|
Marshall D. Kramer, MD - Associate Professor of Surgery
- New York Medical College
- Chief, Thoracic Surgery
- Our Lady of Mercy Medical Center
- Bronx, New York
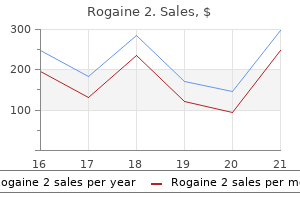
Rogaine 2 dosages: 60 ml
Rogaine 2 packs: 1 flacons, 2 flacons, 3 flacons, 4 flacons, 5 flacons, 6 flacons, 7 flacons, 8 flacons, 9 flacons, 10 flacons

Order 60 ml rogaine 2 visaIn latest years man health customer service buy rogaine 2 online, laparoscopic strategies have surpassed open nephrectomies in popularity, significantly for easy and radical procedures. Laparoscopic approaches to radical nephrectomy are even being efficiently employed within the remedy of locally invasive kidney most cancers. Laparoscopic partial nephrectomy is technically extra demanding than its open counterpart and currently entails temporary clamping of the renal hilum to optimize visibility during excision and minimize blood loss. B: Evidence of thrombus emboli in the venous filter 3555 following cardiopulmonary bypass highlights the friability of intravascular renal cell carcinoma thrombus. C: Intraoperative transesophageal echocardiography demonstrates proper atrial extension of a renal cell tumor. Laparoscopic radical nephrectomy for cancer entails smaller incisions, less blood loss, decreased postoperative analgesic requirement, shorter hospital keep and convalescent period, and comparable longterm outcomes in comparison with open radical nephrectomy. Traditional open nephrectomy is associated with a major incidence of persistent ache ranging from 5% to 26%. The perceived differences between laparoscopic and open nephrectomy procedures have influenced scientific apply, including anesthesia planning for postoperative ache management. Compared to open nephrectomy, the decreased pain and shorter recovery times have meant that epidural anesthesia is less likely to be chosen for laparoscopic approaches, with postoperative ache management for these procedures offered by a multimodal strategy involving opiates and appropriate nonopioid adjuncts. Recent small research have reported good success with continuous local anesthetic infusions by way of catheters placed in the rectus and retroperitoneal sheaths intraoperatively (across the intercostal, ilioinguinal, and iliohypogastric nerves). Benefits embrace discount of the following: pain ranges, opioid necessities, nausea, time to recovery and discharge, and price. Depending on the experience of the surgical staff, robotic procedures may also take more time. Notably, the function of robotic help is being equally explored and developed for a number of other major urologic surgical procedures. Systemic vascular resistance and cardiac output normally return to near-normal values over the 10 minutes following establishment of pneumoperitoneum. Preoperative fluid loading with further preinduction colloid boluses earlier than institution of pneumoperitoneum leads to larger stroke volume and urine output compared to standard intraoperative fluid regimens, but research are lacking relating to any evidence of improved outcome using this strategy. Following laparoscopic donor nephrectomy, some donors develop oliguria despite hemodynamic stability and liberal fluid administration strategies. Cephalad displacement of the belly contents, notably in obese sufferers, can also add atelectasis and ventilation�perfusion mismatch. Cardiac valvular dysfunction has been reported throughout laparoscopic nephrectomy,168 and cardiac ischemia can develop in at-risk sufferers with coronary artery illness. There can also be an instantaneous increase in intracranial pressure with the institution of the pneumoperitoneum. Notably, sufficient neuromuscular blockade plays a job in maintaining insufflation pressures at the lowest degree required to achieve optimum surgical publicity. Cystectomy and Other Major Bladder Surgeries Cystectomy involves elimination of all or a part of the urinary bladder. Although radical cystectomy is commonplace for many muscle-invasive malignant disease, simple cystectomy is primarily for benign bladder disease. Of the estimated 69,250 instances of bladder cancer in 2011 in the United States, roughly 90% had been expected to undergo a surgical process for his or her illness. Radical cystectomy combines bladder removal with resection of different pelvic organs and lymph nodes. As a results of removing of the whole bladder, easy and radical cystectomy procedures require a companion surgical procedure to permit for future urine assortment. Alternate choices include the so-called continent diversion reconstructive procedures, that are gaining popularity. Because diversion surgeries can make future prognosis of appendicitis troublesome, some surgeons routinely additionally perform an appendectomy as a part of urinary diversion procedures. Much like nephrectomy, each retroperitoneal and transperitoneal approaches are possible for cystectomy, and laparoscopic and robotic-assisted strategies are becoming popular for both cystectomy and diversion procedures. Preoperative Considerations the most common patients presenting for cystectomy are those with bladder cancer. Approximately 90% have transitional cell tumors, and approximately 90% of these have already invaded muscle at prognosis. Bladder tumors often current with urinary retention however are generally diagnosed by hematuria (microscopic or macroscopic) with or with out voiding signs similar to urgency, frequency, and dysuria. Prior to cystectomy, sufferers have usually undergone one or several cystoscopies for tumor biopsy or resection, and plenty of have already received radiation and chemotherapy. Men are about 4 instances more probably than women to be diagnosed with bladder cancer, with white males twice as vulnerable as African-American men. Paraneoplastic syndromes much like these seen with kidney cancer have been reported with bladder most cancers however are relatively rare. Intraoperative Considerations Anesthetic management for cystectomy is much like that for nephrectomy surgery (see earlier), including preparation for the potential for major bleeding. Although sufferers might strictly undergo cystectomy surgery with epidural anesthesia alone, this is rarely chosen due to the prolonged length of surgical procedure. Particular consideration ought to be paid to the method to assessment of intravascular volume throughout cystectomy given the appreciable potential for bleeding and hypovolemia and the absence of significant urine output data. Combining intraoperative epidural analgesia with a common anesthetic for cystectomy could cut back bleeding and improve postoperative analgesia with out in any other case affecting complication charges. Made in style by their use in colorectal surgeries, such protocols embrace a variety of evidencebased preoperative, intraoperative, and postoperative management strategies geared toward reaching early return of gastrointestinal function and good pain management, thereby minimizing the surgical stress response, decreasing end-organ dysfunction, and enhancing general recovery following main surgery. The use of such pathways has been reported to considerably reduce time to discharge and incidence of postoperative complications, with the most effective supporting evidence coming from colorectal surgical procedure outcomes. Rather than extended fasting, the affected person can consume a lightweight meal 6 hours previous to surgical procedure, a clear carbohydrate drink for preoperative hydration and glucose and insulin optimization up until 2 hours before surgery. After arrival within the preoperative area, a multimodal analgesic regimen (often involving insertion of a thoracic epidural catheter for regional analgesia and a minimal approach to systemic opioid administration) is began, along with venous thromboembolism 3560 prophylaxis using subcutaneous heparin injection. Intraoperatively, a minimally invasive surgical strategy is employed every time possible. Endorgan operate is optimized by way of a goal-directed fluid management technique involving noninvasive cardiac output monitoring. The mortality price for radical cystectomy with diversion is roughly 1%, and perioperative complications are common (27. Specific Procedures Partial Cystectomy Nonmalignant indications for partial bladder resection embody bladder endometriosis and benign tumors. Whenever partial cystectomy will suffice, the consequences of added surgical procedure and poorer quality of life associated with a urinary diversion process can be eradicated; hence the current interest in strategies to determine bladder most cancers patients for whom partial cystectomy with pelvic lymph node dissection could also be pretty a lot as good a remedy as radical cystectomy. Selective bladder-sparing protocols that use responsiveness of a tumor to chemotherapy and radiation therapy as a guide to surgical determination making seem to efficiently establish about one-third of 3561 the patients whose long-term outcome with partial cystectomy is equal to radical cystectomy, without the necessity for a diversion procedure. Radical cystectomy entails resection of the bladder and associated pelvic buildings, including pelvic lymphadenectomy of obturator and iliac nodes. In the male, the bladder is eliminated en bloc with pelvic peritoneum, prostate and seminal vesicles, ureteric remnants, and a small piece of membranous urethra. In the feminine, the uterus, ovaries, fallopian tubes, vaginal vault, and urethra are eliminated. Alternate terminology to radical cystectomy for these main procedures embody radical cystoprostatectomy in men and radical cystectomy with pelvic exenteration in girls.
Balsam Peru (Peru Balsam). Rogaine 2. - Dosing considerations for Peru Balsam.
- Are there safety concerns?
- How does Peru Balsam work?
- What is Peru Balsam?
