprahyoid have their origins in different embryonic buildings: � the M. Immediately before its attachment to the hyoid bone it divides into 2 tendon strands and surrounds the intermediate tendon of the M. Origins Attachment Corpus and Cornu majus ossis hyoidei Function In bilateral exercise pulls the hyoid bone backwards and upwards M. The Venter anterior originates in the Fossa digastrica on the within of the Mandibula and is innervated as the superficial separation of the M. The Venter posterior originates on the Incisura mastoidea on the medial facet of the Proc. The broad muscle plates on each side unite alongside the centre line in the roughly 4�5 cm long Raphe mylohyoidea. It is a slim, paired muscle, the medial sides of that are nearly touching in their course. The muscle arises from the rectus system of the neck and hence is innervated by a branch of the Plexus cervicalis (C1). When the Mandibula is fixed, it raises the hyoid bone and assists with opening the mouth when the Os hyoideum is fastened. Infrahyoid muscular tissues the 4 flat muscle pairs of the infrahyoid muscle tissue proceed the rectus system of the trunk to cranial. All of those are within the Trigonum musculare of the Regio cervicalis anterius, and are stretched between the sternum, thyroid cartilage, hyoid bone and in their course cowl the trachea, thyroid gland and a large a part of the larynx. All the infrahyoid muscular tissues are innervated by nerve branches of the Plexus cervicalis (C1�C4), which clump to a nerve loop, the Ansa cervicalis (profunda). In conjunction with the suprahyoid muscles, the infrahyoid muscle tissue determine the place of the hyoid bone and larynx, and subsequently play an important role in swallowing and voice formation (phonation). The muscle is divided by an intermediate tendon into 2 muscle bellies, a Venter superior and a Venter inferior. The Venter inferior originates medial of the Incisura suprascapularis on the Margo superior of the shoulder blade. In its course, it runs as an upper boundary of the Trigonum omoclaviculare (Fossa supraclavicularis major) by way of the lateral triangle of the neck to the entrance and continues with its intermediate tendon immediately on the carotid sheath (Vagina carotica). The Venter superior has its origin on the intermediate tendon and runs upwards to the Corpus ossis hyoidei. At the intersection point, the intermediate tendon and the Vagina carotica merge together. As a outcome the point of intersection at the level of the cricoid cartilage can also be used as a puncture point for intravenous entry. It has its origin on the rear surface of the Manubrium sterni and runs as a lot as the Linea obliqua of the thyroid cartilage. Deep layer of the neck musculature Also included in the deep layer of the neck muscular tissues are 2 muscle teams: � the lateral, deep-running Mm. Therefore, only Ansa cervicalis continues to be used, by which is supposed the nerve loop across the V. Occasionally (in approximately one third of the population) a 4th scalene muscle (M. Through its contraction, it assists with tilting the head forwards (inclination) and stabilises the Articulatio atlantooccipitalis. A unilateral contraction leads to tilting and rotation of the top on the ipsilateral aspect. Bilateral contraction assists with the bending forwards of the cervical backbone and the pinnacle. Skills After working through this chapter, you should have the ability to: � name the various fasciae and anatomical areas of the throat space and describe their boundaries the connective tissue of the cervical fascia (Fascia cervicalis) surrounds and connects the muscle tissue, vascular, lymphatic and nervous techniques and viscera of the neck with one another. In their course, the respective fascial sheets delimit different transitional anatomical spaces from each other. These anatomical areas, full of loose connective tissue, surround the viscera and vascular, lymphatic and nervous techniques, and ensure their capability to transfer against one another. This is critical because the neck structures must follow the natural movement of the cervical backbone and the corresponding location modifications throughout swallowing with none friction. The throat space structures themselves, just like the vascular, lymphatic and nervous systems, are also surrounded by their own connective tissue sheaths. Therefore, inflammatory processes or bleeding can unfold nearly freely to the cranium base and spread out into the mediastinum. Fascia � Lamina superficialis (superficial layer) � Lamina pretrachealis (middle layer) � Lamina prevertebralis (deep layer) Enclosed/ensheathed constructions � Complete throat space (also referred to as Fascia nuchae in the nape of the neck) � M. Above the hyoid bone, the Lamina superficialis covers the Trigonum submandibulare and the Glandula submandibularis which in turn is surrounded by its own capsule (specific organ fascia). In comparability to the superficial cervical fascia, the center sheet of the cervical fascia (Lamina pretrachealis) is a a lot coarser and hence more clearly outlined construction.
Syndromes - CT scan
- Blue fingernails and lips
- Get plenty of exercise.
