|
Barry I. Rosenblum, DPM, FACFAS - Assistant Clinical Professor, Surgery
- Harvard Medical School
- Director of Podiatric Surgical Residency
- Beth Israel Deaconess Medical Center
- Boston, Massachusetts
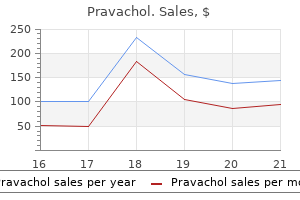
Pravachol dosages: 20 mg, 10 mg
Pravachol packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills

Discount pravachol 10 mg without prescriptionPlacing the affected person in traction with Gardner-Wells tongs cholesterol levels range canada generic 10 mg pravachol fast delivery, for instance, may be extra appropriate for this example. Pin website issues embrace lacerations,fifty five cranium fractures, associated intracranial hemorrhage. Other forms of head assist embrace the horseshoe headrest and the four-cup headrest. Stretch on the brachial plexus may be prevented by placement of an axillary roll barely thicker than the diameter of the higher part of the arm. This roll must be positioned roughly four fingerbreadths beneath the armpit to stop compression of the lengthy thoracic nerve. Failure to place an adequately sized roll may result in excessive stretch of the brachial plexus, with the greatest results on the C5 and C6 nerve roots. The upper extremities need to be supported in relatively neutral positions to stop ulnar neuropathies. Compression of the widespread peroneal nerve can happen because of inadequate padding laterally beneath the knee. Intraoperative Monitoring Various electrophysiologic modalities can be utilized to detect subtle indicators of neurological compromise before they turn out to be fixed deficits. The use of intraoperative monitoring can scale back the chance of serious neurological deficits within the acceptable circumstances. Some positioning issues may be averted with the concomitant use of intraoperative monitoring. We have discovered excellent correlation between the shortage of modifications in evoked potentials and affected person outcome. However, in procedures with a possible for vital danger to the twine or neural constructions, neurological monitoring is a helpful adjunct to the surgeon. The four-cup headrest is a wonderful alternative to the horseshoe, though blindness, skin and scalp compression, and irregular cervical movement are attainable with both assist. This complication happens more incessantly with longer procedures and when the spine is extra flexed for facilitation of the surgical strategy. Such edema may be prevented by minimizing the amount of fluid given by the anesthesiologist and by placing the patient barely more in a reverse-Trendelenburg position to elevate the pinnacle relative to the heart. Facial edema can result in lingual or laryngeal edema and resultant airway obstruction. If obstruction occurs, the patient ought to be kept intubated until the edema has improved or resolved. Premature attempts at extubation may find yourself in hypoxia and may necessitate emergency tracheotomy. Surgeons should immediately seal the portals of entry with bone wax, electrocautery, and full-field irrigation. Repositioning the affected person in the left lateral decubitus position may facilitate elimination of air from the right atrium. Pulmonary embolism, however, is believed to subsequently occur in 15% of such sufferers. Doppler ultrasonography and impedance plethysmography are helpful in detecting proximal venous thrombosis and are the mainstay of analysis, with sensitivities exceeding 90%. Early mobilization of postoperative patients is necessary in stopping thrombus formation. In addition, enoxaparin and heparin have been proven to be equally secure and efficient. Air travels from the pinnacle down the venous system to the guts and eventually to the lungs, the place pulmonary constriction and pulmonary hypertension ensue, or in sufferers with a right-to-left coronary heart shunt, paradoxical air embolism might happen. Peripheral resistance decreases, and cardiac output initially increases to compensate and maintain blood stress. Later, as the volume of air infused will increase, cardiac output drops, as does blood stress. Monitoring strategies and devices used to detect emboli embrace precordial Doppler ultrasonography, capnography or mass spectrometry, transesophageal echocardiography, transcutaneous oxygen, esophageal stethoscope, and proper coronary heart catheter. Because no single monitor is completely reliable, two or extra must be used concurrently. In subarachnoid hemorrhage sufferers, aneurysms must be secured before initiation of pharmacologic prophylaxis. Management choices embrace full-dose heparinization or inferior vena cava interruption. Treatment with intravenous heparin (target partial thromboplastin time of forty five to 60 seconds) is followed by oral warfarin sulfate (target worldwide normalized ratio of 2) when not contraindicated. Anticoagulation should be continued for six weeks to 3 months in uncomplicated cases. Patients experiencing pulmonary embolism complain of pleuritic chest pain, hemoptysis, and dyspnea. Jugular venous distention, fever, rales, tachypnea, hypotension, and altered mental standing may be discovered on physical examination. Arterial blood gasoline willpower reveals a Po2 of lower than 80 mm Hg in 85% of patients, accompanied by a widened alveolar-arterial gradient. In sufferers with large embolism, proper axis deviation, right ventricular