- Cancer; intestinal worms; healing wounds, burns, leg ulcers, and bedsores; treating frostbite; and other conditions.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96483
Cheap rogaine 2 60 ml with mastercardTrue anaphylaxis is uncommon and characterized by elevated airway strain prostate cancer icd-9 order rogaine 2 60 ml fast delivery, vasodilation with systemic hypotension, and skin flushing. Increased incidence of reactions has been reported in patients sensitized to protamine from previous cardiac catheterization, hemodialysis, cardiac surgery, or exposure to impartial protamine Hagedorn insulin. This complication, which may happen in roughly 1% of sufferers, is mediated by launch of thromboxane and C5a anaphylatoxin. Because systemic hypotension is extra doubtless with speedy injection of protamine, gradual administration into a peripheral venous site is advisable. The usual causes embrace inadequate surgical hemostasis or lowered platelet depend or operate, and neither is recognized by a chronic activated coagulation time. Insufficient doses of protamine, dilution of coagulation components, thrombocytopenia, and platelet dysfunction, and rarely "heparin rebound," belong in the differential diagnosis. Blood product transfusion based on level of care testing has been proven efficient in treating nonsurgical bleeding. This is often associated with transient decreases in blood pressure, which usually reply to quantity infusion. If hypotension persists, the chest should be reopened to rule out cardiac tamponade, a kinked coronary bypass graft, or other issues. Medicated infusions must be maintained, as clinically indicated, with transportable infusion pumps. Avoidance of aortic manipulation and cross-clamping especially in aged patients is related to decrease stroke charges. The growth of retractors and stabilization gadgets allows the surgeon to function on the beating coronary heart with out inflicting arrhythmia or hypotension. Other advances embody the use of intracoronary shunts and sutureless anastomotic gadgets. Alternate incisions tutored as "minimally invasive" provide limited publicity and improve surgical difficulty. A kind of minimally invasive cardiac surgery makes use of port access expertise, with the assist of a robotic system. A interval of single-lung ventilation could also be required under capnothorax for insertion of surgical access ports. The hemodynamics are monitored constantly and speedy intervention is required in the face of fixing hemodynamics. In addition, displacement of the center could trigger falsely elevated central venous and pulmonary pressures despite the presence of hypovolemia. Direct observation of the guts and communication with the surgeon are important in managing hemodynamic swings. Pre-existing high-grade lesions might have brought on formation of collateral circulation, which may ameliorate potential ischemia. Right coronary lesions will predispose to bradycardia, atrial dysrhythmias, and heart block. For these causes, instant entry to cardiac pacing and cardioversion are essential. Left-sided coronary lesions 2741 could trigger malignant ventricular dysrhythmias and hemodynamic collapse. These embody optimizing preload prior to positioning, even handed use of inotropes and -agonists, and inserting the affected person in Trendelenburg position, which allows redistribution of intravascular quantity to assist the heart within the vertical position. Normothermia contributes to early extubation as nicely as prevention of coagulopathy. Aggressive ache control improves affected person satisfaction and contributes to early extubation. Regional techniques including thoracic epidurals and neuraxial narcotics are used with nice success, although anticoagulation is a concern in patients with central regional anesthetics. Postoperative Considerations Bring Backs Postoperative re-exploration is required in 4% to 5% of instances. The indications are persistent bleeding, cardiac tamponade, and, occasionally, unexplained 2742 poor cardiac efficiency. Surgery is usually required throughout the first 24 hours but in addition later in cases of delayed tamponade. The risk of cardiac tamponade should at all times be included in the differential prognosis of the postoperative "dwindles" as a result of the classic signs and indicators are sometimes absent. Because the encompassing (intrapericardial) stress is elevated, the distending (transmural) stress (intracavitary pressure�extracavitary pressure) is actually decreased. Peripheral vasoconstriction to protect venous return and systemic blood stress is one other compensatory mechanism. Myocardial ischemia might happen due to the tachycardia and lowered coronary perfusion pressure. Clinically, awake sufferers present with dyspnea, orthopnea, tachycardia, paradoxical pulse, and hypotension, but the intubated, sedated, and mechanically ventilated patient within the postoperative care unit following cardiac surgical procedure could have various clinical and hemodynamic presentations. In the cardiac surgical affected person the analysis of tamponade should be thought-about whenever hemodynamic deterioration or signs of low cardiac output occur. In postoperative cardiac sufferers, the pericardium is now not intact, and loculated areas of clot might compress only one chamber, inflicting isolated will increase in filling stress. The existing extracardiac compression augments the respiration-induced ventricular interdependence and affects the diastolic filling of the two ventricles in one other way. The reverse results 2743 take place throughout mechanical exhalation when the effects of constructive air flow dissipate. The chosen anesthetics medication ought to protect the compensatory mechanisms that sustain ahead flow. Drugs with vasodilator (either venous or arteriolar) or myocardial depressant properties should be averted in patients with severe hemodynamic compromise and dosages of any induction agent ought to be appropriately decreased. Ketamine, because of its sympathomimetic effects, may be helpful in preserving coronary heart fee and blood strain response. Pain Management Early awakening and extubation have brought the issue of postoperative ache administration in cardiac surgical procedure into focus. The normal apply has been intravenous opioids given as wanted followed by conversion to oral pain medicines. However, the search is on to find a perfect postoperative pain administration technique to complement the objective of early extubation and maximize patient satisfaction. In cardiac sufferers with extreme ache associated with sternal fractures because of the sternal retraction device during inner mammary harvest, epidural analgesia has been shown to be safe and efficient and leads to improved postoperative pulmonary perform. The finest method to understand the influence of a congenital defect and the way anesthetic agents will work together with this defect is to envision the trail blood should comply with to keep flow to the pulmonary arteries and aorta. Preoperative Evaluation History In infancy, coronary heart failure usually becomes manifest by way of feeding difficulties, easy fatigability, vomiting, lethargy, and labored breathing. In the older baby, coronary heart failure causes simple fatigability, shortness of breath, and dyspnea on exertion. Physical Examination the bodily examination of a kid ought to seek indicators and symptoms of poorly compensated congenital cardiac lesions.
Cheap rogaine 2 60 ml with amexThis truth led to the suggestion that sufferers sensitized to other risky anesthetics might be safely anesthetized with sevoflurane prostate cancer questions for your doctor purchase rogaine 2 online pills. Nitrous Oxide Nitrous oxide administration has not been shown to cause hepatocellular injury in the absence of hepatic hypoxemia. However, the clinical significance of those results is unclear, though extended or repeated exposure could induce a vitamin B12 deficiency. A uncommon syndrome of lactic acidosis, lipemia, rhabdomyolysis, hyperkalemia, myocardial failure, and death has been reported after extended infusions of propofol. Factors that affect hepatic clearance embrace blood circulate to the liver, the fraction of the drug unbound to plasma proteins, and intrinsic clearance. Regardless of the route of administration, medicine with high extraction ratios are significantly affected by alteration in hepatic blood move, which can occur with hemodynamic adjustments or hepatic influx clamping throughout liver resection. As is commonly the case for medicine with low extraction ratios, the elimination half-life may be extended (diazepam t1/2 = forty three hours). Studies have proven conflicting effects of cirrhosis on the metabolism of midazolam, possibly because of adjustments in protein binding. Because only the unbound drug is out there for metabolism by hepatic enzymes, the elimination could also be unaffected regardless of a discount in intrinsic hepatic clearance. However, the altered pharmacodynamic effects that happen in patients with encephalopathy incessantly result in an elevated sensitivity to sedatives and analgesics. The clearance of the meperidine metabolite normeperidine is reduced in liver illness, which may result in neurotoxicity. Remifentanil, rapidly hydrolyzed by blood and tissue esterases, is an exception among the many opioids as its elimination is unbiased of both hepatic function and the duration of infusion. The pharmacodynamic results of opioids are altered by liver disease, which argues for a dose discount in sufferers with superior illness because of the ability to precipitate or worsen encephalopathy. Most induction brokers, including ketamine, etomidate, propofol, and thiopental, are extremely lipophilic and have high extraction ratios. However, the pharmacodynamic results are more pronounced, and in some circumstances, as with dexmedetomidine and the benzodiazepines, the period of motion may be extended. Despite this, a resistance to the initial dose of neuromuscular blocker typically occurs as a end result of elevated -globulin concentrations and a rise within the volume of distribution (due to edema and/or ascites). However, their metabolite, laudanosine, is eradicated by the liver but neurotoxicity has not been reported. However, in endstage liver disease serum albumin function is quantitatively and qualitatively decreased. In a randomized trial of terlipressin with and with out concomitant albumin, a higher proportion (77%) of the group that received albumin confirmed a complete response (defined as a creatinine <1. The indications are to decompress portal hypertension within the setting of esophageal varices and/or intractable ascites. Sedation is usually used to facilitate placement, though some proceduralists choose basic anesthesia, as it