|
Molly A. Schnirring-Judge, DPM, FACFAS - Director of Podiatric Clerkship Program
- Department of Surgery
- St. Vincent Charity Hospital
- Cleveland, Ohio
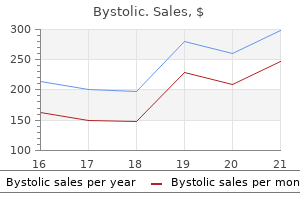
Bystolic dosages: 5 mg, 2.5 mg
Bystolic packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Discount 2.5 mg bystolic fast deliveryThose resulting in blood pressure medication green pill buy generic bystolic on line greater than 1 cm length loss or higher than 5� angulation are thought of main. Depression also happens in some sufferers but responds properly to the momentary use of antidepressants. The pain, lack of appetite, and melancholy during lengthening often resolve spontaneously one week after stopping the distraction. This occurs due to persistent muscle contractures or could additionally be because of stiffness of the joint because of the increased pressure on the joint surface during lengthening. The latter is a theoretical consideration but is a priority for the longterm since nobody yet knows what the impact of this momentary increased strain on articular cartilage will be. All joint stiffness is considered a real complication, the severity of the complication is determined by the practical limitation created. Obviously, 15� loss of knee extension and ankle dorsiflexion is much more critical than a 15� loss of the knee flexion and ankle plantarflexion. Materials and Methods Fortysix sufferers 2�54 years of age had been treated by the Ilizarov technique of limb lengthening with or with out simultaneous correction of deformity. A total of 60 limb segments had been lengthened-40 tibiae, 12 femura, four radii, one humerus, and three ft. There was a big difference in the therapeutic time between children (defined as underneath the age of 20 years) and adults. Contraction of any muscle transfixed by pins is initially painful however resolves inside every week or two. Therefore, a double degree lengthening of the tibia that includes a complete of four osteotomies (fibula and tibia) may be very painful on the primary day. During the distraction phase of lengthening, a chronic uninteresting aching pain is usually experienced. It is extra widespread with longer lengthenings and especially with doublelevel lengthenings. It is more widespread with fixation and splinting of the joints above and beneath the lengthening section. The pain, while present at all times, is normally solely noticed at night and during physiotherapy and strolling. For pain, the creator prescribes acetaminophen with codeine derivatives and avoids oxycodone derivatives because of their elevated tendency to produce dependency in susceptible people. Splinting the knee in extension at evening leads to elevated difficulties with sleep. In one peroneal nerve damage from a wire at the start of an extensive limb lengthening, a prophylactic decompression of the peroneal nerve on the fibular neck was performed to permit the lengthening to proceed without applying early pressure on the traumatized nerve. This nerve went on to recovery of the tibialis anterior and extensor digitorum muscle tissue, and partial recovery of the extensor hallucis longus. In the identical patient, at the distal end of that nerve, the sensory department to the primary internet house had been pierced by a wire, and was explored and severed in the course of the try at elimination of the wire. However, in the first patient the author operated on, displacement of the tibia throughout corticotomy led to probable laceration of a branch of the anterior tibial artery and a hematoma in the anterior compartment of the leg. In the first double stage tibial lengthening on this sequence, severe postoperative ache in the leg was misdiagnosed as a compartment syndrome due to faulty compartment pressure measurements. In both of these cases, the skin of the fasciotomy incisions was closed secondarily 2 weeks after decompression with out pores and skin grafting. In three patients, buckle fractures occurred after removing of the apparatus, resulting in 5�10 mm loss of length. Complete patient satisfaction was achieved in 45 of forty eight sufferers, and partial satisfaction was achieved in the remaining three. There were 35 problems that needed to be resolved in the outpatient clinic in the course of the treatment-20 pin infections (13 patients), 10 axial deviations, two untimely consolidations, two delayed consolidations, and one knee subluxation. There have been eleven obstacles throughout lengthening that required surgical intervention-two pin infections, one pin cutout, two axial deviations, one untimely consolidation, two incomplete cortico tomies, two incorrect constructs, and one bone cyst. There have been a complete of 28 true issues, of which 17 have been thought-about minor and of little significance. The minor issues had been three axial deviations (< 5�), three contractures (recovered), 4 sensory nerve injuries (recovered), a length loss of 1 cm in three, two delayed consolidations, one pseudo compartment syndrome, and one hematoma. Nine complications, of which solely three affected the achievement of unique objectives. The major true complications were one reflex sympathetic dystrophy, one equinus, one nonunion, two late bowing and 4 motor palsy. Of the true problems, seven had been a direct results of surgical injury intraoperatively-three motor nerve injuries, three sensory nerve accidents, and one hematoma. Of all these issues, obstacles, and issues, the one significant residua were one bowing of the distal femur of 25� in the airplane of movement of the knee, one recurrent varus deformity of the tibia, and one nonunion of ankle arthrodesis lengthening. The mistakes in all three instances had been untimely removing of the equipment with insufficient publish removal protection. In all three cases, the equipment had loosened and now not managed the bone ends. Instead of reinserting new wires for stabilization, the equipment was eliminated, and a plaster solid was utilized for a brief time period. Had the wires been reinserted and tensioned, higher fixation would have been achieved, allowing better maturation of the regenerated bone. The solely true nonunion on this sequence resulted from a simulta neous lengthening of a proximal tibial corticotomy and a tibiotalar arthrodesis web site. Both produced wonderful bone, but too early removing of the apparatus resulted in a nonunion of the tibiotalar arthrodesis. Residual stiffness of joints is the one complication that was not well assessed in this study. Most patients had absolutely recovered their vary of movement on the knee and nearly fully recovered their range of movement on the ankle at the time of review, regularly with a residual 5�10� lack of dorsiflexion and full return of plantarflexion. Longer followup study is important to give a whole assessment of this late complication. The different minor or major complications resolved spontaneously, whereas one equinus contracture had a tendoAchilles lengthening. For instance, the peroneal tendon and knee contractures recovered with physiotherapy. Discussion In this chapter, an try has been made to analyze the difficulties that come up from limb lengthening by the Ilizarov technique. Those that might be dealt with by nonoperative means have been considered issues, and those who have been treated by operative means have been thought-about obstacles. Only intraoperative surgical harm and residual issues remaining on the end of lengthening had been thought-about true problems. The importance of this type of breakdown is that it better represents to both the surgeon and the patient, the complexity and the dangers of limb lengthening. Most of the problems are handled by numerous timeconsuming changes to the equipment within the outpatient division. Therefore, this directly correlates with hours spent modifying the equipment to obtain varied corrections and stop the event of problems. Essentially, it represents the unplanned reoperation price for issues that happen during the lengthening.