strain, or proper bundle department block may be recognized on electrocardiography. The whole medical scenario, including affected person examination, laboratory outcomes, and radiographic analysis, results in the prognosis. Patients with an enormous, life-threatening embolus, nevertheless, ought to be fully anticoagulated regardless of the risk for intracranial hemorrhage. This subset of sufferers often requires ventilatory assist and vasopressor remedy to guarantee enough oxygenation and blood strain. Because thrombolytic remedy with urokinase or streptokinase has a higher threat for problems than does treatment with heparin, with no significant enchancment in end result, these modes of therapy have largely been deserted. When all else fails, pulmonary embolectomy could also be carried out as a lifesaving measure. Patients about to endure neurosurgery ought to, when medically suitable, avoid the utilization of aspirin merchandise within the week earlier than surgery and different nonsteroidal anti-inflammatory brokers on the day earlier than surgery. Wound Complications Because of the vascularity of the scalp, most cranial wounds heal nicely. Several potential problems associated to the wound area and wound closure can be anticipated and prevented. Postoperative drainage can also be advantageous in sufferers in whom postoperative anticoagulation could additionally be required because some of these sufferers have slightly delayed hematoma formation. It is greatest to hold a drain within the submuscular space throughout this time to forestall a postoperative seroma that may turn into infected. Recent pointers for an infection prevention advocate prophylactic antibiotics 1 hour earlier than incision and 24 hours postoperatively.
Purchase 20 mg pravacholThere are con flicting information regarding increased complication charges in neuro genic patients and whether concomitant bladder augmentation increases infection unesterified cholesterol definition purchase pravachol 10 mg. Failures of more conservative remedy or devastation of the bladder outlet from persistent indwelling catheters or prior surgical intervention could be managed with closure of the bladder outlet and supravesical urinary diversion. Bladder neck closure can be performed utilizing vaginal, abdomi nal, or combined surgical approaches. In the setting of bladder outlet failure, diversion is used as a final resort for patients with refractory incontinence from either endstage bladder dys perform or complete outlet devastation. By serially emptying the bladder at common mounted intervals, often between four and 6 hours, sufferers could preserve freedom from the nuisance and complications of indwelling cath eters. If leakage happens between catheterizations, the frequency may be increased and anticholinergics could be added. The clear approach, popularized by Lapides, includes washing the catheter and arms with soap and water rather than sterility. The Foley catheter and suprapubic cys tostomy tube are useful within the management of detrusor areflexia and are sometimes useful within the management of acute neurological injury. The suprapubic tube (surgically placed in an infraumbilical position) can keep away from the issues of urethral erosion, epi didymitis, orchitis, prostatitis, and urethral stricture and is often extra comfortable and manageable for the affected person as compared to a Foley (urethral) catheter. However, indwelling catheters of either sort have been shown to be inferior to intermittent cath eterization strategies when it comes to charges of bacteriuria and urethral problems. It has been suggested that, after eight years of an indwelling catheter, the danger for malignancy is such that annual endoscopic surveillance of the bladder ought to be performed. To be successful, the abdom inal pressure generated should overcome outlet closure forces. Patients should be checked for hydronephrosis as a end result of the increased voiding stress could additionally be transmitted to the higher tracts, particularly in sufferers with already impaired compliance. Bethanechol is a cholinergic agonist that may be anticipated to improve bladder contractility. The use of sacral neuromodulation, talked about previously for refractory detrusor overactivity, has proven benefit in stimulating detrusor contraction within the setting of continual nonneurogenic, nonobstructive urinary retention. In a randomized potential trial, 83% of sufferers who obtained a permanent implant had improvement of their signs, with 69% of handled patients capable of discontinue intermittent catheter ization. An alternative to steady bladder drainage with urethral or suprapubic catheters is urinary diversion, which can present a ten Failure to Empty Urine (Retention) Urinary stasis can predispose to urinary tract infection, overflow incontinence, and elevated bladder stress. The targets of deal with ment include both rising bladder contractility, decreasing outlet closure pressure, or otherwise emptying the bladder intermit tently or continuously. Management of these sufferers relies on a selection of factors, most notably the flexibility to catheterize, the presence of autonomic dysreflexia, elevated bladder storage pressure, and incontinence. If left untreated, patients with detrusor�external sphincter dys synergia could have reflux, upper