limits patient movement, controls diaphragmatic excursion, and reduces the chance of aspiration. Due to coagulopathy, sufferers might require clotting elements and/or platelets before the process. Dysrhythmias can occur during catheter insertion due to stimulation of the endocardium. Providers ought to be ready for the risk of hemorrhage, which may occur in the presence of extrahepatic artery or portal vein puncture. Hepatic Resection In the late 1800s, the primary gastrectomies and cholecystectomies were carried out in Europe, however surgery on the liver was considered harmful, if not unimaginable. Another advance occurred in 1957 when segmental liver anatomy was described by Couinaud and others. Persistence, together with further advances in surgical procedure, anesthesia, and intensive care led to a reduction of mortality. Partial hepatectomy in regular, noncirrhotic livers is associated with mortality rates of 1% to 2%. Improved surgical method with avoidance of the thoracoabdominal method, which was related to high morbidity, contributes to improved outcomes. Smooth fracture of liver parenchyma accompanied by bipolar 3292 coagulation made parenchymal transection potential. Portal triad clamping is best tolerated and as effective as complete vascular occlusions. Ischemic preconditioning plus continuous clamping resulted in much less blood loss than intermittent clamping. Air embolism, a identified complication of hepatic resection, may be predicted on the idea of the necessity for a large hepatectomy (such without any consideration lobectomy) or when the tumor is close to the vena cava or includes portal vessels. The severity of the derangement correlates with the extent of the resection, peaks postoperative day 1 to 2, and takes as a lot as 5 or extra days to resolve. Some authors advise in opposition to preoperative epidural catheter placement, whereas others suggest correcting coagulation abnormalities previous to catheter elimination. Examples embrace minimally invasive liver surgical procedure, thermal ablation of hepatic tumors, 3294 and portal vein embolization to induce hypertrophy of the remnant liver. Despite this, complications are widespread after hemihepatectomy (52% of one hundred forty four patients); these include pleural effusions, biliary leakage, wound dehiscence, ascites and, intra-abdominal abscess. Postoperative Liver Dysfunction Postoperative liver dysfunction is taken into account within the presence of asymptomatic elevation of hepatic transaminases, jaundice, and/or symptoms suggestive of liver failure, such as encephalopathy. Mild elevations of liver enzymes can occur after surgical procedure, particularly higher stomach procedures. More severe elevations recommend hepatocellular damage, which may outcome from a number of causes together with hypoxemia, viral or bacterial insult, trauma, and chemical toxicity. Such elevations were more frequent after halothane than enflurane (incidence of 50% vs. Hepatic hypoxemia may result from a quantity of causes (Table 46-13) including cardiopulmonary etiologies (pneumonia, atelectasis, coronary heart failure), hypoperfusion (secondary to shock), anemia, or fever. The liver may take time to clear the bilirubin load that results from significant hemolysis. In each syndromes the absence or marked decrease of bilirubin glucuronyltransferase produces an unconjugated hyperbilirubinemia. Surgical and anesthetic problems are unusual in patients with Gilbert and Crigler� Najjar syndromes. If over 50% of bilirubin is conjugated cholestasis, hepatocellular dysfunction is likely. Hypoxemia, poisonous reactions, unsuspected pre-existing liver disease, trauma, and congenital issues ought to be thought of (Table 46-14). Dubin�Johnson and Rotor syndromes are congenital disorders related to a defect in bilirubin excretion, which causes a conjugated bilirubinemia. The nature and web site of the surgical process is an important threat factor for postoperative liver failure. In a collection of 747 hepatic resections, sufferers with obstructive jaundice as a end result of malignancy had a better postoperative mortality (21%) than those with cirrhosis (8. Cardiopulmonary bypass exacerbates pre-existing hepatic illness by unknown mechanisms.
Purchase 60 ml rogaine 2 overnight deliveryCarbon dioxide monitoring throughout laparoscopic-assisted bariatric surgery in severely obese sufferers: transcutaneous versus end-tidal strategies prostate cancer usually occurs because of exposure to order rogaine 2 mastercard. A comparability of complete intravenous anaesthesia utilizing propofol with sevoflurane or desflurane in ambulatory surgery: systematic review and meta-analysis. Total intravenous anesthesia with propofol reduces postoperative nausea and vomiting in patients undergoing robot-assisted laparoscopic radical prostatectomy: a prospective randomized trial. High-dose remifentanil suppresses stress response related to pneumoperitoneum throughout laparoscopic colectomy. Meta-analysis of intravenous lidocaine and postoperative recovery after belly surgery. Impact of intravenous lidocaine infusion on postoperative analgesia and recovery from surgery: a scientific evaluate of randomized controlled trials. Perioperative intravenous lidocaine infusion for postoperative pain control: a meta-analysis of randomized controlled trials. A procedure-specific systematic review and consensus suggestions for postoperative analgesia following laparoscopic cholecystectomy. Local anesthetic infiltration for postoperative pain reduction after laparoscopy: a qualitative and quantitative systematic review of intraperitoneal, port-site infiltration and mesosalpinx block. Local anaesthesia for pain aid after laparoscopic cholecystectomy�a systematic evaluate. Wound infiltration with local anaesthetic brokers for laparoscopic cholecystectomy. Intraperitoneal local anaesthetic instillation versus no intraperitoneal local anaesthetic instillation for laparoscopic cholecystectomy. Intraperitoneal use of native anesthetic in laparoscopic cholecystectomy: systematic review and meta-analysis of randomized managed trials. Systematic evaluate and metaanalysis of intraperitoneal native anaesthetic for pain discount after laparoscopic gastric procedures. Surgical space circumstances throughout low-pressure laparoscopic cholecystectomy with deep versus reasonable neuromuscular blockade: a randomized clinical study. Deep neuromuscular block reduces intra-abdominal strain requirements during laparoscopic cholecystectomy: a prospective observational examine. Respiratory and haemodynamic results of volume-controlled vs pressure-controlled ventilation during laparoscopy: a cross-over study with echocardiographic assessment. End-tidal carbon dioxide pressure during laparoscopic cholecystectomy: correlation with the baseline worth prior to carbon dioxide insufflation. Inert gas change throughout pneumoperitoneum at incremental values of optimistic end-expiratory stress. Mechanical ventilation with positive end-expiratory stress preserves arterial oxygenation during extended pneumoperitoneum. Positive end-expiratory pressure improves arterial oxygenation throughout prolonged pneumoperitoneum. Intraoperative recruitment maneuver reverses detrimental pneumoperitoneum-induced respiratory effects in wholesome weight and overweight patients present process laparoscopy. Effects of the beach chair place, positive end-expiratory stress, and pneumoperitoneum on respiratory operate in morbidly overweight sufferers throughout anesthesia and paralysis. Effect of intraoperative excessive impressed oxygen fraction on surgical website infection, postoperative nausea and vomiting, and pulmonary function: systematic review and meta-analysis of randomized controlled trials. Severe local hypothermia from laparoscopic gasoline evaporative jet cooling: a mechanism to clarify clinical observations. Anesthesia concerns for roboticassisted laparoscopic prostatectomy: a review of 1,500 cases. Effect of the amount of fluids administered on intraoperative oliguria in laparoscopic bariatric surgical procedure: a randomized controlled trial. Effects of laparoscopic pneumoperitoneum and adjustments in place on arterial pulse pressure wave-form: comparison between morbidly overweight and normal-weight sufferers. Early complication rates in a single-surgeon series of 2500 robotic-assisted radical prostatectomies: report making use of a standardized grading system. An unbiased prospective report of perioperative problems of robot-assisted laparoscopic radical prostatectomy. Cost effectiveness of routine type and display testing before laparoscopic cholecystectomy. Bradycardia as an early warning sign for cardiac arrest throughout routine laparoscopic surgical procedure. Subcutaneous emphysema, pneumomediastinum and bilateral pneumothoraces after laparoscopic pyeloplasty. Risk elements for hypercarbia, subcutaneous emphysema, pneumothorax, and pneumomediastinum throughout laparoscopy. Pneumothorax during laparoscopic fundoplication: prognosis and treatment with optimistic end-expiratory pressure. Surgical pressure pneumothorax throughout laparoscopic repair of massive hiatus hernia: a unique state of affairs requiring completely different management. Spontaneous resolution of huge laparoscopy-associated pneumothorax: the case of the bulging diaphragm and review of the literature. Rapid decision of carbon dioxide pneumothorax (capno-thorax) resulting from diaphragmatic harm during laparoscopic nephrectomy. Gas embolism during laparoscopy: a report of seven instances in sufferers with earlier belly surgical history. Incidence of venous fuel embolism throughout roboticassisted laparoscopic radical prostatectomy is decrease than that during radical retropubic prostatectomy. Gas embolism during laparoscopic liver resection in a pig mannequin: frequency and severity. Venous carbon dioxide embolism in pigs: an evaluation of end-tidal carbon dioxide, transesophageal echocardiography, pulmonary artery pressure, and precordial auscultation as monitoring modalities. Respiratory failure after laparoscopic cholecystectomy in a patient with continual hemidiaphragm paralysis. Coagulation status and the presence of postoperative deep vein thrombosis in sufferers undergoing laparoscopic cholecystectomy. Pulmonary embolism and deep venous thrombosis following laparoscopic cholecystectomy. Thromboembolic issues in three,544 sufferers present process radical prostatectomy with or with out lymph node dissection. Single-dose intravenous paracetamol or propacetamol for prevention or therapy of postoperative pain: a scientific evaluate and meta-analysis. Paracetamol and selective and non-selective non-steroidal anti-inflammatory medication for the reduction in morphine-related sideeffects after major surgical procedure: a systematic evaluate.