- Confusion or decreased alertness
- Soreness and burning pain (in some cases)
- Blood in the urine or semen
- Infections during pregnancy
- How severe it is

Buy kamagra gold amexThe epiphyseal plates join between the 14th and 25th years and in most bones up to erectile dysfunction drugs wiki generic kamagra gold 100mg on-line the twenty first 12 months of life. Joints (diarthroses) between the individual bones are current from the start of the foetal interval (from the 9th week). The ectoderm at the distal fringe of the limb buds (ectodermal marginal ridge) varieties progress elements, which attract precursors of muscle cells from the somites of the mesoderm into the torso region. By the sixth week the precursor cells in the limb methods kind the ventral and dorsal muscle plenty, from which the flexor and extensor muscle tissue later develop. Since the limb muscles develop out of precursor cells from the ventral (hypaxial) muscle system of somites, the muscle tissue of the limbs are all later innervated by the anterior branches of the spinal nerves. Pharyngeal arch muscles Eye muscular tissues Former position of the occipital somites Section airplane of b Structures of the attention muscular tissues Occipital dermomyotomes and myotomes Leg muscles Somites of the tail bud a Cervical dermomyotome Arm muscle tissue Ventrolateral trunk musculature Eye Lumbar dermomyotome C1 C2 C3 C4 C5 C6 C7 C8 T1 T2 T3 T4 T5 T6 T7 T8 T9 T11 T12 Cervical dermomyotomes and myotomes Thoracic myotomes Epaxial trunk musculature Rr. Therefore, earlier than puncture there ought to always be a guide palpation to check whether the respective vessel within the elbow nonetheless actually has a pulse and may thus be seen as an artery. Arrangement of the dermatomes at the beginning (a and d) and finish of the 5th week (b and e) as well as in adults (c and f). The muscle precursor cells for the legs originate from segments L2�S3, the motoneurons of which are correspondingly merged in the Plexus lumbosacralis. Due to the rising out of the limbs, the association of the cutaneous areas, that are innervated by a spinal wire segment additionally adjustments. Arms and legs exhibit a ventroaxial border by which the individual sensory innervated areas hardly overlap. Because of two bends the Clavicula is curved and barely S-shaped, so that ventrally the lateral half is concave and the medial half is convex. Dorsally positioned underneath at the lateral bend is the Tuberculum conoideum as a small apophysis. Also on the underside of the lateral third is a despair, the Sulcus musculi subclavii, in which the M. The Clavicula originates predominantly by membrane ossification and in the 7th week is the primary osseous skeletal factor of an embryo. Firstly, an axial artery varieties within the median airplane, from which afterward branches develop out at the distal finish. Clinical remarks Because of the uncovered place of the Clavicula and its S-shape that. In a typical fracture within the center third of the Clavicula the lateral half is dragged downwards by the weight of the arm, however the medial part, then again, is dragged upwards by the pull of the M. Corresponding to the triangle shape, a distinction is made between three sides (Margo lateralis, medialis and superior) and 3 angles (Anguli lateralis, inferior and superior). A brief neck piece, the Collum scapulae, types an appendage which protrudes in the lateral angle, into which the Cavitas glenoidalis is sunken. There are 2 small elevations on its upper and decrease edges, the Tubercula supraglenoidale and infraglenoidale as the origins for the Caput longum of the M. Spine of the Scapula (Spina scapulae) is elevated from the Facies posterior and articulates with the Clavicula with its end part, the acromion. On the Scapula there are three recesses: � Fossa subscapularis, Ventral; origin of the M. Margo superior Angulus superior Fossa supraspinata Spina scapulae Incisura scapulae Proc. Clinical remarks In distinction to injuries to the medial clavicular joint, trauma to the Articulatio acromioclavicularis (clinical: dropped shoulder) is frequent. Typically they arise through a fall onto the shoulder with an outstretched arm, usually via sports activities accidents. In addition, as a result of the relatively weakly developed saddle type of the articular surfaces of the sternoclavicular joint, mild rotational actions of the Clavicula Lig. Movement Elevation/depression Protraction/retraction 40� Range of movement 40��0��10� 25��0��25� 0� 10� around its longitudinal axis are potential. During actions within the clavicular joints the Scapula is by necessity always moved as well. Thus, the Angulus inferior may be rotated approximately 30� medially and roughly 60� laterally. This rotation capability is essential for abduction of the arm in the shoulder joint beyond 90�, which is designated as elevation. A particular state of affairs right here is the flexibility to deploy a few of these muscular tissues as auxiliary respiratory muscular tissues for respiratory assist. Therefore, these muscular tissues are also referred to as migrated (secondary) back muscular tissues. The Clavicula and Scapula are moved by the shoulder girdle muscular tissues as a unit in opposition to the abdominal wall. The 2 muscle tissue of a sling act as antagonists and thus move the Scapula in opposing instructions. During rotation of the Scapula in a lateral path (movement of the Cavitas glenoidalis cranially) the M. Both tubercles are separated by the Sulcus intertubercularis and taper out distally as the Crista tuberculi majoris and minoris. At the Collum chirurgicum distal to the 2 tubercula, fractures of the humerus are widespread. This carries both joint plates of the elbow joint, the Trochlea humeri medial/ulnar and the Capitulum humeri lateral/ radial. Above the 2 joint plates are 2 indentations that come into contact with the 2 forearm bones throughout flexion. The Fossa coronoidea for the corresponding extension of the Ulna is medial and the Fossa radialis is lateral. Dorsally the Fossa olecrani impedes extending motion via contact with the olecranon of the Ulna. Proximal to the Condylus the Epicondyli medialis and lateralis are elevated as apophyses, which taper out upwards on either side as the Cristae supraepicondylares medialis and lateralis. The surface of the Cavitas glenoidalis is, nonetheless, much smaller than that of the humeral head. A unfastened connective tissue joint lip (Labrum glenoidale) due to this fact enlarges the joint plate. The shoulder joint is the ball joint with the largest vary of motion within the human body. The wide joint capsule originates at the Labrum glenoidale and extends to the Collum anatomicum of the humerus. Below the shoulder roof there are bigger bursae: � the Bursa subacromialis on the attachment tendon of the M. Therefore, in the case of operations in the area of the shoulder joint makes an attempt ought to be made to facilitate movement of the shoulder joint as early as attainable. The massive range of motion in the shoulder joint is due to the truth that the soundness of the joint is accomplished much less by bone inhibition and ligament steering, however mainly by muscles. This noticeably will increase the range of movement of the upper extremity in comparability with actions within the shoulder joint alone (> Table 4. This movement can solely be carried out together with a rotation of the Scapula, as the shoulder roof impedes additional abduction in the shoulder joint; nonetheless, rotational movements of the Scapula begin lengthy before reaching the utmost abduction within the shoulder joint of 90�.