tract injury, worsening bladder compliance, and finally renal failure. Destruction of the sphincter mechanism produces complete urinary inconti nence that could be managed with external condom catheters. Although the outcome will be low bladder stress and low outlet resistance, the process is related to the problems of hemorrhage and stricture and has a high rate of failure to relieve outlet obstruction. Prosthetic stent placement throughout the exter nal sphincter can produce an effect just like that of sphincter otomy by eliminating outlet obstruction. In the instant postoperative period, surgical issues such as bleeding and failure are much less frequent. However, the longterm issues of stent migration, encrustation, and stenosis can produce unsat isfactory outcomes. Direct injection of botulinum toxin A into the external sphincter can provide a minimally inva sive and secure different to surgical ablation. Similar to other outlet reduction procedures, botulinum toxin A injection decreases intravesical strain, improves urinary retention, and decreases autonomic dysreflexia. Food and Drug Administration, is associated with important expense for the affected person, and requires reinjection every three to 9 months. Adrenergic blocker medications can promote bladder smooth muscle rest on the level of the bladder neck. Cystoscopic incision of the bladder neck with elec trocautery can also defunctionalize the internal sphincter. Botulinum toxin A within the overactive bladder: present standing and future instructions. Epidemiology and threat components for urinary tract infection in patients with spinal cord damage. Botulinum toxin A (Botox) intradetrusor injections in adults with neurogenic detrusor overactivity/ neurogenic overactive bladder: a scientific literature review. Clean, intermittent self catheterization in the remedy of urinary tract disease. Current practice patterns in the urologic surveillance and administration of patients with spinal wire damage. Effect of bladder administration on urologi cal complications in spinal twine injured sufferers. The price to the United Kingdom National Health Service of managing erectile dysfunction: the impact of sildenafil and prescribing restrictions. Sympathetic exercise within the proximal urethra in patients with urinary obstruction. Practical information to diagnosis and followup of patients with neurogenic bladder dysfunction. The effect of nifedipine on cystoscopyinduced autonomic hyperreflexia in patients with high spinal twine accidents. Assessment of bladder operate after lumbar decompressive laminectomy for spinal stenosis: a potential study. Urodynamic findings in youngsters with myelomeningocele after untethering of the spinal twine. The effects of detethering on the urodynamics profile in children with a tethered twine. Clinical, urodynamic and neurophysiological findings in sufferers with neuropathic bladder because of a lumbar intervertebral disc protrusion. Control of detrusor hyperreflexia by the intravesical instillation of oxybutynine hydrochloride. Role of adrenoceptor subtypes in mediating rest of the pig bladder trigonal muscle in vitro. Phase 3 efficacy and toler capability examine of onabotulinumtoxinA for urinary incontinence from neurogenic detrusor overactivity. OnabotulinumtoxinA for the remedy of patients with overactive bladder and urinary incontinence: outcomes of a phase three, randomized, placebo controlled trial.
Purchase 20 mg pravachol amexC cholesterol levels ratio calculator order 10 mg pravachol mastercard, Cerebrospinal fluid could be seen welling up via the foramen of Luschka (center). On the neuronal organization of the acoustic center ear reflex: a physiological and anatomical research. Quantitative evaluation of electrically evoked auditory brainstem responses in implanted youngsters with auditory neuropathy/dyssynchrony. Diagnostic functions of impedance audiometry: Middle ear disorder, sensorineural dysfunction. Acoustic reflex take a look at in neuro-otologic prognosis: a evaluate of 24 instances of acoustic tumors. Electrophysiological results of inserting cochlear implant electrodes in a perimodiolar position in younger youngsters. The mismatch negativity cortical evoked potential elicited by speech in cochlear-implant customers. Observations on the generator mechanism of stimulus frequency acoustic emission-two tone suppression. Translabyrinthine approach to the cerebellopontine angle and internal auditory canal. A crucial review of the neurophysiological proof underlying medical vestibular testing using sound, vibration and galvanic stimuli. Test-retest reliability and age-related traits of the ocular and cervical vestibular evoked myogenic potential tests. Vestibular migraine (patient video describing symptoms before and after remedy with Topamax). Right perilymph fistula not superior canal dehiscence (patient video describing signs before and after surgical repair). Right perilymph fistula: dizziness, migraine complications and cognitive dysfunction (patient video describing symptoms before and after surgical repair). Perilymph fistula (patient video describing signs before and after repair of traumatic perilymph fistulae). Value of skull radiography, head computed tomographic scanning, and admission for observation in instances of minor head injury. Endoscope-assisted surgery