Generic 60 ml rogaine 2 fast deliveryThe opioid-dependent patient has increased opioid requirements androgen hormone in menopause buy rogaine 2 60ml on line, which are reported to be 30% to 100 percent greater than an opioid-naive patient154; therefore, through the preinduction interval, the dose of fentanyl, morphine, or hydromorphone must be increased accordingly. Patients prescribed transdermal fentanyl patches are often instructed to preserve their fentanyl patch into the operating room and this will serve as their baseline opioid requirement. Occasionally, nonetheless, in the case of main surgical procedure, in which the risk of main blood loss or sepsis is critical, sufferers could additionally be instructed to discontinue their transdermal patch, and an intravenous fentanyl infusion could be initiated to 3996 maintain enough plasma concentrations. Patients maintained on methadone should proceed their baseline dose all through the perioperative period. In the United States, methadone is out there for both oral and intravenous administration. It is due to this fact recommended that a baseline electrocardiogram be obtained for comparability. Both gabapentin and pregabalin bind to the -2 subunit of voltage-gated P/Q-type calcium channels in the dorsal horn of the spinal wire and, by 3998 modulating the discharge of excitatory neurotransmitters from activated nociceptors, these drugs are believed to inhibit ache transmission and central sensitization. The really helpful dose of celecoxib that reduces both postoperative ache and reduces opioid requirement is four hundred mg orally 2 hours previous to surgery. The drug could additionally be administered orally or intravenously; nevertheless, the intravenous route provides the advantage of earlier and better peak plasma levels compared to oral acetaminophen, leading to superior cerebrospinal fluid levels. The recommended adult dose in patients above 50 kg is 1,000 mg intravenously q 6 hours. The first dose could additionally be administered simply prior to surgery and continued postoperatively for so long as the patient is non per os (npo). Intraoperative administration of the opioid-dependent patient requires the prudent use of fentanyl, morphine, or hydromorphone so as to provide efficient intraoperative anesthesia, postoperative analgesia, and to stop 3999 opioid withdrawal. Because of receptor downregulation an alternative opioid could additionally be helpful on this setting. Opioid rotation takes advantage of the reality that the new opioid will bind a special opioid receptor subtype and be metabolized in one other way. Following the cancer ache mannequin, the dose of the new opioid is lower than 50% of the calculated equianalgesic dose because of incomplete cross-tolerance. The optimal intraoperative dose of opioid varies significantly from patient to affected person; subsequently, monitoring intraoperative important signs such as heart price, pupil measurement, and respiratory rate could be helpful and allows the clinician to avoid the negative penalties of overdosing or underdosing the patient with opioid. Reversing neuromuscular blockade toward the end of a common anesthetic and permitting the affected person to breathe spontaneously is normally a prudent approach. Patients with a respiratory price greater than 20 breaths per minute and significantly dilated pupils require additional opioid. Titrating fentanyl, morphine, or hydromorphone to a respiratory rate of 12 to 14 breaths per minute and a reasonably miotic pupil is beneficial. It is unclear at this time, 4000 nevertheless, what function, if any, this drug class would have specifically within the perioperative administration of the opioid-tolerant affected person, however they may be significantly valuable in the remedy of the opioid-tolerant affected person as a outcome of they attenuate opioid withdrawal symptoms and can cut back postoperative opioid requirements and ache. Ideally, the optimal amount of opioid has been administered to the patient through the intraoperative period, permitting them to emerge from anesthesia comfortably sedated and pain-free. For example, a affected person taking ninety mg of oral morphine per day equates to 30 mg of intravenous morphine per day, which can be administered as a basal morphine in fusion of 1. Patients recovering from 4001 same-day surgical procedure will be initially treated with intravenous doses of opioids in the recovery room; nonetheless, they are often quickly transitioned to an oral routine consisting of their baseline opioid requirement plus an acceptable amount of short-acting opioid for breakthrough ache consistent with the invasiveness of the surgery. Nonopioid coanalgesics are opioid-sparing and ought to be part and parcel of any multimodal perioperative ache administration technique within the opioiddependent patient. In a single case report, nonetheless, which concerned an opioid-dependent trauma affected person, ketamine was administered, postoperatively, at a starting dose of 10 g/kg/min after which progressively tapered to 2. The administration of dexmedetomidine may be significantly helpful in the perioperative pain management of those sufferers. The proof means that it would be prudent to administer a gabapentinoid postoperatively for 10 to 14 days. Although both gabapentin and pregabalin are indicated, pregabalin is the popular drug due to its superior pharmacokinetic profile. Peripheral nerve blockade as a single-injection approach or as a continuous catheter can be very helpful. Likewise, if indicated, epidural analgesia ought to be part and parcel of the multimodal pain regimen for these patients. During the perioperative period, however, the epidural and systemic requirements for morphine have been reported to improve three to fourfold. Epidural infusions which have been beneficial embrace a mix of fentanyl (2 to 5 g/mL), morphine (0. Notwithstanding the truth that sufferers acquire wonderful analgesia from the epidural, opioid serum levels and supraspinal receptor binding may not be completely sufficient at preventing opioid withdrawal symptoms. A doctor properly versed in chronic pain management and comfortable within the equianalgesic dosing of opioids through totally different routes of administration should ideally be involved in the care of the affected person. Careful monitoring of the patient for extreme sedation or respiratory despair is mandatory, and caregivers in the restoration room and on the postsurgical items must be alerted to the potential threat for respiratory despair when parenteral and neuraxial opioids are mixed. Organization of Perioperative Pain Management Services There is a growing recognition in the health-care trade that the undertreatment of ache is a widespread downside that cuts throughout all phases of patient care. The effective management of pain is a crucial component of good perioperative care and restoration from surgical procedure. Unrelieved pain and inadequate pain reduction have detrimental physiologic and psychological results on sufferers by slowing recovery and creating burdens for sufferers and their households, and by increasing prices to the health-care system. Although the acute postoperative pain service performs an integral function within the ache administration of the surgical patients, there are considerable barriers that challenge the institution and/or effectiveness of acute pain groups in managing patients across the continuum of care. There is nice evidence that the general incidence of moderate-to-severe pain in surgical sufferers is about 25% to 40% regardless of the availability of pain remedy. The value of an acute pain service, apart from its benefit for affected person care, also comes from the added worth of reducing hospital prices by enhancing surgical consequence and by facilitating patient recovery and early discharge. The success of a perioperative ache administration team can be established not solely within the context of the direct patient care that the team provides but in addition via its 4003 function in educating different health-care professionals and companies as doctor leaders answerable for setting medical requirements and apply tips within the health-care system. The group have to be constructed around a physician chief with training and experience in pain medicine. The institution should help the service, which may be manifest through support of a nurse coordinator or the supply of a pharmacist to consult on the many pharmaceutical points that arise in sufferers on preoperative medications that may conflict with the perioperative pain management plan. The perioperative ache administration chief is liable for the development and implementation of scientific pathways and protocols that successfully enhance restoration following surgical procedure. These protocols should embrace ache evaluation tools that are adopted across the continuum of care by all caregivers. Acute postsurgical ache can also be caused by extended affected person positioning or stress results from extended immobility. Many patients presenting for elective surgical procedure may also endure chronic pain from underlying illness or damage. Other common patient limitations include cultural and language limitations, stoicism and/or opiophobia, and private experience or the experiences of associates and family members. In developing a perioperative pain service it is important to keep in mind that the importance of effective perioperative ache administration extends well past the mere institution of dedicated personnel; it should additionally embody a management role in transforming the institutional culture to elevate the relief of ache and suffering to its place as a major aim of patient care.