Kamagra gold 100 mg visaIn addition buy erectile dysfunction drugs uk discount 100 mg kamagra gold free shipping, as a result of their association with urinary retention from spinal twine compression, patients are at higher threat of urinary tract infections and pyelonephritis. Treatment Complications: Chemotherapy, radiation, radiosurgery, and radical resection can be thought-about depending on the kind and site of the tumor. Radiation, radiosurgery, and surgery risks embody paralysis, bladder incontinence, and urinary retention. Risks of chemotherapy include infection, hair loss, and gastrointestinal discomfort as nicely as a quantity of other systemic side effects depending on the medication. Symptoms Localization web site Spinal wire Comment Pain and spinal tenderness often precede neurologic deficits. Imbalance with walking happens when dorsal columns are affected May be concerned within the circumstances of intradural or intramedullary tumors. Spinal Perimedullary Fistula Epidemiology and Demographics: Most generally these are small fistulae and occur in older adults. Less generally, medium-sized fistulae may have an effect on young adults and barely big fistulae may affect kids. Disorder Description: Abnormal connection between a spinal artery and medullary vein. Symptoms often develop slowly over time but the childhood giant fistulae could present abruptly and whilst subarachnoid hemorrhage. Anterior horn cells Conus medullaris Cauda equina Specific spinal roots Symptoms Localization website Spinal twine Comments Gradual myelopathy consisting of weak spot and numbness below the extent of the lesion. Progressive urinary and fecal incontinence can also be seen the young adult form is usually situated right here and presents with paraplegia and distinguished incontinence Syndromes with combined higher and lower motor neuron deficits Conus medullaris 617 Section 1 Diagnostics Secondary Complications: Some forms are associated with vascular malformations within the skin and mind. Spondylitis Epidemiology and Demographics: Incidence is approxiDisorder Description: Spondylitis is defined as irritation of the vertebrae. Spinal Subarachnoid Hemorrhage Epidemiology and Demographics: this dysfunction is extremely rare with few cases reported within the literature. Disorder Description: Hemorrhage amassing between the arachnoid and pia mater within the spinal twine. This is generally associated to trauma or spinal procedures however can be seen in coagulopathy. Spinal aneurysms are rarely present, with or without spinal perimedullary arteriovenous fistulae. Being in the subarachnoid space, the blood irritates the spinal nerve roots rather than causing compression of the spinal twine itself. Symptoms Localization site Cervical backbone Comment Neck pain, radicular symptoms together with radiation into shoulders, decreased vary of movement Mid back pain Low back ache, radicular symptoms, hip pain, buttock ache Temporal mandibular joint pain Iritis or anterior uveitis Thoracic spine Lumbosacral spine Jaw Symptoms Localization site Cauda equina Comment If the blood collected below L1, then the cauda equina shall be compressed causing ache with numbness and weak point affecting all lumbosacral roots If the blood collects proximally, it may irritate individual nerve roots causing apparent radiculopathy Eyes Secondary Complications: Cauda equina syndrome Specific spinal roots can occur in patients with longstanding spondylitis. Urinary retention and/or incontinence, loss of bowel management, sexual dysfunction, and weak point of the lower extremities ought to elevate the potential of cauda equina syndrome. Ankylosing spondylitis and associated spondyloarthropathies: the dramatic advances in the past decade. Time developments in incidence, scientific options and cardiovascular disease in ankylosing spondylitis over 3 many years: a inhabitants based mostly research. Treatment Complications: Most cases are treated surgically with the attendant dangers of bleeding, infection, anesthesia, and harm to underlying tissue. Worse in immunocompromised, including diabetes, alcoholism, and continual obstructive pulmonary disease. Transmitted through soil or other natural material