of the trigeminal, facial, cochlear or vestibular nerve. Cochlear implantation for auditory rehabilitation in Camurati-Engelmann illness (hereditary diaphyseal dysplasia). Intraoperative assessment of cochlear implant and auditory brainstem implant system perform. A detailed historical past and physical examination, together with a neurological examination, are essential for assessment, accurate analysis, and treatment of urologic conditions resulting from neurological illness. Additional diagnostics, corresponding to laboratory testing and numerous radiologic studies to evaluate the upper and lower urinary tract, often require evaluation. Ultimately, ongoing reassessment at regular intervals can be necessary to forestall progression of urologic illness in these sufferers. Urinary issues of neurological disease or injury can affect the filling/storage or emptying phases of micturition, or can impression both phases. The deficits are usually depending on the area of the nervous system concerned within the disease and may be grouped into supraspinal lesions, spinal lesions, suprasacral wire harm, and illness at or distal to the sacral spinal twine. Although important variability exists inside a given disease entity, characteristic symptom patterns and urodynamic findings are widespread, depending on the level or location of the lesion. Once a analysis of the neurological or neurosurgical illness has been established and the neurourologic disturbance recognized, consideration must be given to the short- and long-term treatment of signs and prevention of long-term issues. There are four basic goals in bladder administration: (1) protecting renal perform and upper urinary tracts, (2) minimizing lower urinary tract complications, (3) treating the bothersome signs of neurourologic illness, and (4) selecting a administration program appropriate with individual affected person goals and abilities. To obtain these targets, therapy should give consideration to upkeep of low storage pressure, prevention of incontinence, promotion of efficient bladder emptying, and avoidance of infection. Because of the difficult and variable symptomatology of neurourologic issues, administration can be more easily divided into categories of lower urinary tract dysfunction somewhat than remedy of particular disease entities. Appropriate recognition and well timed management of urologic issues related to neurological situations are important to keep away from potentially irreversible opposed outcomes. The lower urinary tract has two primary physiologic features: low-pressure storage of enough volumes of urine with applicable sensation and periodic, voluntary expulsion of urine from the bladder in a coordinated and full trend. To provide these capabilities, the bladder, bladder neck, exterior urethral sphincter, and urethra will must have coordinated exercise mediated by the autonomic and somatic nervous methods. When evaluating a affected person with urologic problems secondary to a neurological situation, a radical neurourologic evaluation Renal ultrasound demonstrating hydronephrosis in a affected person with a neurogenic bladder and poor bladder compliance. The arrow identifies areas of distention of the renal pelvis, calyces, and proximal ureter. Note the preserved renal parenchyma surrounding the calyces, a finding suggesting preserved renal function. Activation of adrenergic receptors inside the wall of the bladder supplies inhibition and leisure of the detrusor muscle. Activation of cholinergic receptors stimulates the detrusor to contract, primarily through the M3 muscarinic receptor subtype. Additional neurotransmitters, including nitric oxide, adenosine triphosphate, and neuropeptides, even have a proposed modula tory position in bladder leisure and contraction. Adrenergic receptors predominate in this area, and stimulation of postgan glionic adrenergic receptors provides excitatory input to the trigone, bladder neck, and proximal urethra that ends in increased bladder outlet closure pressure. Afferent (sensory) transmission of lower urinary tract stimuli travels through the pelvic, hypogastric, and pudendal nerves to the dorsal root ganglia of the lumbosacral spinal twine. The pelvic nerve afferents monitor the volume of the bladder and the ampli tude of bladder contraction through myelinated (A) and unmyelin ated (C) fibers throughout the bladder wall. The unmyelinated fibers are also implicated in the transmission of urgency and ache. The proximal 2 to three cm of the urethra in both men and women is primarily sphincteric. In males, the prostatic glan dular and fibromuscular stroma tissue surrounding the proximal urethra can affect voiding through extrinsic compression and obstruction. There is a excessive density of adrenergic receptors that, when stimulated, produce a rise in intraurethral strain. The extrinsic muscle consists of primarily fasttwitch muscle fibers and is under vol untary management. The intrinsic muscle tissue, also known as the intrinsic sphincter or the rhabdosphincter, consists primarily of slowtwitch fibers and offers passive urinary continence. Innervation of external sphincter and pelvic floor musculature is primarily somatic from branches of the pudendal nerve. The pudendal nerve pathway begins in the anterior horn cells of the S3 and S4 segments of the spinal cord.