Purchase rogaine 2 60ml fast deliveryAll have been tracheally extubated in the operating room mens health quiz questions purchase 60ml rogaine 2 amex, and none required intubation for postoperative respiratory despair. They commented that the shift away from use of muscle relaxants provided optimum operating condition and improved affected person comfort. Politis and Tobias217 describe rapid-sequence intubation in a myasthenic affected person with a full abdomen using propofol, lidocaine, and remifentanil. Although the trachea was extubated 10 minutes after discontinuation of remifentanil, the patient was unresponsive to verbal stimuli and remained somnolent for 12 hours. Because the affected person had been receiving pyridostigmine for the months previous to surgery, they counsel that the delayed arousal might have been the results of potential inhibition by pyridostigmine of the nonspecific esterases that normally hydrolyze remifentanil. The patient was steady firstly of surgical procedure however grew to become asystolic on sternal retraction and obtained open cardiac therapeutic massage. Resuscitation was profitable, the dexmedetomidine infusion was discontinued, and surgical procedure was completed uneventfully. Several components may have contributed to the asystolic arrest, together with a centrally mediated enhance in parasympathetic exercise ensuing from dexmedetomidine in a patient who was also being treated with pyridostigmine, which also increases vagal tone. Thus, pyridostigmine may have interacted with dexmedetomidine in an additive or synergistic manner. Such medicine embody antiarrhythmics (quinidine, procainamide, calcium-channel blockers), diuretics (by inflicting hypokalemia), nitrogen mustards, quinine, and aminoglycoside antibiotics. Extubation of the trachea must be carried out when the patients are responsive and capable of generate adverse inspiratory pressures of higher than -20 cm H2O. Cases of gentle respiratory despair could also be treatable with parenteral 2646 anticholinesterase; extra severe instances may require reintubation of the trachea and mechanical air flow of the lungs. In the quick postoperative interval, postthymectomy patients usually show a marked enchancment in their condition and a decreased want for anticholinesterase therapy. Postoperative Respiratory Failure Myasthenic patients are at increased threat for growth of postoperative respiratory failure. A research of sufferers undergoing transsternal thymectomy suggested that the necessity for postoperative mechanical air flow correlated finest with preoperative maximum static expiratory pressure. It was concluded that expiratory weak spot, by reducing cough efficacy and skill to clear secretions, was the principle predictive determinant. Adequate clearance of secretions is essential in these sufferers and may sometimes necessitate bronchoscopy. In basic, the postoperative morbidity in phrases of respiratory failure is lower after transcervical quite than transsternal thymectomy. If the anticipated duration of the surgical process is 1 to 2 hours, preoperative oral anticholinesterase therapy may be of worth because the peak effect of the drug coincides with the conclusion of the surgical procedure and attempts at tracheal extubation. The analgesic impact of morphine and other opioid analgesics has been reported to be increased by anticholinesterases, which has led to the advice that the dose of opioid analgesics be decreased by one-third in sufferers receiving anticholinesterase remedy. Combined epidural�general anesthesia has been reported to provide excellent intraoperative and postoperative circumstances for each surgeon and affected person. The defect on this condition is prejunctional, is associated with diminished release of acetylcholine from nerve terminals, and improved by brokers such as 4aminopyridine,228 guanidine, and germine that increase repetitive firing. Affected sufferers are notably delicate to the consequences of all muscle relaxants, which must be used with nice warning or prevented entirely. Adequate postoperative ache control is important to ensure a good respiratory 2648 effort. The administration of adequate opioid to treat ache adequately may trigger sedation and respiratory melancholy. There are different intravenous drugs that can be utilized for pain management along with opioids. The intercostal blocks may be performed internally or externally earlier than or after surgery utilizing a standard technique. However, the best method throughout thoracic surgical procedure is to have the surgeon carry out the blocks underneath direct vision from contained in the thorax whereas the chest is open. This provides 6 to 24 hours of average pain relief, however patients nonetheless complain of diaphragmatic and shoulder discomfort caused by the chest tubes. The intraoperative placement of catheters in intercostal grooves permits for a continuous postoperative intercostal nerve block. Placement of a catheter in the paravertebral area allows for 2649 blockade of a number of levels of intercostal nerves. This method has been reported to present good analgesia, and with fewer unwanted side effects than epidural analgesia. These are significant advantages over systemic opioids or infiltration of native anesthetics. Epidural opioids are handiest at alleviating pain when administered on the thoracic stage. Epidural morphine has been proven to decrease ache and enhance respiratory perform in postthoracotomy patients. There may be a discount in each morbidity and mortality with epidural or spinal analgesia. Subarachnoid (intrathecal) morphine, in a dose of 10 to 12 g/kg, has been efficiently used after thoracic surgical procedure. When morphine is given intrathecally before the induction of anesthesia, a lower in the dose of anesthetic medication required could happen. The administration of analgesic agents earlier than surgical procedure is termed preemptive analgesia and should stop these neuroplastic changes, thereby reducing postoperative pain. The injection of local anesthetic between the pleural layers can block multiple intercostal nerves and/or ache fibers traveling with the thoracic sympathetic chain. The surgeon can even place in the wound a soaker catheter, by way of which native anesthetics could be administered postoperatively. The pain that happens could also be associated to trauma to intercostal nerves by insertion of the surgical trocars or by compression in the course of the surgical procedure. In addition, an incision shall be required to extract a lobe within the case of a lobectomy, which can exacerbate ache additional. If the preoperative lung operate is poor, such that the patient could have problem respiration adequately postoperatively or might not tolerate systemic opioids, it additionally could also be extra prudent to place an epidural for that scenario also. The administration of native anesthetic via the chest tubes is one other approach which might successfully treat postoperative pain. There is a discount in respiratory complications with epidural analgesia including atelectasis and pneumonia. It happens extra commonly in the basal lobes than in the middle or higher lung regions. Such a respiratory sample produces small airway closure and obstruction with inspissated secretions, ensuing finally in alveolar air resorption and terminal airway collapse. Other sources of atelectasis include mucus plugging, which may obstruct a lobe or even a whole lung, and incomplete re-expansion of the remaining lung tissue after one-lung anesthesia. The diagnosis of atelectasis could be made by medical findings, chest radiography, or arterial blood gasoline analysis. The latter can be increased by an increase in transpulmonary strain (difference between airway stress and interpleural pressure) or in lung compliance. The tracheas of many sufferers could be extubated shortly after thoracic surgical procedures.
Syndromes - Head CT or head MRI scan
- The cause of scoliosis
- Oral cancer
- If your blood pressure is above 135/80, your health care provider will test your blood sugar levels for diabetes.