contacting the skin, or by way of inhalation. Staphylococcus aureus Epidemiology and Demographics: Ubiquitous bacterium Disorder Description: Causes a variety of neurologic that colonizes the skin of many individuals. Infective endocarditis can result in embolic strokes and mycotic aneurysm; pyomyositis, infection of the skeletal muscle, is possible. Meningitis happens in the setting of head trauma or neurosurgery (especially shunts) and infrequently because of bacteremia. Symptoms Localization site Cerebral hemispheres Mental standing and psychiatric aspects/complications Brainstem Cerebellum Cranial nerves Comment Meningitis Encephalopathy because of meningitis Meningitis Meningitis Meningitis Symptoms Localization web site Cerebral hemispheres Mental status and psychiatric aspects/complications Brainstem Cerebellum Cranial nerves Comment Meningitis Confusion, lethargy, delirium, coma Meningitis Meningitis Meningitis If an infection is due to lumbar puncture Infection related to devices and procedures Related to inflammatory state Critical sickness polyneuropathy Direct an infection Secondary Complications: Skin ulceration and secondary Conus medullaris Cauda equina Plexus Peripheral neuropathy Muscle an infection by different organisms. Treatment Complications: Treatment with itraconazole or amphotericin B (nephrotoxicity) in more severe cases, together with meningitis. The upside of bias: a case of chronic meningitis due to Sporothrix schenckii in an immunocompetent host. Secondary Complications: Lungs, spleen, joints, bones, and/or pores and skin can all be concerned. Treatment Complications: Resistant strains make polytherapy needed and, with it are more unwanted facet effects of antibiotics. The incidence in Europe is lower (10�16/100,000 population) in contrast with the United States (18� 41/100,000 population). American ethnic minorities have a better incidence (57/100,000) than whites (20/100,000). It is a condition which may have longterm penalties (after time level t2), together with neuronal dying, neuronal damage, and alteration of neuronal networks, depending on the type and duration of seizures. The commonest etiologies embody infections, brain injury and epilepsy, withdrawal or adjustments in antiepileptic medication, as well as distant symptomatic epilepsy. Autoimmune encephalitis has been lately recognized as an essential etiologic consideration. If patients fail to reply, intubation and use of continuous infusion of sedatives such as propofol, midazolam, or pentobarbital are frequently employed. Focal seizures, which may embrace refined clinical motor findings similar to facial, eyelid, or limb clonus. Findings vary with the type of seizures, seizure severity, duration, underlying etiology, and chronologic age of the patient Mental standing and psychiatric aspects/ complications Secondary Complications: Common problems embrace respiratory acidosis with or with out metabolic acidosis, hypoxia, hyperglycemia and peripheral leukocytosis, arrhythmias, cardiac troponin elevation, and ischemic electrocardiographic patterns. Rhabdomyolysis might lead to acute renal failure, myoglobinuria, transaminitis, and disseminated intravascular coagulation. Treatment Complications: Benzodiazepines may suppress degree of consciousness and respiratory drive. Barbiturates may cause prolonged sedation, hypotension, paralytic ileus, immunosuppression, propylene glycol toxicity, hepatic toxicity, pancreatic toxicity, and lingual edema. Stiff Person Syndrome (Glycine Receptor Antibody Syndrome) Epidemiology and Demographics: Age at presentation varies from 30 to 60 years, however is most incessantly seen in sufferers of their 40s. The stiffness impacts primarily the truncal muscular tissues and is accompanied by spasms that trigger postural deformities. Initially, stiffness occurs in the thoracolumbar, paraspinal, and abdominal muscle tissue. Patients have chronic pain, however stress, infections, and cold temperature could cause an acute worsening of the ache. The superimposed muscle spasms happen primarily within the proximal limb and axial musculature. The spasms are unpredictable and are extraordinarily delicate to noise and touch and emotional misery.