Buy generic pravachol 20 mg onlineThe tectorial membrane extends in a medial-to-lateral direction inside the scala media and above the hair cells cholesterol levels slightly elevated buy discount pravachol, the place the hair cell stereocilia are embedded. Facial nerve injury secondary to temporal bone fracture is discussed on this chapter solely in the context of the cochlear and vestibular nerves, although extra in depth reviews associated to therapy are discussed in Chapters 351, 352, and 355 and supplied in other publications. Understanding the capabilities of the primary afferent neurons constituting the eighth cranial nerve requires information of the complicated structures of the peripheral vestibular and auditory systems. During the embryonic stage, the neurosensory portions of the vestibulocochlear system are derived from ectoderm. With progress and development, these neurosensory epithelial structures turn out to be incorporated inside the petrous portion of the temporal bone and are encased within the otic capsule. Concurrently, the middle ear house develops as an invagination from the primary pharyngeal pouch and comes to lie lateral to the otic capsule. Meanwhile, the external ear develops from the overlying epithelium, and the fundus of its canal abuts the middle ear house at the tympanic membrane. Air vibrations impinge on the tympanic membrane and trigger it and the malleus to vibrate. This physical vibration is transmitted through the incus to the stapes and by means of its footplate to the fluids of the labyrinth. The fluid vibrations produce a stimulus along the basilar membrane that activates the organ of Corti. Impulses are transmitted through the cochlear nerve endings to the cochlear nuclei in the pontomedullary junction. The bony heart, around which the spiral is coiled, assumes the shape of a tapered screw (from the Latin word modiolus) if the outer components of the bony spiral are removed. The relationships of the temporal lobe, inside ear, middle ear, eustachian tube, and pinna. Course and relationships of the facial, vestibular, and cochlear nerves from the pontomedullary junction by way of the temporal bone. Sound waves contact the tympanic membrane, and the acoustic power is reworked and transmitted to the internal ear through the ossicular chain within the middle ear. Hair cell transduction occurs because the basilar membrane containing the organ of Corti moves relative to the tectorial membrane. If sound vibrations were to reach the oval and spherical home windows at the similar time, a sure quantity of the sound would be canceled. The intact tympanic membrane protects the spherical window from direct sound impingement; the tympanic membrane is connected to the oval window through the ossicular chain, which makes direct transmission by this route sooner; and the round window membrane faces backward, at proper angles to the airplane of the tympanic membrane, and is recessed inside the niche. These factors delay the impingement of sound onto the spherical window membrane, which produces the part difference. As a consequence of these phenomena, a large perforation of the tympanic membrane ends in a hearing loss of 30 to 35 dB by air conduction, whereas dislocation of the ossicular chain with an intact tympanic membrane produces an air conduction lack of about fifty five to 60 dB. TransmissionintheLabyrinth Cochlear sign transduction of high frequencies happens close to the basal portion, and transduction of low frequencies happens near the apical regions of the basilar membrane and the organ of Corti. Detailed mechanisms of sound transduction and notion are beyond the scope of this chapter but may be present in other publications. Because the efficient vibratory area of the tympanic membrane is about 17 instances as massive as the area of the footplate of the stapes, and because the manubrium of the malleus is 1. Anatomy of the inner ear and innervation of the cochlea and vestibular end-organs. Upper left inset, the relationship between the posterior crista and the cupula is demonstrated. Lower left inset, the basal turn of the cochlea is proven, along with the relationships of the scala vestibuli, scala media, scala tympani, and the organ of Corti. The objective of this section is to describe the current, major measures of auditory system perform. Some of these measures depend upon the subjective response of the patient and are referred to as subjective measures of listening to. Other measures require no subjective response from the patient, but the affected person must be quiescent and cooperative. Such goal measures of auditory system operate could be conducted when the affected person is alert and cooperative or when the affected person is sedated or anesthetized. Before improvement of the clinical audiometer, assessment of listening to was usually carried out with tuning fork exams. Each tuning fork emits a pure tone of a specific frequency, relying on the physical traits. An skilled practitioner can activate the fork by striking it with a "normal" blow. Because of issues in reliably striking a standard blow and the noise levels in most scientific examination rooms, tuning forks are extra usually used in a qualitative method to assess the type of hearing loss. A calibrated audiometer is the instrument of alternative for more precisely determining the magnitude and configuration of listening to loss as a operate of frequency. For individuals with regular listening to and people with sensorineural hearing loss, the tuning fork is heard longer by air conduction than by bone conduction because of the advantage supplied to the air conduction sign by the conventional center ear system. However, when the patient hears bone conduction longer than air conduction, a conductive (middle ear) hearing loss is sometimes recommended. This ensues when the air conduction route of transmission is not the more environment friendly path to the cochlea. When both ears are regular or symmetrically abnormal, the auditory signal is localized to the middle of the pinnacle. The tuning fork tests present the inspecting physician with an preliminary impression of the likelihood of listening to loss and the potential web site of the auditory lesion affecting listening to sensitivity. Such data is available from extra formal measures of auditory system function. Pure-tone threshold listening to sensitivity is the subjective process by which auditory sensitivity is set. The output sound pressure degree for standard circumaural or inserted earphones, or each, is specified when measured in a regular coupler, referred to as an artificial ear. The synthetic ear simulates the impedance characteristics of the common human ear on the aircraft of the tympanic membrane. The decibel levels utilized in audiometers for the normal threshold for air conduction can be present in different publications. To decide hearing loss, listening to sensitivity is assessed at octave frequencies between 250 and 8000 Hz. In abstract, pure-tone air conduction testing is the initial and significant measurement for subjective hearing loss. The measure supplies a sign of the magnitude and configuration of the hearing loss as a operate of frequency.