Generic 5mg bystolic with amexCut harm at proximal forearm often should spare the thumb extensor muscle tissue as they originate extra distally blood pressure high bottom number order bystolic with a visa. If patient is unable to lengthen the thumb in proximal forearm damage posterior interosseous nerve injury must be suspected. Outcome of surgical restore of the posterior interosseous nerve is very good due to virtually pure motor nature of the nerve. Clinical examination would reveal weakness of extension of the injured finger, pain on resisted extension and lack of hyperextension of the injured finger. Testing for active extension of the affected digit whereas holding the remaining fingers neutralizes the pull of juncture; and will reveal lack of complete extension of the finger with injured tendon. Tendons at this degree may be repaired with 3-0 Prolene core sutures and 5-0 Prolene epitendinous sutures. Due to interconnected nature of the extensor tendons, extensor digitorum damage to any finger ought to require splinting of all of the 4 digits. Thumb Thumb being an important of all digits needs particular consideration to its extensor tendon damage. Splinting in extension for 6�8 weeks or K-wire stabilization of the thumb interphalangeal joint in extension gives equally good results. Its division to some extent is at all times required to expose and repair the injured tendons. Complete excision of retinaculum ought to be avoided as it may end up in bowstringing of the extensor tendons with related weak spot and useful deficit. This would also provide more room for the repaired extensor tendons to glide under. At this zone, the extensor tendons of various digits are near one another and therefore multiple tendon damage is more widespread. Matching of the minimize ends may be done based mostly on the dimensions of tendon, path of the laceration and anatomical location of the tendon. Tendons listed right here are round and ponderous and can be repaired with two or 4 strand core suture utilizing 3-0 or 4-0 Prolene supplemented with 5-0 Prolene epitendinous sutures. In this zone, the tendon rehabilitation ought to have an early mobilization protocol like flexor tendons to stop adhesions of the multiple tendons under the retinaculum. In case of delayed shows, the rerouting may present elevated size and tension-free repair. In such circumstances, transfer of extensor indicis to restore the operate is simpler and extra dependable method than interposition tendon grafting. At another middle, the extensor tendons had been repaired with out repairing the posterior interosseous nerve. Absence of thumb extension (arrow) with proximal forearm level harm ought to alert the surgeon of the risk of the posterior interosseous harm. Encouraged with the success of early mobilization after flexor tendon repair these rehabilitation protocols have been applied to extensor tendons also. The particulars of the splinting and rehabilitation are mentioned together with the administration of the extensor tendons in particular zones. Rehabilitation technique adopted for a given case would rely upon factors like the character of damage to the tendon and associated accidents, zone of the harm, quality of repair and patient profile. Report of the Committee on Tendon Injuries (International Federation of Societies for Surgery of the Hand). A method for reconstruction of the central slip of the extensor tendon of a finger. Reconstruction of the extensor central slip using a distally base flexor digitorum superficialis slip. A biomechanical study of extensor tendon restore methods: introduction of the running-interlocking horizontal mattress extensor tendon restore technique. Closed remedy of non-rheumatoid extensor tendon dislocations at the metacarpophalangeal joint. Dynamic lumbrical muscle switch for correction of post-traumatic extensor tendon subluxation. A comparability of outcomes of extensor tendon repair followed by early managed mobilisation versus static immobilisation. A study of the dynamic anatomy of extensor tendons and implications for treatment. A single finger extensor loss could be managed with side-hitching or transfer of extensor from the aspect finger. With multiple finger involvement the options include reconstruction utilizing the bridging graft or by tendon transfer. The wrist level tendon transfer donors would solely attain the distal third of the forearm, but the flexor digitorum superficialis can attain till the dorsum of the hand. Sometimes the size might have to be increased with tendon graft or fascia lata extension to reach the distal minimize end. Complications the commonest and probably the most important downside with extensor tendon surgery is limitation of flexion and the resultant lowered grip power. This can happen because of two reasons: first, as the extensor tendons have lesser tour than the flexors especially within the distal zones, shortening can result in decrease in flexion. This could be prevented by considered selection of the rehabilitation regimen depending on the damage characteristics, high quality of the repair achieved and the affected person profile. Various environmental and genetic factors have been identified which disturb normal embryogenesis at specific level of time resulting in these anomalies. Congenital anomalies affect 1�2% of neonates, and of which 10% have upper limb anomalies. Earliest written reference is the Bible where a giant named Gath or Goliath had six fingers and toes. The Thalidomide babies in the 1960s then spurred newer primary research within the space. Molecular Biology of Limb Development the initiation of limb bud is poorly understood and limb forming potential is current alongside the entire length of lateral mesoderm. Wingless type (Wnt) signaling center-the nonridge ectoderm in the dorsum of limb bud controls the dorsovenrtal spatial improvement. The pathway produces transcription factor, Lmx1 that induces dorsalization of the mesoderm. In ventral mesoderm, a product of gene Engrailed1 (En1) is produced which blocks the Wnt pathway. It is charac terized by patterns of repeated motifs, regulated progress and programmed segmentation. Limb growth is a threedimensional process with three spatial axes, the proximal-distal, the dorsal-ventral and the anterior-posterior/radial-lunar/preaxial-postaxial axis.