Buy cheap kamagra gold 100 mgClinical remarks the bite top (jaw occlusion) is of significance for the manufacture of prostheses in edentulous jaws erectile dysfunction commercial bob purchase cheap kamagra gold. In a hyper-extension of the ligaments and the joint capsule or in the case of a flat tubercle the joint heads can slip in front of the Tuberculum articulare (luxation) and thus evoke a jaw lock (the decrease jaw can not be adducted). In addition, softer food components are pulverised by the pressure of the tongue towards the exhausting palate. Structure of the tongue the tongue is divided into tongue physique (Corpus linguae) and tongue root (Radix linguae). Corpus linguae and Radix linguae are separated from each other by the Vshaped Sulcus terminalis, with the tip of the V in the center of the tongue going through the Isthmus fau cium. Development Roughly in der 4th embryonic week the event of the tongue unit begins within the 1st pharyngeal arch. First, 3 protrusions seem under the ectoderm of the Stomatodeum, 2 paired laterally, the Tu bercula lingualia lateralia, and within the center on the rear the Tuber culum impar. All 3 bulges merge with each other and later kind the anterior twothirds of the tongue. From the 2nd, third and 4th pha ryngeal arches another bulge develops behind the Tuberculum im par, the Copula, from which the tongue root emerges. Between the Tuberculum impar and the Copula the Tuber culum impar is created in the middle, its epithelium constricted as a Ductus thyroglossus, grows in the neck space into the depth and Innervation space Joint capsule lateral, dorsal, medial Joint capsule anterior Lig. The constriction point of the Ductus thyroglossus is marked by the Foramen cae cum in adults. The development of the tongue from multiple pharyngeal arches and the occipital myo tome explains the complicated innervation of the tongue. Tongue mucosa the tongue surface (Dorsum linguae) passes on the tongue margin (Margo linguae) over to the tongue decrease surface (Facies inferior linguae). The section of the dorsum of tongue in front of the Sulcus terminalis is referred to as Pars presulcalis (Pars anterior), the part behind the Sulcus terminalis as Pars postsulcalis (Pars posterior). The mucosa of the Dorsum linguae within the space of Pars presulcalis is covered with quite a lot of tongue papillae (Papillae lingualis). A distinction is made between the following constructions on the tongue floor: � Mucosa � Threadshaped papillae, Papillae filiformes � Mushroomshaped papillae, Papillae fungiformes � Leafshaped papillae, Papillae foliatae � Valate papillae, Papillae vallatae the papillae are distributed in another way over the tongue. Papillae foliatae concentrate on the sting of the tongue, Papillae vallatae (only approx. Mucosa the mucous membrane (Tunica mucosa linguae) is rough within the entrance section of the dorsum of the tongue and in entrance of the Sulcus terminalis a multilayered keratinized squamous epithelium with different levels of keratinisation. The roughness comes from nu Epiglottis Plica glossoepiglottica mediana Tonsilla lingualis; Cryptae tonsillares Foramen caecum linguae Sulcus terminalis linguae Fossulae tonsillares, Cryptae tonsillares Dorsum linguae, Pars posterior Papillae vallatae Papillae foliatae merous small, partially macroscopically seen connective tissue papillae (Papillae linguae), which are for the contact and taste sensa tion. The papillae usually form a core (primary papilla), from the opposite small secondary pupillae. The mucosa is fixed on a rough plate of connective tissue (Aponeurosis linguae), however a Tela sub mucosa is missing. Tongue papillae Papillae filiformes the threadshaped papillae (Papillae filiformes) are distributed over the entire dorsum of the tongue and are covered by a kerati nized squamous epithelium. Papillae fungiformes Mushroom papillae (Papillae fungiformes) are rare on the tongue and lie distributed between the Papillae filiformes. The Papillae fungiformes have a conical shaped connective tissue core from which superficial brief secondary papillae radiate into the ep ithelium. The Papillae fungiformes are cov ered by a multilevel keratinized squamous epithelium. There are additionally quite a few mechanoreceptors and thermal receptors and free nerve endings in the connective tissue. Thus the fungal papillae are for taste percep tion as well as thermal and mechanoreceptors. Papillae foliatae Foliate papillae (Papillae foliatae) are located on the rear aspect of the tongue and run vertically from the tongue dorsum to the bottom of Vallecula epiglottica Plica glossoepiglottica lateralis Radix linguae M. They are covered by multilayered keratinized squa mous epithelium; in their lateral folds there are taste buds. The papillary body is covered by a barely keratinised squamous epithe lium and is positioned on the extent of the tongue surface. In the epithe lium of the walls of the wall trench there are quite a few taste buds on both sides. The base of the tongue is covered by multilayered keratinised squamous epithelium and has in relation to the palatine tonsil (Tonsilla palatina) low, extensively spaced crypts. On the tongue root the unpaired Plica glossoepiglottica mediana and the paired Plicae glossoepiglotticae laterales to the epiglottis originate and limit the intervening pits (Valleculae epiglotticae). Clinical remarks Taste buds All style buds (Caliculi gustatorii) together type the taste organ (Organum gustus). The style buds are located in the epithelium of the Papillae vallatae, Papillae fungiformes and Papillae foliatae. In infants and children there are also taste buds on the laryngeal en trance and the oesophageal entrance, which slowly recede in the midst of life. The taste buds encompass onion skinlike organized sensory cells and help cells. The basal section of the sensory cells is related with the taste buds through synapses. It is assumed that the supporting cells are for the regeneration of the style cells. Via the taste buds we perceive 5 style qualities: sweet, bitter, salty, bitter and umami (hearty). Tongue inferior surface the tongue inferior floor is roofed by a easy, multilevel nonkeratinised, very skinny squamous epithelium. Especially in the case of pipe smoking, potential precancerous cells occur at the tongue base as hyperkeratoses or leucoplakias. The term glossitis contains acute and chronic diseases or modifications within the tongue floor and/or the tongue body, which may have very completely different causes,corresponding to bacterial and viral infections, fungal infestation, toxic effects (smoking, alcohol), iron deficiency, and a lot of extra. If swallowed, overseas bodies can cross to the Valleculae epiglotticae at the base of the tongue and relocate the airway by stress on the epiglottis. Tongue muscle tissue A difference is made between intrinsic (own) muscles and extrinsic muscular tissues, which originate from the skeleton. In the midline the Septum linguae divides the tongue in completely into two halves. The growth of the tongue muscles is individually simply as various because the motion options. Intrinsic muscles the intrinsic muscle tissue have their origin and attachment in the tongue (> Table 9.