Buy pravachol with a visaWhen the sample is immersed within the sturdy cholesterol lowering diet and lifestyle cheap pravachol 20 mg without a prescription, fixed magnetic area, the spins within the pattern bear a slight polarization. The fee of this precession is a product of the intrinsic magnetic second (the gyromagnetic ratio) of the spin and the energy of the primary magnetic field. Up to this point, the sample has been polarized and excited and a signal detected, however the location of the spins that created the sign remains unknown. Suppose that two objects are within the magnetic subject, each of which create a signal. The resonant frequency of the spins is a function only of the magnetic area at that point in area. Thus the spatial origin of the sign could be decided by the frequency of the received sign. In apply, to determine this, a linear gradient is created that provides to or subtracts from the main subject as a linear function of offset from the origin. The second function is to encode the spatial location of spins to kind the magnetic resonance image. To set up location along the frequency-encoding axis, a gradient is applied in the course of the signal readout time. To encode the orthogonal axis, a gradient is applied someplace between the time of excitation and reception and is called part encoding. One distinctive value of phase encoding is utilized each time that the readout gradient is utilized. The spin of nucleus a creates the magnetic moment of the nucleus, which causes the spin to precess along circle b around magnetic area B0. However, intensity within the voxel also depends on the comfort charges of the spins. After excitation, the magnetization in the slice returns alongside the axis of the primary magnetic field by interaction with other nonmoving hydrogen spins, sometimes those hooked up to large molecules. Slice choice illustrating a bunch of four excited axial slices relative to a affected person. Maximal contrast between structures of interest may be achieved by the appropriate selection of sequence parameters. With the 180-degree pulse included, the decrease is T2, with T2 always being larger than T2*. A single gradient (G) is designed to change the magnetic area alongside just one direction (along the x, y, or z axis). Macroscopic and microscopic field gradients, created by variations within the magnetic susceptibility of tissue, trigger some of the excited spins to precess faster and some slower. Lung parenchyma normally appears hypointense as a result of the T2 of lung tissue is so low that the signal is gone earlier than it could be sampled. The gadolinium atom is strongly paramagnetic and acts to shorten the T1 rest time of nearby water protons in blood. A, Recovery of longitudinal magnetization (Mz) versus time for 3 substances with different T1 values. The spin echo starts with nutation of longitudinal magnetization (Mz) into the transverse aircraft (A). The longitudinal magnetization (Mz) signal regrows from -z to +z at a fee determined by the T1 of the spins. Inversion restoration can be used to enhance contrast between buildings, similar to grey and white matter, or to nullify signals that arise from protons of a recognized T1. The whole k-space matrix must be collected earlier than the images could be reconstructed. The effect is to create image blurring that worsens with rising echo train size or lowering tissue T2. The comparatively lengthy T2 times of tissues within the neuraxis permit echo train length values of 16 to be used routinely. In this case, the sequence is referred to as a gradient echo because a readout gradient is used to type the echo. In this way, the k-space could be crammed very quickly, and the scan can be accomplished in a matter of seconds somewhat than minutes, as is the case with typical spin echo. In a multiple-echo spin echo sequence (not shown here), a single section encoding is applied for all four echoes and every echo fills in the identical sample line in four separate k-space matrices. The sequence must be repeated a selection of instances equal to the decision in the phase-encoding direction of the image. In the quick spin echo sequence, a different part encoding is utilized for every echo of the identical sequence. Inversion recovery sequence displaying both the movement of the spins (A) and a plot of longitudinal magnetization (Mz) versus time (B). Coronal inversion restoration magnetic resonance photographs of a volunteer and a jar of mayonnaise. The nullifying impact of sure T1 occasions on numerous substances is illustrated: T1 of a hundred and ten milliseconds nullifies mayonnaise (Mayo), T1 of 150 milliseconds nullifies white matter, and T1 of 375 milliseconds nullifies grey matter. The flip angle becomes an important determinant of image contrast in gradient echo sequences. Low flip angles (typically 5 to 20 degrees) end in images that are extra T2* weighted, whereas larger flip angles (40 to ninety degrees) result in photographs that are extra T1 weighted. Diffusion-WeightedImaging Diffusion of water within the mind is dependent upon