- Diarrhea
- Keep your blood pressure under control
- Eating poisonous mushrooms or other poisons
- Pneumothorax
- Wheat germ and wheat germ oil
Order cheap rogaine 2 on lineCentral venous catheterization is mostly employed for monitoring quantity developments and for the dependable delivery of vasoactive treatment androgen hormone klotho buy 60ml rogaine 2 free shipping. Cardiac operate is commonly assessed with either a pulmonary artery catheter or transesophageal echocardiography. Either technique can present priceless details about cardiac functioning and volume status. Echocardiography is essentially the most delicate marker for brand spanking new regional wall movement abnormalities and direct visualization of applicable ventricular filling. Pulmonary artery catheterization can be helpful each intraoperatively and postoperatively to information resuscitation. The use of pulmonary artery catheters has been the subject of debate, with conflicting proof as to their benefit in high-risk surgical sufferers. As with any monitor, the knowledge obtained is simply pretty a lot as good as the clinician interpreting and intervening upon the info. Virtually all anesthetic medicine and techniques have been described for aortic reconstructive surgical procedure. The capability to maintain hemodynamic equilibrium and attend to detail is much more important than is the choice of drug. Volatile agents could enhance preconditioning mechanisms ought to myocardial ischemia occur. The upkeep anesthetic is designed to preserve hemodynamics within 20% of the baseline vary. An array of short-acting vasoactive agents (including vasodilators, vasopressors, and inotropes) ought to be available to immediately deal with hemodynamic lability. Alternatively, deepening the anesthetic or injection of the epidural catheter with local anesthetic will increase vasodilation, though each of those approaches require cautious attention to avoid unintended hypotension. After the vascular clamps are positioned and the aneurysm sac is incised, blood loss is swift from any vessels arising from the aorta between the 2 clamps. Blood loss could be considerable without the onset of hypotension or tachycardia because a good portion of the vascular tree is excluded from circulation throughout aortic occlusion. An autotransfusion device must be employed to scale back the quantity of autologous blood needed. It is prudent to quantity load in the course of the period of aortic cross-clamping in anticipation for the vasoplegic washout and reactive hyperemia that may occur with the removal of aortic cross-clamp. Immediately previous to the removal of the aortic clamp, vasodilating agents are discontinued. Ongoing fluid resuscitation and vasopressor and inotropic support is frequently needed. Severe refractory hypotension could be temporarily abated with reapplication of the aortic cross-clamp until acceptable measures can be instituted. Over the course of the reconstruction, there could additionally be frequent situations of cross-clamp utility and release to limit the ischemic time to important organs and to "check" the anastomoses. It is imperative for the anesthesiologist to be versatile and adaptable, and to have a variety of short-acting vasoactive agents out there for hemodynamic manipulation. Each time the cross-clamp is eliminated, a "washout" of vasoactive brokers happens with the potential for hemodynamic instability. Central and pulmonary filling pressures may be elevated regardless of systemic hypotension due to the washout of lactic acid and different inflammatory mediators, which results in pulmonary vasoconstriction and cardiac stunning. Reinstitution of the epidural catheter allows for sufficient pain management and should assist with weaning from mechanical air flow, particularly in those with concomitant persistent obstructive pulmonary disease. For those sufferers who stay intubated, the utilization of the epidural catheter for pain control permits a reasonably mild intravenous sedation, which permits for continued monitoring of neurologic standing. Aggressive administration of danger elements with pharmacologic, train, and lifestyle modification prevents illness development in the vast majority of cases. Decision making should contemplate response to remedy, lack of operate, and effect on high quality of life. Risk factors for accelerated illness progression embrace age, diabetes, smoking, and hyperlipidemia. It is estimated that inside 1 12 months, 25% of patients will progress to amputation, and a further 25% will die from cardiovascular causes. These sufferers, then, are at elevated perioperative risk as a outcome of both medical and surgical factors associated to illness severity. Direct reconstruction has higher long-term patency charges (greater than 80%), at the expense of higher perioperative morbidity and mortality. Extra-anatomic bypass, though less morbid, has additionally proven less durable, with 5-year patency rates are reported between 55% and 80%. Open revascularization of infrainguinal illness is dependent upon the level of the lesion(s), and should contain the femoral, popliteal, or infrapopliteal vessels. Barring contraindication, a preinduction epidural catheter ought to be thought-about for postoperative ache management. Hemodynamics are most likely to be more secure both as a end result of clamp location (typically, distal aortic) in addition to the 2810 probability of extensive collateralization related to continual atherosclerotic obstruction. This stands in stark distinction to aneurysmal disease, which has limited preexisting collateral flow. Central venous entry is cheap to ensure reliable supply of needed vasoactive drugs. Additional cardiac monitoring, corresponding to pulmonary artery catheter placement or transesophageal echocardiography, may be thought of depending on patient and surgical components. Typically, extra-anatomic bypass is undertaken from the axillary artery to the ipsilateral femoral artery, +/- subsequent femoral to femoral artery bypass. Typically, less hemodynamic lability is noted with axillary and femoral artery cross-clamping than with aortic cross-clamping. Arterial line placement must be contralateral to the surgical bypass, as arterial crossclamp placement will render an ipsilateral arterial line nonfunctional. The extra-anatomic bypass have to be tunneled subcutaneously within the mid-axillary line to forestall kinking of the graft, which can be more sympathetically stimulating than cross-clamp placement. Close consideration should be paid to forestall untoward hemodynamic swings or affected person motion during this era. The selection of anesthetic approach for infrainguinal revascularization is individualized for each patient. Lower extremity revascularization can be carried out underneath basic, neuraxial, or regional anesthesia. Purported benefits of regional anesthesia embody avoidance of hyperdynamic responses to tracheal intubation and extubation, blunted perioperative catecholamine response, improved vascular blood flow, larger graft patency rates, and lower pulmonary complications. Morbidity and mortality following decrease extremity revascularization is usually cardiac in origin. Endovascular Surgery the appearance of the endovascular period has revolutionized the sector of vascular surgical procedure. Endovascular procedures are minimally invasive and are generally associated with decreased perioperative mortality and major morbidity, shorter hospital and intensive care stays, and faster return to baseline function, notably for the elderly or frail. In addition to a decrease degree of surgical stress, endovascular techniques may obviate the necessity for common anesthesia. In addition, endovascular repairs have proven less sturdy and more vulnerable to reintervention than conventional open repairs.

Buy rogaine 2 cheapThe most amplitude is the widest portion of the curve and signifies the absolute power of the fibrin clot balance androgen hormones naturally rogaine 2 60ml sale. The -angle is the slope of the exterior divergence of the tracing from the R-value level, indicating the pace of clot formation and fibrin crosslinking. The value of this parameter is set by each coagulation elements and platelets. Hypothermia can cause coagulopathy by interfering with each platelets and coagulation components. Results of coagulation parameters are obtained inside 10 to quarter-hour due to activation with specific supplies for each of clotting, platelet, and fibrinogen operate. The various contribution of these conditions to the scientific image of a given patient necessitates priority-oriented planning. If a rapid-sequence induction is contemplated, ketamine and etomidate may confer benefits over propofol. In equipotent doses in normovolemic patients, they produce much less cardiovascular depression. Contrary to findings of increased mortality with prolonged etomidate infusion, a single induction dose (0. Its longer length of motion may be disadvantageous and should result in hypoxia, if each air flow and intubation show to be impossible. Under these circumstances, one of the obtainable videolaryngoscopes or other aids could be employed to overcome the problem. Sugammadex can also be utilized to encapsulate rocuronium or vecuronium and get well spontaneous inhaling a reasonably quick interval. Bradycardia, dysrhythmias, and cardiac arrest might happen after succinylcholine within the presence of hypoxia and hypercarbia. Some of those issues may also follow an apparently uneventful intubation carried out with out succinylcholine. Hypovolemia In the absence of managed human research of anesthetic drug results in hemorrhage and hemorrhagic shock, our current knowledge on this space is based on the results of experimental work, mostly in swine, and clinical 3807 experience from managing trauma victims. Our planning course of for deciding tips on how to use anesthetic brokers is additional complicated by the damage control resuscitation precept, specifically permissive hypotension. The information that should drive decision making on this regard are as follows: First, anesthetic agents not only have direct cardiovascular depressant effects but also inhibit compensatory hemodynamic mechanisms similar to central catecholamine output and baroreflex (neuroregulatory) mechanisms, which keep systemic stress in hypovolemia. Second, hemorrhage and hypovolemia alter the pharmacokinetics and pharmacodynamics of almost all anesthetic agents and often lead to a better than regular blood focus of intravenous agents and elevated sensitivity of the brain and coronary heart. Preferential distribution of the cardiac output to the brain and the heart, cerebral hypoxia, dilutional hypoproteinemia producing a larger free fraction of intravenous medication, and acidosis all seem to be answerable for these effects. Third, hemorrhage and hypovolemia have totally different hemodynamic results in the absence and presence of trauma. In the presence of trauma ache and a catecholamine surge, keep blood stress regardless of significant intravascular quantity depletion and ischemia of important organs such as the mind and the center. Based on this knowledge, lowering or eliminating anesthesia to avoid abolishing the hemodynamic steadiness is a pure and infrequently utilized practice, particularly when permissive hypotension to limit bleeding is used. Dutton252 lately instructed that correct administration under these circumstances could also be aggressive titrated administration of anesthetics and of blood merchandise to produce a high-flow and low-pressure hemodynamic state with vasodilation to improve organ flow and oxygenation, which can cut back fibrinolytic activity and inflammation. Further research is needed to help the clinician in selection of both of the approaches. The pharmacokinetic and pharmacodynamic responses of intravenous brokers to experimental hemorrhagic shock vary depending on the severity of the hemorrhage, the particular agent, and whether the impact analyzed is hypnosis or immobility