Buy discount kamagra gold on lineThis consists of connective tissue that respectively types a hoop (Anuli fibrosi dexter and sinister) across the atrioventricular valves (Valvae atrioventricularesl in addition to a fibrous ring across the semilunar valves erectile dysfunction doctors augusta ga buy discount kamagra gold on-line. In addition to the lltablllaatlon of the guts valves the cardiac skeleton also se! The proper atrium and the best ventricle are separated by the tricuspid valve (Valva atrioventricularis dextral. This consists of three cusps that are hooked up via tendinous cords (Chordae tendineae) to three papilla� ry muscles (anterior. The mitral valve (Valva atrioventricularis sinistral is only composed of two cusps; correspondingly there are solely two papillary muKies (Mm. Blood is pumped through the aortic valva (Valva aortae), which consists of three semilunar valves (Valvulae semilunares). The left vantricle is opened in such a way that the two papillary muscle tissue ofthe mitral valve may be recognized. The projection of the four heart valves varieties a cross, barely shifted to the left from the median plane. The projection of the valves is of mi- nor practical importance since heart sounds and in addition heart murmurs which may arise within the area of the valves are transmitted (arrows) with the blood stream to factors of most impulse (circles), the place the center is sounded (auscultated). When sounding the center with a stethoscope (auscultation), one hears at varied points the center sounds, which result from the motion of the center: � the lint coronary heart sound is created at the beginning of the systole by ventricular contraction and recoiling of the cuspidal valves. Both narrowing (stenosis) in addition to insufficient closure (failure) of the valves may trigger mur� murs. The timing of the murmur and its localisation give info on the malfunction of the respective valves. If a murmur may be heard within the diastole above the cuspidal valve, this means a lltanoslll since the valve should be open within the filling phase. Stenoses could be either congenital or acquired (rheumatic ailments, bacterial endocarditis). Failures are usually acquired and can be brought on by heart assaults if the papillary muscles. The Nodus sinuatrialis (sinus node is roughly three x 10 mm massive and is positioned in the wall of the proper atrium subepicardially between the confluence of the V. This excitation propagation could be diverted by electrodes to the surface of the physique. If the excitation travels in the course of the electrodes on the surface of the body, a positive upsurge ensues. The Q wave outcomes from a brief downward excitation propagation within the interventricular septum. The ascending branch of the R wave is attributable to excitation propagation to the apex of the guts. Because usually no less than three limb leads are taken up, one can determine the electrical axis and thereby the traditional axis from the deflection with the largest R wave. The electrical cardiac axis is, nonetheless, not similar to the anatomical cardiac axis, because the muscle mass of the two ventricles and the electrical excitability of the tissue even have an affect. The aympllthetlc flbrea are postganglionic nerve fibres, the cell bodies (perikaryal of which are localised inside the neck ganglia of the Truncus sympathicus, and attain the Plexus cardiacus through three nerves (the Nn. The sympathetic nervous system increases coronary heart rate (posi- tiva chronotropic effect), conduction speed (positive dromotropic effect). In addition, contractile drive (positive inotropic effect) is elevated, atony is accelerated (positive lusitropic effect), and cell cohesion is enhanced (positive adhesiotropic effect). As with different organs, in which these ganglia are sometimes embedded in tile wall of the oFgans, the parasympathetic Ganglia cardiaca are normally microscopically small and therefore not visible to the bare eye in a dissection. The deep, posterior group extends into the Sinus transversus pericardii and due to this fact between the arterial vessels! This posterior group spreads caudally to the dorsal layer of the pericardium into the Sinus obliquus pericardii. The Plexus cardlacus in the centre is in its natural position (in situ) and shows the course of autonomic neurons. The neurons then comply with the branches of the cardiac vessels and unfold from there onto the surface of the heart. The parasympathetic neurons, then again, are preganglionic nerve fibres from the N. Usually (in balanced and right-dominant coronary circulation, linked in 75% of instances. In addition, additional branches on the Facies sternocostalis supply the proper atrium and ventricle. In over 80% of the instances in balanced and right-dominant circulation the dominant artery is the A. If the myocardium is collapsing, then a heart assault (myocardial infan:tion) is present. Accompanying risk components are diabetes mellitus, high blood pressure (hypertension), elevated levels of cholesterol in the blood (hypercholesterolemia) and smoking. In these cases, an inflammatory course of originates within the tunica intima of the A;J, coronariae, which is triggered by cholesterol~ontaining lipid deposits. This persistent inflammlltory course of types atherosclerotic plaques (b) which narrow the vessel lumen and into which haemorrhages can occur (c). It is necessary to notice that arteriosclerosis is often a sysbtmic diseue and impacts the entire systemic circulation, during which blood stress is high. Since the muscle wall of the proper ventricle has a lower oxygen demand than that of the left ventricle, as a result of stress situations. The remaining 25% of the venous blood reaches the atria and ventricles immediately via the transmural and andomural techniques. The higher respiratory tract consists of: � Nasal cavity (Cavitas nasi) � Pharynx the decrease respiratory tract comprises: � Larynx � Trachea � Lungs (Pulmones) the right lung (Pulmo dexter) has three lobes, the left lung (Pulmo sinister) has two. In the occasion of imminent suffocation this data may provide a well being care provider with an important time advantage! The asymmetrical place of the principle bronchi also needs to be tal<:en under consideration in Intubation: with this, a rubber hose (tubusl is insert- ad by way of the mouth up to the decrease respiratory tract in order to enable ventilation. If this tube is inserted too far, it normally goes into the steeply positioned proper primary bronchus. After making use of the tube, one should due to this fact use sounding of the lung (auscultation) to ensure the coFrect position of the tube in the tracheal 60 Projection of the Lungs Mldclav1r::ular line Mldadary line Slamalllna scapur. The proper lung has three lobes that are demarcated by the Fissura indirect and the Fissura horlzontalls. In this, the Fissura obliqua follows the fourth rib dorsa-laterally and separates the higher and decrease lobes. From the midaxillary line it then descends steeply and reaches the sixth rib within the midclavicular line. Anteriorly, the Fissura horizontalis continues the course along the fourth rib and separates upper and middle lobes. Because the center causes the mediastinum to distend to the left (Incisura cardiaca), the quantity of the left lung is smaller and its place additionally differs within the sternal and midclavicular lines from the proper lung (see table).