the integrity of the mobile membrane and the osmotic steadiness of the neurons and astrocytes. During restoration and into the continual stage, the loss of cell wall integrity causes the diffusion to enhance. The distinction in B0 area is brought on by the utilized gradient and the whole movement of the spin in that path. The spin precesses at a different price before and after the 180-degree pulse, thereby leading to an accumulated section error at the time of readout and a loss of signal. The farther that the spin wanders (in brownian terms) between gradient lobes, the higher the signal loss. Conversely, when the cells swell and the spin motion is lowered to lower than that of normal tissue, the diffusion loss is lowered to less than that of regular tissue, and the region turns into hyperintense. This sequence is utilized in purposes which are highly sensitive to even minor affected person movements. The readout gradient repeatedly reverses, which fills the k-space matrix in a single excitation. B, Magnetic resonance angiogram of a affected person with an occluded proper center cerebral artery. C, Perfusion picture from the same patient as in B, showing the anticipated hypoperfusion (in blue) in the proper hemisphere.
Purchase pravachol onlineComplications of posterior lumbar interbody fusion when using a titanium threaded cage gadget lower cholesterol without medication quickly order pravachol 10 mg free shipping. The causes of failure of lumbar transpedicular spinal instrumentation and fusion: a prospective research. Complications of anterior approaches to the thoracolumbar spine: emphasis on Kaneda instrumentation. Postoperative neurological deficits in segmental spinal instrumentation: a research using spinal twine monitoring. Management of symptomatic lumbar pseudarthrosis with anteroposterior fusion: a useful and radiographic outcome study. Posterolateral lumbar and lumbosacral fusion with and with out pedicle screw internal fixation. Comparison of anterior and posterior instrumentation for correction of adolescent thoracic idiopathic scoliosis. The function of anterior lumbar interbody allograft bone dowel fusion as an adjunct to posterior segmental lumbar fixation. Posterior plates in the management of cervical instability: long-term ends in 44 sufferers. Internal fixation in lumbosacral spine fusion: a biomechanical and clinical study. Management of pseudarthrosis after arthrodesis of the spine for idiopathic scoliosis. Factors predicting postoperative problems following spinal fusions in kids with cerebral palsy. Efficacy of pedicle screw fixation within the remedy of spinal instability and failed back surgery: a 5-year evaluation. Short segment posterior instrumentation, discount and fusion of unstable thoracolumbar burst fractures-a evaluation of 26 instances. Does anterior plating maintain cervical lordosis versus conventional fusion techniques The position of acute decompression and restoration of spinal alignment within the prevention of post-traumatic syringomyelia: case report and evaluate of current literature. Intraoperative ultrasound for quick analysis of anterior cervical decompression and discectomy. Initial experience with intraoperative magnetic resonance imaging in backbone surgery. A new method to computer-aided backbone surgical procedure: fluoroscopy-based surgical navigation. Frameless stereotactic guided neurosurgery: clinical experience with an infrared primarily based pointer device navigation system. Improving accuracy and lowering errors in spinal surgery-a new technique for thoracolumbar-level localization utilizing computer-assisted picture steerage. Placement of C2 laminar screws using three-dimensional fluoroscopy-based image guidance. A comparability of two strategies in image-guided thoracic pedicle screw placement: a retrospective research of 37 patients and 277 pedicle screws. Miniature robotic steering for backbone surgery-introduction of a novel system and analysis of challenges encountered during the scientific growth phase at two backbone centres. Significantly improved lumbar arthroplasty placement using picture steering: technical note. Traumatic spinal wire harm as a complication to ankylosing spondylitis: an extended report. Spinal cord damage occurring in sufferers with ankylosing spondylitis: a multicenter examine. Fractures of the backbone in ankylosing spondylitis: analysis, treatment, and problems. Management of cervical spinal cord harm in ankylosing spondylitis: the intervertebral disc as a explanation for wire compression. Spinal cord injury, spinal fracture, and spinal stenosis in ankylosing spondylitis. The stabilizing effects of different orthoses within the intact and unstable higher cervical backbone: a cadaver examine. Acute pulmonary edema following removal of a spinal orthosis: an unusual complication of a halo vest. The effect of torque stress on halo pin complication rates: a randomized potential study. Halo pin intracranial penetration and epidural abscess in a patient with a previous cranioplasty: case report and evaluation of the literature. Clinical, radiographic, and