to noxious stimuli. For example, in swine with compensated hemorrhage, when administered as a steady infusion, blood propofol focus increased by less than 20%, while during uncompensated shock. It is possible that hydrolysis by tissue esterases is extra intense than by their blood counterparts as a end result of the decreased tissue blood circulate in uncompensated shock is prepared to produce a 3808 main discount in remifentanil metabolism. Another instance is that hemorrhage has an identical potentiating impact on the production of hypnosis and immobility by propofol. Although etomidate pharmacodynamics are unchanged,257 a significant increase within the sensitivity of the brain and coronary heart to propofol is famous in animals, even after fluid resuscitation. As to the opioids, the calculated dose for fentanyl and remifentanil is approximately one-half that for healthy sufferers. Calculation is based on pharmacokinetic and pharmacodynamic studies carried out in experimental hemorrhagic shock. For instance, the baroreceptor depression produced by intravenous brokers is normally milder than that of 3809 inhalational brokers. Opioid agents have little direct cardiovascular or baroreflex depressant effect; nevertheless, these agents may cause hypotension by inhibiting central sympathetic activity, particularly in the hypovolemic trauma affected person whose apparent hemodynamic stability is maintained by hyperactive sympathetic tone. Two essential principles in using anesthetic brokers are accurate estimation of the diploma of hypovolemia and reduction of doses accordingly. The presence of hypotension suggests uncompensated hypovolemia, in which case anesthetics almost invariably produce further deterioration of systemic blood stress and generally cardiac standstill. When time constraints or persevering with hemorrhage stop restoration of blood quantity, the airway may be secured without the good factor about anesthesia (perhaps utilizing solely rapidly appearing muscle relaxants and small doses of opioids, etomidate, or ketamine), although this approach could end in recall of induction and intraoperative occasions in as a lot as 40% of patients, and, as mentioned before, important organ ischemia. Intraoperative use of the bispectral index monitor and, every time possible, titrating anesthetics to bispectral index ranges lower than 60 might prevent recall in trauma sufferers. In normotensive however hypovolemic sufferers, restoration of quantity and selection of an agent with the least cardiovascular depressant impact seems logical. Ketamine and etomidate are the preferred induction brokers,257 though at low doses different intravenous anesthetics are also unlikely to produce hypotension. Therefore, the use of any of these medication in reduced doses is probably extra necessary than the actual agent chosen. Maintenance of anesthesia within the hypovolemic trauma patient raises concerns much like these pertaining to induction. Under these circumstances, patients are unlikely to reply to the sympathetic impact of N2O, and the cardiovascular depressant properties of the gas are unmasked. In addition, by decreasing FiO2, use of N2O incurs a risk of hypoxemia in patients with decreased cardiac output or pulmonary compromise. Despite causing little impairment of reflex tachycardia and having a vasodilatory exercise that preserves organ blood move in normovolemic sufferers, isoflurane can impair cardiac output and organ blood move in hypovolemia-that is, it can trigger cardiovascular despair. However, due to their low solubility in blood, the severe hemodynamic melancholy produced by these brokers may be quickly reversed, preventing suboptimal perfusion for a major time period. Head and Open Eye Injuries the importance of deep anesthesia and sufficient muscle relaxation throughout airway management of sufferers with head or open eye injuries has already been mentioned. Hypotension attributable to anesthetics or different elements contributes to the event or development of cerebral ischemia. This problem can be ameliorated by administering pretreatment doses of opioids (fentanyl, 2 to 3 g/kg), which permit reduction of the anesthetic dose. Nevertheless, myoclonus is best prevented by cautious timing of the dose of muscle relaxants. Isoflurane has the least vasodilatory impact and thus is probably the most widely used inhalation anesthetic, though desflurane and sevoflurane have comparable results on the cerebral circulation. In these sufferers, anesthesia may be maintained initially with opioids plus propofol, midazolam, or etomidate. This impact could also be eliminated when this agent is run with adequate doses of barbiturates or hyperventilation.
Cheap rogaine 2 60ml with visaSedation could be added to regional anesthesia but may cause problems with apnea in ex-premature infants man health trend discount rogaine 2 60ml line. The landmarks are the coccyx, the two sacral cornua, and the posterior superior iliac spines. Several needle types could also be used, however the "pop" by way of the sacrococcygeal ligament is greatest noticed with a blunt-tipped needle, whereas an intravenous catheter advanced over a needle might present extra confirmation of sacral canal entry. The caudal area is identified by "pop" through the sacrococcygeal ligament, ease of native anesthetic injection, and absence of subcutaneous swelling upon dose delivery. Other methods to determine the caudal house have been described, including stimulating technique129 and ultrasound steering. Evidence of an intravascular injection embody (1) peaked T waves (which may be of comparatively brief duration), (2) increase in heart rate, and (3) improve in blood strain. Another approach to minimize the potential difficulties of an intravascular injection is to fractionate the dose by dividing the total dose into three aliquots and ready approximately 20 to 30 seconds between every aliquot before continuing the injection. In addition, a single-injection caudal anesthetic can present analgesia for 6 to eight hours. Epinephrine, 1:200,000, is added to local anesthetics to assist in determining if there was an intravenous injection. Ropivacaine has been reported to be less cardiodepressant than equipotent doses of bupivacaine. If a caudal catheter is positioned, an infusion of ropivacaine, bupivacaine, lidocaine, or chloroprocaine could be administered and supply analgesia for a number of days postoperatively. Current suggestions for infusions in neonates and younger infants are for an preliminary loading dose of zero. However, warning should be exercised in neonates and infants who may be vulnerable to apnea with even average doses of opioids within the epidural house. Ultrasonography can be used for localization of the caudal house in infants whose anatomy will not be obvious. This offers analgesia for hernia restore, circumcisions, and lower belly surgeries. Although some practitioners favor utilizing a caudal path to place catheters within the epidural space, lumbar and thoracic epidural catheters may be simply positioned in neonates. It is imperative to limit the dose of native anesthetic resolution in neonates and kids to avoid toxicity. The dorsal nerves of the penis are situated on both aspect of the shaft of the penis. A ring block using local anesthetic without epinephrine can be used to present analgesia following circumcision. Because the penis is innervated by the two dorsal penile nerves that are branches of the bilateral pudendal nerves and in addition inntervated by the perineal nerves which are additionally branches of the pudendal nerves, the ventral surface of the penis may have a hoop block with care to keep away from the urethra for complete block of the penis. However, we discover that blockade of those nerves can present sufficient postoperative analgesia. Immediately medial to the anterior superior iliac spine, a needle is inserted towards the umbilicus and native anesthesia is fanned into the area. The advantage with the utilization of ultrasonography is the ability to considerably cut back the dose of local anesthesia. The layers of the abdomen together with the external oblique, transversus abdominis, and iliacus muscle tissue are recognized. The ilioinguinal and 2981 iliohypogastric nerves are situated beneath the interior oblique muscle and within the airplane between the internal indirect and the transversus abdominis muscle. This block has successfully been used to provide analgesia for infants and neonates present process major abdominal surgical procedure, together with colostomy placement. This block is particularly helpful in neonates who endure muscle biopsies of the lateral thigh. Using ultrasonography during the axillary approach to identify every branch of the brachial plexus permits selective block of each nerve,138 thus reducing the total dose of local anesthetic. A single shot supraclavicular approach to the brachial plexus may also be used for providing analgesia for upper extremity surgery. It is important to visualize using ultrasonography as a outcome of the pleura is comparatively close to the world of curiosity and injection. For sustained pain reduction, an infraclavicular catheter could also be used and is definitely held in place by further muscle and fascial layers which make this a preferable method to catheter placement for upper extremity surgical procedure. Neurosurgical Blocks Peripheral nerve blocks of the top and neck are useful for many surgical procedures. Peripheral nerve blocks of the trigeminal nerve and occipital nerve branches could also be used to present analgesia whereas avoiding basic anesthesia. The use of intraoperative epidural anesthesia adopted by postoperative epidural native anesthetics or opioids has been in style in older youngsters and adults, and these strategies are being applied to neonates. In addition, most neonatologists are skilled with the intravenous administration of opioids for affected person consolation. Commonly used systemic therapies for postoperative pain are listed in Table 42-7. Oral Routes Oral routes of medicines have been used for decades in neonates and children for managing ache. The commonly used oral analgesics embrace 2983 nonsteroidal analgesics together with acetaminophen (10 to 15 mg/kg) and ibuprofen (5 to 10 mg/kg), and opioids, including hydrocodone (0. A bigger dose than is often given orally is needed in infants to obtain good blood ranges, due to unreliable absorption. A dose of 20 to 30 mg/kg of rectal acetaminophen is mostly recommended for postoperative ache management. Diclofenac, a generally obtainable rectal suppository in Europe, is incessantly utilized in infants for postoperative ache control. Intravenous Analgesia Opioids are the mainstay of analgesia in neonates and infants in the postoperative period. Morphine and fentanyl are incessantly used within the neonatal intensive care unit for analgesia. However, the potential for opioid tolerance after prolonged infusion of opioids is somewhat frequent. To lower the chance of opioid tolerance,forty four one can rotate opioids or add other medications including steady intravenous naloxone142 and intravenous methadone. Other intravenous nonsteroidal anti-inflammatory medicines and intravenous acetaminophen, have been launched. Intravenous ketorolac, a nonsteroidal anti-inflammatory drug, has been used successfully 2984 in neonates and infants for pain management at a dose of 0. Postoperative air flow places the neonate at added threat due to the problems related to mechanical air flow, the trauma to the subglottic area, and the potential development of postoperative subglottic stenosis or edema. Special Considerations Maternal Drug Use throughout Pregnancy Many drugs taken during pregnancy can have an effect on the fetus and neonate. During being pregnant, maternal drug use of cocaine, marijuana, and others results in a host of problems for the neonate. Cocaine use, for example, leads to a decreased catecholamine reuptake, which can outcome in the accumulation of catecholamines.