Cheap kamagra gold 100mg overnight deliveryCommon (>1%) embody anorexia erectile dysfunction medication covered by insurance purchase generic kamagra gold on line, behavioral adjustments, agitation, confusion, despair, hallucinations, psychosis, and seizure. Voriconazole has a unique antagonistic effect among the many azoles of visual disturbances, manifested as altered visible perception, blurred imaginative and prescient, shade imaginative and prescient adjustments, and/or photophobia. These visible disturbances might occur regardless of voriconazole serum focus. Voriconazole can be associated with hallucinations and encephalopathy, that are more common with supratherapeutic voriconazole serum concentrations (>5. Aztreonam (Azactam, Cayston) Typical Uses: gram negative infections, together with Pseudomonas aeruginosa, generally safe in sufferers with a history of beta-lactam allergy (exception: ceftazidime) Potential Neurologic or Psychiatric Medication Adverse Effects: Aztreonem is usually properly tolerated. The most Azole Antifungals Class Members: fluconazole (Diflucan), itraconazole (Sporanox), voriconazole (Vfend), posaconazole (Noxafil), isavuconazonium sulfate (Cresemba) incessantly encountered opposed events include seizure (<1%) and fever (<1%). Typical Uses: candidiasis, histoplasmosis, blastomyco- sis, aspergillosis, mucormycosis, cryptococcosis, invasive mold prophylaxis Further Reading Azactam (aztreonam) package insert. Ceftazidime/avibactam, nonetheless, may be very commonly (>10%) related to anxiety and dizziness. Pipercillin/tazobactam has been reported to generally (1�10%) cause headache, insomnia, dizziness, fever, agitation, pain, and nervousness. Potential Neurologic or Psychiatric Medication Adverse Effects: In general, the beta-lactam/beta-lactamase Further Reading Amoxicillin/clavulanate potassium. Seizures is a standard (1�10%) antagonistic impact in neonates and infants <3 months of age associated with meropenem and imipenem/cilastatin administration. Altered psychological status is a common (1�10%) antagonistic effect related to ertapenem. Although uncommon in adults (<1%), all carbapenems have been associated with seizures, with imipenem having the very best epileptogenic potential. Seizures happen most frequently in individuals with pre-existing contributing components (brain lesions, historical past of seizures or strokes, concomitant administration of medications that lower the seizure threshold, bacterial meningitis, or decreased renal function). Dose adjustment is beneficial in patients with decreased renal operate in order to keep away from medicine accumulation and increased danger of seizures. Co-administration of carbapenems with valproic acid or divalproex sodium will lead to decreased valproic acid serum concentrations and a attainable elevated threat of breakthrough seizures. Alternative antimicrobials must be thought of in a affected person whose seizures are properly managed on valproic acid or divalproex sodium. Probenecid interferes with energetic tubular secretion of carbapenems and concomitant administration can lead to elevated antibiotic concentrations. Daptomycin (Cubicin) Typical Uses: sophisticated skin and skin construction infections, bacteremia secondary to vascular access and endocarditis, septic arthritis, osteomyelitis, extreme infections due to methicillin-resistant Staphylococcus aureus and vancomycin-resistant Enterococcus cephalosporins, particularly in sufferers with renal failure. Drug therapy should be discontinued if seizure is suspected secondary to cephalosporin administration and an anticonvulsant could also be used if clinically indicated. Ceftriaxone is associated with kernicterus in neonates and ought to be prevented in this affected person inhabitants. Symptoms might embody decreased acuity, scotoma, color blindness, and visual defects. Optic neuritis is generally reversible upon discontinuation of ethambutol, though irreversible blindness has been reported. Testing of visual acuity should be carried out earlier than initiating ethambutol remedy and periodically during drug administration. Echinocandins Class Members: micafungin (Mycamine), caspofungin (Cancidas), anidulafungin (Eraxis) Typical Uses: candidemia, aspergillosis Potential Neurologic or Psychiatric Medication Adverse Effects: the opposed impact profile is comparable among agents within the echinocandin class. Very widespread adverse effects (>10%) embrace headache, insomnia, anxiety, and dizziness. Common adverse effects (1�10%) embody fatigue, rigors, melancholy, confusion, intracranial