Discount bystolic 5mg overnight deliveryIntertrochanterIc Fractures oF Femur this concept applies primarily to methods to forestall hip fractures blood pressure medication used for sleep cheap 2.5mg bystolic with visa. Falls with a rotational element are more common with extracapsular hip fractures. However, the most effective radiographic analysis of the hip fracture occurs in the operative suite with fluoroscopic C-arm views. During surgery, surgeon have to be prepared to change his plan of alternative of implant after anatomic reduction, if needed. The space of assembly between the secondary pressure trabecular and the compression trabecular within the heart of the head of femur carries the densest portion of cancellous bone, during which an effort is made to have interaction the tip of the sliding screw. Sometimes, an additional cancellous screw fixation above the sliding screw is suggested in severely osteoporotic neck and/or basal fractures. Treatment the aim of treatment is to achieve union with out deformity and encourage early mobilization to cut back the morbidity and mortality rates and to restore the affected person to his or her preoperative useful status on the earliest potential time. Comminution the diploma of comminution is determined by osteoporosis and drive of harm. When the mixed influence of osteoporosis and comminution is considered, the most stable fracture is the two-fragment fractures of porotic bone. Osteoporosis and comorbidities provides to the complexity of the fracture and its management. Multiple modalities of remedy, implants and surgical methods have to be mastered. The stability after surgical treatment signifies union of fracture without deformity and good function. Currently, reduction of anteromedial cortex has been given much significance to obtain stability. As there are a big number of fracture patterns, comminution and extreme osteoporosis make the fracture treatment complex, due to this fact, needs all kinds of implants instruments and carefully mastering the procedures instrumentation. It is important for an orthopedic surgeon to perceive the biomechanics of the various implants. Indication for Nonoperative Treatment � An elderly person whose medical condition carries an excessively excessive risk of mortality type anesthesia and surgery � Nonambulatory patient who has minimal discomfort following fracture � the conservative therapy by skeletal tibial traction may be tried for 8�12 weeks � Intensive medical and nursing care is required to forestall strain sores, pneumonia, urinary tract infection, thromboembolism, and pin-tract sepsis. Factors under the control of surgeon for successful therapy are: � Good discount � Proper choice of implant � Proper surgical technique, which includes availability of recent operation rooms and entire set of implants and instrumentations � Availability of picture intensifier and clean air system (laminar air flow) in operation rooms can additionally be necessary. The components most important for instability and fixation failure are: � Loss of posteromedial or medial cortical help � Severe comminution � Subtrochanteric extension of the fracture � Reverse indirect fracture � Shattered lateral wall � Bone high quality. There are numerous articles with meta-analysis and randomized, potential research; nonetheless there are lot of controversies relating to number of implants and procedures. Screw of sliding within the barrel is determined by: � Fracture geometry � Quality of reduction � Position of screw within the head and neck of femur � Angle of the barrel and plate � Integrity of lateral wall. The shearing pressure on the femoral head being transferred to the axis of the sliding screw, hence producing a compressive force. Note the tension in the aspect plate to compress the fracture of the lateral cortex. For this reason, the head screw is positioned larger to achieve distance inside the proximal fragment. Even if the fracture unites, there may be thigh pain, shortening of limb and unhealthy limp Cutout of implant may happen in extreme osteoporotic bone Reverse indirect fracture are unstable fractures. Excessive collapse happens due to shearing forces and to powerful muscular tissues performing on fragments. Reduction: Patient is positioned in a supine position on a fracture desk, preferably under epidural anesthesia. Reduction of the fragments, especially the anteromedial, is an important prerequisite for good union. Anatomical reduction can be achieved by closed method by making use of traction to over distract. Most fractures are lowered by direct traction, slight abduction and normally 10�15% inside rotation. Occasionally slight external rotation could also be required for more intensive and comminuted fractures. With picture intensifier the limb ought to be rotated internally to obtain passable reduction. It is necessary to verify on the lateral projection that the shaft has not sagged posteriorly. Once discount is achieved, most necessary step is to preserve it, until definitive fixation is full. With elevation of the sagging shaft, a Steinman is passed from higher trochanter into the pinnacle of femur as provisional fixation to preserve the reduction. The valgus place of the proximal fragment reduces the deforming drive and the incidence of fixation failure, and makes the fracture more steady. In an osteoporotic bone with comminuted fracture, anatomical reduction is tough if not unimaginable. In comminuted fractures, the greater trochanter fragment is pulled superiorly to enable direct visualization of the fracture. This maneuvers denervates the posterior fiber and is related to greater bleeding. Occasionally, the sharp anteromedial spike of the proximal fragment is entrapped in the overlying rectus femoris muscle tissue. The level of coalescence of the strain and compression trabeculae leads to a dense sample of cancellous bone in the heart of the femoral head. This is where one of the best purchase within the bone could be obtained for a fixation gadget. When these trabecular are absent, the surgeon can count on a better price of failure with use of any device. The tip-to-apex distance has been described by Beumgaertner67 as a information to accurate screw placement, and should be less than 25 mm. Tip-to-apex distance helps outline screw place and risk of cutout and is easily measured intraoperatively. If the screw is placed inadvertently within the superior half of the pinnacle, then the next angled barrel plate (140�) could additionally be required. If the screw is positioned within the lower half of the head, barrel and plate angle is less than 135�, often 130�. Tapping of the femoral head to cut screw threads prior to insertion of the screw is recommended in all, but the most Advantages of Central Placement of the Implant � the putting of the lag screw in a central position avoids the potential complication of a peripherally placed screw, which can appear to be inside the femoral head. This will reduce the torsional stress and thereby the risk of rotation of the proximal fragment during insertion of the screw. An various method of stopping rotation is by placing a supplementary guidewire across the fracture.