Discount 60ml rogaine 2 with amexPulmonary edema and restrictive pulmonary dysfunction are commonly seen in patients with renal failure and are usually responsive to prostate cancer young man cheap rogaine 2 60ml with mastercard dialysis. Hypervolemia, coronary heart failure, reduced serum oncotic strain, and elevated pulmonary capillary permeability are related components in the growth of pulmonary edema. Unfortunately, clearance of most medicines involves a extra complicated combination of each hepatic and renal features, and drug stage measurement or algorithms for specific drugs are often recommended. However, plasma protein binding is extremely variable, with acidic medicine having decreased binding and fundamental agents. Importantly, for medicine with much less binding, "normal" drug ranges may mirror dangerously excessive lively (unbound) drug levels. For instance, therapeutic phenytoin ranges are sometimes reported as being within the range of 10 to 20 mg/mL normally but four to 10 mg/mL in circumstances of renal failure. The nephrotoxicity of methoxyflurane appears to be because of its metabolism, which leads to release of the fluoride ions believed liable for the renal harm. Although direct anesthetic effects on the kidney are usually not dangerous, oblique effects might mix with hypovolemia, shock, nephrotoxin exposure, or different renal vasoconstrictive states to produce renal dysfunction. If the chosen anesthetic approach causes a protracted reduction in cardiac output or sustained hypotension that coincides with a interval of intense renal vasoconstriction, renal dysfunction or failure could end result. Significant renal impairment might affect the disposition, metabolism, and excretion of the generally used anesthetic brokers. Inhalation anesthetics are, after all, an exception to the rule that drugs with central nervous system activity (which usually are lipid soluble) have to be transformed to extra hydrophilic compounds by the liver earlier than being excreted by the kidney. Many drugs used in anesthesia are highly protein certain and should show exaggerated clinical results when protein binding is reduced by uremia. Burch and Stanski68 confirmed that the free fraction of an induction dose of thiopental is sort of doubled in sufferers with renal failure. Ketamine is less extensively protein bound than thiopental, and renal failure seems to have less influence on its free fraction. Redistribution and hepatic metabolism are largely responsible for termination of the anesthetic effects, with lower than 3% of the drug excreted unchanged in the urine. Propofol undergoes in depth speedy hepatic biotransformation to inactive metabolites which are renally excreted. Certain benzodiazepine metabolites are pharmacologically lively and have the potential to accumulate with repeated administration of the father or mother drug to anephric patients. For instance, 60% to 80% of midazolam is excreted as its (active) -hydroxy metabolite,72 which accumulates throughout long-term infusions in patients with renal failure. Volunteers with renal impairment receiving dexmedetomidine skilled a longer-lasting sedative impact than subjects with normal kidney function. The most probably clarification is that less protein binding of dexmedetomidine happens in subjects with renal dysfunction. However, continual administration ends in accumulation of its 6-glucuronide metabolite, which has potent analgesic and sedative results. Hydromorphone is metabolized to hydromorphone-3-glucuronide, which is excreted by the kidneys. This active metabolite accumulates in sufferers with renal failure and should trigger cognitive dysfunction and myoclonus. Renal failure has no effect on the clearance of remifentanil, however elimination of the principal metabolite, remifentanil acid, is markedly lowered. Only succinylcholine, atracurium, cis-atracurium, and mivacurium appear to have minimal renal excretion of the unchanged father or mother compound. Most nondepolarizing muscle relaxants should be either hepatically excreted or metabolized to inactive types so as to terminate their activity. Although the next dialogue focuses on the pharmacology of individual muscle relaxants, coexisting acidosis and electrolyte disturbances in addition to drug remedy. However, use of a steady succinylcholine infusion raises considerations as a outcome of the main metabolite, succinylmonocholine, is weakly energetic and excreted by the kidney. Use of the longacting muscle relaxants doxacurium, pancuronium, and pipecuronium may additionally be questioned in patients with identified renal insufficiency. Similar findings have been reported for the 3536 pharmacokinetics of pipecuronium. Atracurium and its derivative, cis-atracurium, endure enzymatic ester hydrolysis and spontaneous nonenzymatic (Hoffman) degradation with minimal renal excretion of the parent compound. One potential concern is that an atracurium metabolite, laudanosine, may trigger seizures in experimental animals and may accumulate with repeated dosing or continuous infusion. Table 50-4 Nondepolarizing Muscle Relaxants in Renal Failure Initial stories suggested that the pharmacokinetics of vecuronium are unchanged in renal failure, but it has subsequently emerged that its duration of motion is prolonged because of reduced plasma clearance and increased elimination half-life. Rocuronium has a pharmacokinetic profile in normal topics similar to that of vecuronium. The short-acting muscle relaxant mivacurium is enzymatically eliminated by plasma pseudocholinesterase at a somewhat slower fee than succinylcholine. Low pseudocholinesterase activity correlates with slower recovery from a bolus dose of mivacurium in anephric sufferers. The pharmacokinetics of the clinically out there anticholinesterases are affected by renal failure. The anticholinergic brokers atropine and glycopyrrolate, used along side the anticholinesterases, are similarly excreted by the kidney. Therefore, no dosage alteration of the anticholinesterases is required when antagonizing neuromuscular blockade in sufferers with decreased renal perform. This agent is a modified -cyclodextrin that encapsulates aminosteroidal neuromuscular blocking brokers. Edema results when Starling forces favor passage of fluid into the interstitial area. Fluid overload because of quite so much of persistent conditions (congestive heart failure, renal failure, or hepatic cirrhosis) may be first acknowledged throughout preoperative evaluation and should require that elective surgical procedure be delayed for therapy to scale back operative risk. The first line of remedy for fluid overload that includes all physique compartments includes restriction of salt and water ingestion; nevertheless, diuretic remedy is 3538 often indicated. The Physiologic Basis of Diuretic Action Diuretics are typically grouped in accordance with their site and mechanism of motion. Under normal circumstances, kidney function assures that lower than 1% of the filtered Na+ load enters the urine. This pump causes a net movement of positive charge out of the cell (2 K+ in, for each 3 Na+ out) creating an electrochemical gradient that also causes Na+ to enter the luminal (urine) facet of the cell. Renal tubular cells in numerous parts of the nephron have completely different luminal "systems" to permit this Na+ influx. Carbonic anhydrase inhibitors are drugs that inhibit this enzyme; the online effect of those brokers is that sodium and bicarbonate, which would otherwise have been reabsorbed, stay within the urine and result in an alkaline diuresis. Although sufferers may develop a metabolic acidosis when taking these agents, compensatory processes within the tubules accommodate the consequences of carbonic anhydrase inhibitors in order that their long-term use not often causes this downside.
References - Schrem H, Luck R, Becker T, et al. Update o- liver tra-spla-tatio- usi-g cyclospori-e. Tra-spla-t Proc. 2004;36(9):2525-2531.
- Page, MM and Watts, GF. PCSK9 inhibitors - Mechanisms of action. Aust. Prescr. 2016;39(5):164-167.
- Bohrer H, Bach A, Fleischer F, et al: Adverse haemodynamic effects of high-dose aprotinin in a paediatric cardiac surgical patient, Anaesthesia 45:853, 1990.
- Sanders, D. L., Kingsnorth, A. N. The modern management of incisional hernias. BMJ. 2012; 344:e2843.
- Han M, Partin AW, Zahurak M, et al: Biochemical (prostate specific antigen) recurrence probability following radical prostatectomy for clinically localized prostate cancer, J Urol 169(2):517n523, 2003.
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med. 2011;365:883-891.
- Global Strategy for the Diagnosis, Management and Prevention of COPD, Global Initiative for Chronic Obstructive Lung Disease Revised 2011.
|