hemorrhage, delirium, and seizure. Fidaxomicin (Dificid) Typical makes use of: Clostridium difficile infections Potential Neurologic or Psychiatric Medication Adverse Effects: Due to minimal systemic absorption, fidax- Further Reading Cancidas (caspofungin) bundle insert. Fluoroquinolones Class Members: ciprofloxacin (Cipro), delafloxacin (Baxdela), gemifloxacin (Factive), levofloxacin (Levaquin), moxifloxacin (Avelox) Typical Uses: bone and joint infections, respiratory tract infections, intra-abdominal infections, urinary tract infections, acute bacterial skin and pores and skin construction infections including these caused by methicillin-resistant Staphylococcus aureus and Pseudomonas aeruginosa (delafloxacin) Ethambutol (Myambutol) an infection Typical Uses: tuberculosis, Mycobacterium avium Potential Neurologic or Psychiatric Medication Adverse Effects: Common adverse effects (1�10%) embrace confusion, disorientation, dizziness, hallucinations, 742 Antimicrobial Medications Fluoroquinolones have black field warnings for tendon rupture and myasthenia gravis. Risk of tendinitis is elevated with concomitant use of corticosteroids, advanced age, and in lung, coronary heart and kidney transplant sufferers. Exacerbation of myasthenia gravis is associated with fluoroquinolones and it is strongly recommended to keep away from their use in patients with identified historical past of myasthenia gravis. Common (1�10%) opposed results embody headache (4%), dizziness (3%), insomnia (2%), nervousness (<2%), and somnolence (<2%). Potential Neurologic or Psychiatric Medication Adverse Effects: rules and practice of infectious illnesses. Glycopeptides (Orbactiv), (Vancocin) infections Class Members: dalbavancin (Dalvance), oritavancin telavancin (Vibativ), vancomycin Typical Uses: acute bacterial skin and skin construction Potential Neurologic or Psychiatric Medication Adverse Effects: Further Reading Baxdela (delafloxacin) bundle insert. Common (1�10%) adverse results related to the glycopeptides class embrace headache and dizziness. Very frequent (>10%) antagonistic results associated with telavancin embody insomnia and psychiatric disturbances. Paresthesia and rigors have been reported as frequent (1�10%) adverse results associated with dalbavancin. Vancomycin is commonly related to ototoxicity particularly in sufferers with renal dysfunction, underlying listening to loss, and concomitant use of ototoxic brokers such as aminoglycosides. Serum trough monitoring is really helpful to reduce vancomycin-induced ototoxicity. Fosfomycin (Monurol) Typical Uses: remedy of uncomplicated urinary tract infections, specifically these caused by prone strains of Escherichia coli and Enterococcus faecalis ated with fosfomycin use is headache. Peripheral neuropathy is 743 Section 2 Medication Adverse Effects dose-related, occurs mostly in the malnourished and in these predisposed to neuritis. Concomitant pyridoxine remedy is beneficial for these with threat components for neuropathy. Common adverse results (1�10%) include convulsions, dizziness, lethargy, memory impairment, and toxic psychosis. Isoniazid carries a black field warning for hepatotoxicity, which in extreme circumstances could current with encephalopathy. The risk of hepatotoxicity is greater in patients concomitantly receiving different anti-tubercular brokers related to hepatotoxicity, similar to rifampin and pyrazinamide. Common (1�10%) clarithromycin adverse effects embrace headache, insomnia, and vertigo. Few neurologic or psychiatric adverse results have been reported for erythromycin. Metronidazole ought to be used with warning in sufferers with a history of seizure or different central nervous system disorders.
References - Toyota M, Ahuja N, Ohe-Toyota M, et al. CpG island methylator phenotype in colorectal cancer. Proc Natl Acad Sci U S A 1999;96(15):8681-8686.
- Stratford, P. W., Binkley, J. M., Riddle, D. L., & Guyatt, G. H. (1998). Sensitivity to change of the Roland-Morris Back Pain Questionnaire: Part 1.
- Ghika-Schmid F, Bogousslavsky J. The acute behavioral syndrome of anterior thalamic infarction: a prospective study of 12 cases. Ann Neurol 2000;48(2):220-7.
- Cornud F, Khoury G, Bouazza N, et al: Tumor target volume for focal therapy of prostate canceroDoes multiparametric magnetic resonance imaging allow for a reliable estimation?, J Urol 191(5):1272n1279, 2014.
- Roberts DJ, Hall RI, Kramer AH, et al: Sedation for critically ill adults with severe traumatic brain injury: a systematic review of randomized controlled trials. Crit Care Med 39:2743-2751, 2011.
|