5mg bystolic amexAn inverted "T or Y" configuration involving the entire base of the metacarpal is referred to as a Rolando fracture blood pressure medication rebound effect generic bystolic 5mg free shipping. These fractures are also unstable and require stabilization after correct reduction. Assessment of these fractures after fixation is troublesome unless correct imaging is obtained. The Roberts pronated true anteroposterior view offers a transparent view of the joint and congruity is greatest assessed in this view. Though low on the proof score scale, a good total evaluation of the operative administration of hand fractures is outlined by Freeland and Orbay. Bicortical self-tapping mini screw fixation of extraarticular oblique metacarpal and phalangeal fractures simplifies screw insertion and provides stability similar to that of fractures fastened with lag screws. Percutaneous intramedullary wire fixation might afford appropriate fixation for unstable extra-articular oblique as well as transverse metacarpal fractures. Unicortical screw fixation of mini plates securing transverse extra-articular metacarpal fractures affords stability similar to that of 1740 TexTbook of orThopedics and Trauma 4. In vitro kinematics of the proximal interphalangeal joint within the finger after progressive disruption of the primary supporting buildings. Dynamic intradigital external fixation for proximal interphalangeal joint fracture dislocations. Minimally invasive finger fracture administration: wide-awake closed reduction, K-wire fixation, and early protected motion. The dissection required for plate fixation and the small surface area of transverse fractures delay and sometimes impair bone healing. Primary bone grafting of diaphyseal defects in clean secure wounds may shorten and simplify therapy and reduce morbidity. Synchronous wrist and digital workout routines may scale back peritendinous fracture adhesions. Early motion of adjacent joints in closed easy metacarpal fractures expedites recovery of motion and strength with out adversely affecting fracture alignment and leads to earlier return to work". With increasing attention to sports in any respect levels and with better facilities and propaganda, the number of such accidents in not solely skilled gamers, but additionally the casual gamers is on the rise. The enhance in journey actions and the hustle and bustle of public transport in crowded metropolitan areas add to the incidence of those injuries. These injuries stop additional participation in sport and are fairly disabling even in actions of every day dwelling. Identifying these injuries early and treating them correctly can result in wonderful restoration and return to the identical level of the sport or professional, leisure and private exercise. Terminal Interphalangeal Joint Collateral ligament accidents as additionally dislocations of the terminal interphalangeal joint are rare. More common injuries associated with this joint are avulsion fractures (mallet and jersey finger) or tendon avulsions. Dorsal dislocations are sometimes related to wounds as the pores and skin of the pulp is tethered to the bone to permit agency gripping and stability to hold objects. Dislocations are simple to scale back and regain stability, if the adjoining buildings are uninvolved in the injury. Crushing accidents with dislocations are extremely unstable and need extra K-wire stabilization for varying periods. The correct collateral ligament fans out from the neck of the proximal phalanx to insert on the side of the center phalanx. The volar plate and the collateral ligaments type three sides of a field which reinforces the stability of the joint. The dorsal capsule is additional strengthened by the central extensor slip and despite this stays probably the most vulnerable part of the joint. A vital lateral impact, normally a glancing harm from a ball, can cause the collateral ligament to get avulsed from the proximal phalanx. Movements are painful and despite the passage of time and anti-inflammatory medicines, the discomfort persists. Stress X-rays are helpful in diagnosing the damage however the opening up of the joint is very deceptive. Through a lateral approach the collateral ligament is identified and the ligament is freshened. Once the anchor is placed securely, a Bunnell sort suture is run through the ligament finish and the ligament is reattached. Type I (Hyperextension) Avulsion of the volar plate from the base of the center phalanx and a minor longitudinal split in the collateral ligaments is seen. In this, the articular surfaces stay in contact, the middle phalanx articulates with the dorsal third of the condyle of the proximal phalanx. Attempts at flexion is commonly painful and even passive flexion is at instances not attainable because the ruptured volar plate, a sturdy structure, now edematous, is interposed in the joint. The collateral ligaments are normally intact or solely few fibers are involved within the damage. The insertion of the volar plate, including a portion of the volar base of the center phalanx is disrupted. The major portion of the collateral ligaments remains with the volar plate and flexor sheath. In the hyperextension injuries, discount is stable and permits early mobilization. Irreducible or locked hyperextension the volar plate is ruptured and will get interposed between the joint surfaces. With a correct rehabilitation program, full actions could be restored in these instances. Dorsal dislocations are normally decreased by the affected person himself or a useful colleague or the staff physiotherapist. Once reduced, an evaluation of the instability is important to verify whether the volar plate needs to be repaired. In compound injuries, it might be prudent to take the chance to restore the volar plate and if the collateral is injured, a well-placed suture will help in regaining full function in the finger. This ensues from splinting in too much flexion and relying too much on the "ball bandage" position. These contractures are proof against dynamic splinting and bodily therapy, if not attended to early. The collateral ligaments are attached to the pinnacle slightly dorsally to the axis of rotation. However, associated delicate tissue injuries could cause lingering symptoms and discomfort. Rarely, avulsion fractures result in appreciable instability and at instances, there could additionally be an entire rupture of the collateral ligament without an avulsion fragment. Stress X-rays are useful is deciding which of those require to be addressed surgically. In simple subluxations, the volar plate remains attached to the proximal phalanx and is stretched over the metacarpal head. It is liable to tear and get transformed to an entire dislocation with improper attempts at reduction.
Generic bystolic 2.5mg visaThe tunnel ought to be situated as medially within the radial tuberosity as attainable with the forearm supinated to recreate probably the most anatomic location for the tendon blood pressure chart for excel order bystolic 5mg fast delivery. Create a cortical window for the tendon on the anterior floor of the tuberosity by use of a high-speed bur. Next, a information pin for the Endobutton cannulated drill is placed through the anterior tunnel through the posterior cortex to exit the skin posteriorly. Then a running locking sort of suture is positioned with a strong, braided nonabsorbable suture. The suture is superior proximally on the tendon for about 2 cm and then distally exits the tendon end. The suture 2039 limb is then handed by way of the button earlier than re-entering the tendon to complete the loop. The knot should be tied leaving a maximum 2�3 mm gap between the button and the free tendon end to allow the button to be manipulated and "flipped" over the dorsal cortex. The two outer holes of the Endobutton are then each threaded with a unique colour suture to determine the sutures as they draw the Endobutton into the socket and onto the posterior cortex. A beath pin is superior by way of the outlet at the base of the tuberosity socket from anterior to posterior; the 4 suture ends (two ends of two sutures of various colors) are thread through the eyelet, and the pin is withdrawn out the skin of the posterior forearm with the elbow in 90� of flexion. Once the button clears the posterior cortex, the opposite suture is tensioned to flip the button on to the posterior cortex; this strategy of button passage may be facilitated with fluoroscopic steerage. The most typical current method is either a transverse or longitudinal (Henry) 3�5 cm incision anteriorly over the antecubital fossa to retrieve the biceps tendon. Bunnell-type or other operating grasping sutures are used to secure the distal end of the tendon. The tendon is drawn into the defect and the sutures are tied with the forearm in neutral or supination B is made over the instrument tip. With the forearm in maximal pronation, this posterior incision is carried down to the radial tuberosity by splitting the extensor muscle mass and supinator consistent with their fibers. A bur or osteotome is then used to make a cavitary opening in the tuberosity massive sufficient to cross the tendon via. Small drill holes are then made alongside the margin of the cavitary opening unicortically, one for each Bunnell strand. The Endobutton is secured to the tendon, and passing sutures are positioned by way of the posterior cortical tunnel prepared for tendon passage; (B) the tendon with Endobutton, ready to be pulled via the tunnel by use of the passing sutures as kite strings; (C) Lateral postoperative radiograph. Note the anterior cortical tunnel and the Endobutton securely seated 230 Chapter Stiff Elbow Vidisha S Kulkarni, Madhura Kulkarni Introduction Elbow is a secure, congruent and complex hinge joint. Inadequately, mounted fractures of the distal humerus are immobilized within the splint postoperatively to compensate for insufficient or improper stability. Treatment by quack or therapeutic massage, injures the already injured gentle tissues leads to fixed contractures and heterotopic ossification. Functional arc for elbow is 30� flexion up to 130� flexion and 50� of pronation supination each affected person can adapt to carry out every day activities of life even when fastened flexion deformity is 70�. Flexion is probably the most required perform so loss of flexion is poorly tolerated than lack of extension. Even 50% much less of movement impairs elbow by as a lot as 80% when terminal flexion is restricted. The severity of stiffness is graded as follows primarily based on the functional arc: � Verysevere: <30 of useful arc. Contractures are also frequent in inflammatory diseases, degenerative diseases or septic arthritis. Tuberculosis in addition to rheumatoid arthritis affecting elbow is another cause of ankylosis. Stiffness because of heterotopic ossification is seen in head harm patients and paralytic contractures are seen after cerebral vascular accident. It is because an intra-articular effusion causes the joint to assume a position of flexion to maximize capability and minimize pressure. Acquired Contractures � Burns � Trauma � Intra-articular fractures of distal humerus � Elbow dislocation � Surgery � Prolonged immobilization � Infection � Rheumatoid arthritis � Tuberculosis, etc. Contractures are additional classified2 as the following: � Extrinsic: Stiff elbow with no identifiable intra-articular pathology, relatively normal articular surfaces and alignment. Trauma Injury about the elbow usually involves trauma to brachialis muscle because it crosses anterior capsule. The damaged brachialis undergoes scarring which tethers to the normal capsule hindering motion. Early mobilization of the elbow joint should be started which sadly is deferred until 6 weeks after surgery. Intrinsic contractures involve intra-articular adhesions, malunions, avascular fragments, loss of cartilage, and so forth. It is seen secondary to intra-articular fractures, bony avascular changes with lack of cartilage. Irrespective of cause all stiff elbows have contracted capsule, secondary contractures develop in ligaments, muscle tissue. Static3 components of ankylosis constitute contractures of capsule, ligament or muscle, heterotopic ossification inflicting impingement or bridging, articular floor scarring, osteophytes, incongruity, and adhesions. Dynamic parts of contracture constitute muscles like, brachialis common extensor tendon, common flexor tendon, hypertonia or limited excursion across the joint. Even 50% loss of movement impairs the elbow function as a lot as 80% each time the terminal flexion is restricted. Continuous passive motion and adjustable static kind of splints are very helpful in attaining a plastic deformation of soppy tissues through stress relaxation. It is necessary to observe any prior an infection, pores and skin incision, scar neurological damage, and so on. We prefer open release due to the number of issues related to arthroscopic launch. Risk of neurovascular damage is more with arthroscopic release and decreased intracapsular quantity sometimes could not allow entry of scope. Pathophysiology Any immobilization post-trauma or post-surgery permits distension of the joint capsule in the place of most capacity, i. Because of immobilization the stress within the surrounding muscles enhance and the muscle tissue fibers bear shortening and contractures within a brief interval. Sometimes improper reduction and malunion of distal humeral fractures obliterates the distal humeral articular anterior tilt which is necessary for clearance of the coronoid course of leading to restricted flexion past 90� postoperatively. Extension lag or terminal restriction of extension is seen generally as a result of place of maximum capability assumed by the elbow. StageI: Bleeding happens inside minutes to hours after trauma and ends in distension of the joint capsule and swelling of periarticular tissues. High hydrostatic stress in the joint and stiff tissues will end in pain and elevated resistance to movement. This loosely organized tissue turns into increasingly strong with deposition solid extracellular matrix.
Discount bystolic expressInaccurate discount of the fracture with incongruity within the articular surface may end in early osteoarthritis of the elbow and have detrimental results at the proximal radioulnar joint pulse pressure deficit generic 5mg bystolic with visa. In addition, fixation have to be secure enough to permit early mobilization to keep away from vital elbow stiffness. Open discount and internal fixation utilizing one of the a quantity of strategies described right here on this chapter. Used in neutralization mode for fixation of indirect fractures with interfragmentary screws. Screw can nevertheless lead to extreme compression,7 notably in osteoporotic bone. Oblique fractures Intramedullary Nailing Intramedullary nails have been developed for fixation of olecranon fractures. Their benefits included minimally invasive method, much less soft-tissue irritation and lower rates of implant removal as compared to tension band wiring. Alternative measures like proximal fragment excision and triceps advancement can be used if attainable. Complications: � Triceps weakness because the blood provide of the tendon is affected � Posteromedial elbow instability12,thirteen � Increased vulnerability of the ulnar nerve to trauma. Anterior transposition of the nerve is sometimes beneficial with the index process. In complicated fractures malunion happens secondary to improper reduction or inadequate fixation. Intra-articular malunion results in fast joint degeneration and symptomatic arthritis. Extra-articular malunion at the metadiaphyseal junction can result in radial head subluxation and posterolateral instability requiring corrective osteotomy. Arthritis Arthrosis is often the end result of inaccurate reduction with articular step-off of two mm or higher. Loss of Motion An common lack of 10�15% terminal extension in comparability with the contralateral aspect is to be expected following olecranon fractures, and sufferers should be endorsed as such. Instability and Subluxation Malreduced Monteggia fractures, unreduced coronoid fractures and proximal fragment excision can result in postoperative subluxation and instability. Postoperative Regime An preliminary posterior plaster slab with the elbow flexed to 90� helps handle quick postoperative ache and can be discontinued after 5�7 days and extended up to 2 weeks with a rigidity band assemble when a detachable splint is supplied. If the soundness of the fixation is a priority, then a hinged fracture brace can be utilized to provide extra help. With triceps advancement, immobilize the elbow in 45� of extension for 4 weeks and progressively permit 10� of further flexion each week. Symptomatic Hardware and Infection Symptomatic hardware issues are the most typical complication after fixation of olecranon fractures. Tension band assemble has been discovered to be equally irritating as plate fixation with charges of removing starting from 20% to one hundred pc. Results and Outcome Outcomes after olecranon fracture are usually good to excellent, with restoration of normal or near-normal perform in additional than 1436 References TexTbook of orThopedics and Trauma nical comparison with tension band wiring. The therapy of olecranon fractures by excision or fragments and repair of the extensor mechanism: historical evaluate and report of 12 fractures. Safe zone for anterior cortical perforation of the ulna throughout tension-band wire fixation: a magnetic resonance imaging analysis. Ulnar nerve palsy on the elbow after surgical remedy for fractures of the olecranon. Current concepts in the remedy of fractures of the radial head, the olecranon, and the coronoid. Biomechanical comparison of interfragmentary compression in transverse fractures of the olecranon. Biomechanical evaluation of fixation of comminuted olecranon fractures: one-third tubular versus locking compression plating. Comparison of olecranon plate fixation in osteoporotic bone: do present technologies and designs make a distinction New intramedullary locking nail for olecranon fracture fixation-an in vitro biomecha- 12. Residual deformity and impairment results in poor practical outcomes4-6 and this prevents return to pre-accident occupation leading to monetary difficulties and reliance on welfare systems. The aspect predominantly concerned in sideswipe accidents is dependent upon the aspect of road where driving is allowed in that specific area. Management of these accidents is tough and entails a multidisciplinary strategy using orthopedic, plastic and vascular surgeons. With the advent of newer antibiotics, trendy surgical methods and numerous gentle tissue coverage procedures, limb salvage is feasible in most cases, but an algorithmic method must be adopted and a number of procedures could additionally be required to obtain useful results. Pathology After understanding the mode of harm, one can easily visualize the probabilities of the injury, which can range from a number of mere scratches to a most critical and disabling traumatic amputation. In most circumstances, nevertheless, a badly mutilated forearm and elbow results, with compound fractures of the bone around the elbows as well as an avulsion loss of soft tissues, together with blood vessels and nerves. The issues related to sideswipe accidents are: � Multiple fractures and dislocations across the elbow � Skin loss and delicate tissue harm and � Injury to the nerves and vessels. There is all the time a comminuted fracture of the distal humerus and the olecranon at coronoid degree, anterior dislocation of the higher end of the each bones of forearm, fracture of shaft of ulna and a fracture of the mid-shaft of humerus. This is adopted by careful planning and a staged surgical protocol to be able to maximize functional outcomes. All sufferers must be given intravenous antibiotics at their arrival to the emergency. As majority of them are compound fractures initial treatment follows the usual management practices for open fractures. However skeletal stabilization was not carried out (8 months postinjury) 1438 TexTbook of orThopedics and Trauma External fixation can be used in sufferers with marked comminution of the fractured bones, bone loss, and multisystem accidents in accordance with the rules of injury management orthopedics. Articulated external fixator has been used as a substitute for transfixation in circumstances of advanced elbow trauma. Wherever attainable, the vessels could additionally be repaired or a venous graft could also be used to obtain revascularization. Debridement of the Wound the wound is totally debrided and prophylactic antibiotics administered. In all cases of high power trauma the wound ought to ideally be debrided inside 6 hours of the traumatic occasion. A thorough lavage helps to remove the contaminants and thereby minimizes the risk of infection. In the absence of infection, delayed closure of the wound may be carried out after about one week which may be aided by split or full thickness pores and skin grafts depending on the need for coverage. Early wound coverage with skin grafts and flaps is preferred so as to decrease an infection, tissue edema and tissue dying and permit early mobilization.
Purchase discount bystolic on lineLoose our bodies and osteophytes from the coronoid tip and the anterior humerus are removed utilizing an arthroscopic burr heart attack vol 1 pt 4 discount bystolic 2.5 mg overnight delivery, via a lateral portal. The posterior compartment is then entered and osteophytes from the olecranon tip and the fossa are equally excised. If a capsular launch is to be performed for loss of extension, we preferentially start in the posterior compartment to keep away from significant swelling creating after the anterior capsule has been excised. The thickened anterior capsule could be then excised taking care to keep away from injury to the radial nerve because it lies anterior to the radial head. If the patient has loss of flexion the anterior compartment is debrided and loose bodies eliminated after which the posterior compartment of the elbow is entered and the capsule excised from the posterior humerus. The medial and lateral gutters are inspected, with particular care to avoid the ulna nerve on the medial aspect, and again loose bodies are removed if current. If a significant improve within the range of elbow movement is anticipated launch or anterior transposition of the ulna nerve is obligatory as with out it ulna nerve signs are likely to occur postoperatively. A cumbersome dressing is utilized and, if there have been significant will increase in vary of motion achieved, steady passive movement may be employed. Arthroscopic debridement of elbow joint has proven encouraging results when it comes to pain relief and enchancment of range of movement. The technique permits removing of free bodies, excision of osteophytes and resection of the thickened olecranon fossa membrane. Their outcomes showed discount in ache, although no important enchancment in vary of motion was famous. Adding anterior and posterior capsular releases has been advocated to enhance range of motion. Acute exacerbations of pain are associated with mechanical symptoms of locking, which outcome from single or multiple loose our bodies within the joint. Pronation and supination of the forearm while gripping can exacerbate the signs as a outcome of degenerative modifications within the radiocapitellar joint. Patients with inflammatory arthritis complain of swelling, pain, loss of movement and deformity. These patients might have related indicators and signs in different joints as a outcome of the systemic nature of the condition. These patients are sometimes on illness modifying medications and this should be famous in drug history. These could present osteophyte formation on the tip of the coronoid and olecranon processes and around the radial head. Radiocapitellar narrowing with preservation of the ulnotrochlear articulation is attribute of primary osteoarthritis. Generalized joint house narrowing is more obvious in early stage rheumatoid arthritis leading in later levels to subluxation or ankylosis of the joint. Treatment Options There is a task for conservative therapies in early elbow arthritis. This could involve oral medicine, often steroid injections, physiotherapy and, at occasions, splintage. Various surgical remedy options can be found when conservative measures fail and although any of these may be indicated for an individual affected person, the options can broadly be divided into these most suitable for degenerative and post-traumatic issues and people more acceptable for inflammatory illness. Surgical Management of Osteoarthritis of the Elbow A variety of surgical choices are available and the kind of surgery is principally decided by the severity of arthritis and the expertise of the surgeon. The options embrace elbow arthroscopic debridement, open surgical debridement, ulnar nerve surgical procedure and eventually whole elbow arthroplasty. Arthroscopic Debridement this is changing into extra popular among surgeons however is technically demanding and requires appropriate training. It requires good information of elbow anatomy and particularly the location of the neurovascular buildings. The approach is beneficial for the removal of osteophytes, loose our bodies, launch of the capsule and radial head excision. It can also be used to carry out the Outerbridge-Kashiwagi process (ulnohumeral arthroplasty). The benefits of Open Surgical Debridement Procedures Outerbridge-Kashiwagi method/ulnohumeral arthroplasty: the Outerbridge-Kashiwagi (O-K) procedure modified by Morrey, and termed the ulnohumeral arthroplasty is a helpful procedure in delicate the arThriTic elbow to moderate elbow arthritis. The procedure enables the removing of unfastened our bodies, excision of osteophytes and fenestration of the thickened olecranon fossa membrane. Procedure: the operation is carried out with the patient supine, a sandbag under the ipsilateral scapula and the arm throughout the chest. With tourniquet control a midline incision is made from the tip of the olecranon extending proximally for 8 cm. This is opened and free our bodies within the posterior compartment of the elbow are eliminated. Osteophytes on the tip of the olecranon and around the olecranon fossa are excised. The floor of the olecranon fossa is then fenestrated using a bone trephine the scale of which is determined by the diameter of the olecranon fossa. A window is produced into the anterior compartment of the elbow enabling anterior unfastened bodies to displace into the fenestration by elbow flexion and extension hence achieving their removing. It can additionally be possible to function via the fenestration excising osteophytes at the tip of the coronoid and partially releasing the tight anterior capsule. Symptoms were noted to recur in 20% at 10 years with recurrence of radiographic changes in up to 50% at 5 years. At a imply follow-up of 33 months, Morrey13 found utilizing the Mayo elbow performance score that 12 of his 15 sufferers had both a wonderful or good outcome (80%). It is normally carried out by way of a lateral method (lateral column) but a medial column procedure may also be undertaken significantly if the ulnar nerve requires decompression or transposition. Procedure: the operation is carried out under general anesthesia with the patient supine and with the arm across the chest. A lateral incision is normally used but if the elbow is very stiff a posterior incision is most well-liked as it will enable medial and lateral pores and skin flaps to be developed to find a way to achieve entry to both the lateral and medial sides of the joint. The brachialis muscle is separated from the capsule utilizing a periosteal elevator after which the anterior capsule is excised. Loose bodies throughout the anterior compartment and osteophytes are additionally removed at this stage. If restricted, extension is still vital; a medial column method may be performed to be able to resect the anteromedial capsule. Less incessantly, loss of flexion is a priority and is often due to adhesions and scarring throughout the posterior compartment of the elbow joint. Treatment includes elevating the triceps, excising the posterior capsule and removing any posterior unfastened bodies and osteophytes. Mansat and Morret reported the outcome on 38 sufferers who had undergone surgery for elbow stiffness at a mean of 43 months postoperatively.
Buy genuine bystolic onlineCompression rotation test: the supine patient abducts his shoulder 90� blood pressure control chart discount bystolic 5mg on line, preserving the elbow flexed 90�. Clinical Presentation History Patients current with shoulder ache, which can be anterior, posterior and even sick defined. A related check carried out with the patient in upright position and arm elevated to 160� within the scapular plane is termed the crank check. Now with the arm in the same position the palm is fully supinated and the maneuver is repeated. Pain from this take a look at can be elicited because the contraction of biceps tendon will increase pressure on the superior labrum. Range of movement: Overhead athletes have lowered internal rotation in their dominant arm. These exams have various of sensitivity and specificity within the prognosis of superior labral injuries. One line represents the sublabral recess whereas the second defines the labral tear � An irregular or laterally curved area of excessive signal depth in the posterior third of the labrum. Besides an intensive examination of the superior glenoid labrum, it could be very important search for varied anatomical variations like sublabral recess and Buford complex. There can also be a optimistic drive through signal in which the scope sheath can simply be handed superior to inferior. In patients with sort I tears the torn and frayed labral tissue is debrided back to intact labrum, carefully preserving the attachment of labrum and biceps tendon to the glenoid. On the contrary giant vascular fragments may be abraded and repaired with sutures by all inside repair method. Small and unstable fragments are debrided whereas bigger (>50% thickness) are repaired with fixation methods. Lightly abrade superior rim of glenoid neck adjacent to the articular cartilage and freshen the bone beneath biceps labral complicated. Through the anterosuperior cannula a suture anchor is inserted in the superior glenoid tubercle just under the biceps tendon. One limb of the suture is retrieved out of the mid-anterior cannula with a crochet hook. A fowl beak type of tissue penetrating cum suture retrieving instrument is inserted by way of the superior labrum simply posterior to the biceps tendon. The suture limb retrieved out of the mid-anterior cannula is grasped with this instrument and retrieved through the labrum and out of the anterosuperior cannula. Either a easy suture configuration or mattress suture configuration could also be used. A sliding knot is tied and using a loop deal with knot pusher this knot is tightened. Three additional alternating half hitches are tied together and locked in order to complete the repair. My preference typically is an easy suture posterior to the biceps tendon first, adopted by a mattress suture at the biceps tendon region. Establish the three standard anterior and posterior arthroscopic portals (anterosuperior simply behind the biceps tendon, and mid-anterior just above subscapularis tendon). Proper placement of the anterosuperior portal is critical to the success and ease of the process as a result of both suture placement and drill positioning are carried out via this portal. A spinal needle is used to take a look at the portal place earlier than institution of this access website. When proper place is decided, an outside-in method is used to establish this portal. Debride degenerative labral and biceps tissue to expose the superior glenoid neck. Postoperative Rehabilitation the affected person is positioned in a sling that he can take away for full extension of elbow. Patients are instructed to avoid external rotation of shoulder past impartial and extension of arm behind the physique, with the elbow extended for a period of four weeks. The shoulder sling is discontinued after 4 weeks and physiotherapy with mild energetic and passive workouts restricted to 90� of flexion, 70� of adduction and 0� exterior rotation. Usually sufferers take 6 months postoperatively to contain of their sports activities. Clavicle fractures accounts for roughly 35�40% of fractures within the shoulder region. It derives the name from the Latin word for key clavis and clavicula referring to the musical image similar to its shape. The medial progress plate of the clavicle is responsible for almost all of the expansion (80%). The clavicle being an S-shaped spiral bone the stress concentrates on the junction of the center and distal third which supplies method. The distal section is pulled downward by the burden of the arm and inward by the pull of the pectoralis major and latissimus dorsi. The proximal fragment is pulled upward by Functions of the Clavicle and Anatomy the clavicle serves as a bony link from the thorax to the shoulder. The clavicle is an S-shaped bone and has an anterior convex to concave curvature when considered from medial to lateral. The lateral finish of the clavicle flattens whereas the medial end stays cylindrical. Because the sternoclavicular ligaments are extremely strong the force exits the clavicle in the midshaft the sternomastoid. In either case as the sternoclavicular joint is intact, the posteriorly directed drive on the whole shoulder or scapula itself might bend or break the clavicle over the fulcrum of the primary rib. Classification the fracture of clavicle is assessed according to the location of fracture. Type 2: Coracoclavicular ligament disrupted permitting superior displacement of lateral fragment. TexTbook of orThopedics and Trauma Treatment Lester, in 1929 has reported 104 forms of therapy of fracture clavicle. A figure-of-8 bandage with splint or a "jacket" solid can be a perfect method of immobilization of this fracture. Anderson in contrast the figure-of-8 with the sling and swathe for the treatment of these fractures. The figure-of-8 also presses the proximal fragment backward and exaggerates the deformity. The jacket solid provides more pain aid, and the patient joins his or her work earlier, although it could be heavier and slightly uncomfortable to the affected person. They concluded that the useful and cosmetic outcomes of all of the methods are the identical, and also the time required for healing was the same. The affected person is sitting with both the shoulders bracing posteriorly with each the hands pressed on the pelvis.
References - Komodromas T, Lieb D, Baraboutis J. Unusual presentation of a pericardial cyst. Heart vessel. 2004;19:49-51.
- Marshall JC, Christou NV, Horn R, et al. The microbiology of multiple organ failure. Arch Surg. 1988;123:309-315.
- Lewin KJ, Fair WR, Steigbigel RT, et al: Clinical and laboratory studies into the pathogenesis of malacoplakia, J Clin Pathol 29(4):354n363, 1976.
- Ernst, S., Ouyang, F., Linder, C. et al. Initial experience with remote catheter ablation using a novel magnetic navigation system: magnetic remote catheter ablation. Circulation 2004;109:1472-1475.
|