kinematic outcomes from an adjustable four-pad halo vest. Oropharyngeal morbidity following transoral approaches to the higher cervical spine. Odontoid upward migration in rheumatoid arthritis: an analysis of 45 sufferers with "cranial settling. Recurrent laryngeal nerve palsy after anterior cervical backbone surgery: the influence of endotracheal tube cuff deflation, reinflation, and strain adjustment. Intraoperative monitoring of the recurrent laryngeal nerve throughout revision thyroid surgery. The mechanism of recurrent laryngeal nerve damage throughout thyroid surgery-the utility of intraoperative neuromonitoring. Vertebral artery injury in cervical spine surgery: anatomical concerns, management, and preventive measures. Vertebral artery injury throughout cervical backbone surgical procedure: a survey of more than 5600 operations. Anatomical variations of the vertebral artery section within the lower cervical spine: analysis by three-dimensional computed tomography angiography. Upper airway obstruction by retropharyngeal hematoma after cervical backbone trauma: report of a case handled with percutaneous dilational tracheostomy. Anterior approaches to cervical spondylosis and ossification of the posterior longitudinal ligament: evaluate of operative method and evaluation of 65 multilevel circumferential procedures. Cervical spinal stenosis: outcome after anterior corpectomy, allograft reconstruction, and instrumentation. Central corpectomy for cervical spondylotic myelopathy: a consecutive series with long-term follow-up analysis. Subtotal corpectomy versus laminoplasty for multilevel cervical spondylotic myelopathy: a longterm follow-up research over 10 years. Surgery for ossification of the posterior longitudinal ligament of the cervical spine. Postoperative segmental C5 palsy after cervical laminoplasty might happen with out intraoperative nerve damage: a prospective study with transcranial electric motor-evoked potentials.
Buy pravachol 10 mg cheapThe differential analysis of optic disc edema cholesterol levels recommended generic 10 mg pravachol free shipping, or swelling, is extensive (Table 8-1). That time period should be reserved only for optic disc edema within the face of documented or strongly suspected raised intracranial strain. Note the pink neuroretinal rim, the central position of the central retinal artery and vein, and the branching sample of the retinal vasculature. This optic disc is at risk for the event of nonarteritic anterior ischemic optic neuropathy (see text). The normally transparent peripapillary nerve fiber layer gradually opacifies and obscures the retinal vessels. The optic disc could turn out to be hyperemic as small vessels are dilated, and characteristic splinter hemorrhages may appear at the disc margin in the nerve fiber layer. In addition, deeper hemorrhages might seem in the peripapillary retinal and subretinal layers. The swelling can also compromise venous outflow by enlarging the central veins at the disc, causing vascular tortuosity. Optic atrophy is the final frequent pathway of optic nerve illness that develops four to 6 weeks after vision loss. Virtually all optic nerve insults ultimately evolve to optic disc pallor or cupping, or both. The differential analysis of optic atrophy is broad and consists of all the problems that initially trigger disc edema and lots of entities that can result in axonal demise without first manifesting as disc swelling. The axons turn out to be myelinated after passing through openings in the sclera referred to as the lamina cribrosa. The retrobulbar optic nerve has three segments: intraorbital, intracanalicular within the optic canal, and intracranial simply anterior to the optic chiasm. The axons decussating within the chiasm are these from the nasal retina that serve the bitemporal visual fields. Posterior to the chiasm, all unilateral visible subject axons serve the contralateral hemifield. The retrochiasmal pathway consists of the optic tract, the lateral geniculate nuclei where the retinal ganglion cell axons synapse, the geniculocalcarine tracts in the temporal and parietal lobes, and the striate cortex within the occipital lobe. The the rest of this part will cowl pathologic examples of illness all through the afferent visual axis. The origin of a vision change might or may not be associated to the known neurosurgical pathology. For instance, in a affected person known to have an optic nerve sheath meningioma, unrelated retinal detachment could develop. A, Severe disc edema of the left optic disc from papilledema (raised intracranial pressure). Note the substantial blurring of the disc margins, nearly complete obscuration of the vasculature on the disc, peripapillary disc hemorrhages, and white gliosis and cotton-wool spots. Removal of the left cerebral hemisphere on this illustration permits visualization of the visible sensory system. Tear dysfunction is frequent in women older than forty years and could additionally be associated with collagen vascular illness, medicines, or systemic problems such as sarcoidosis. Cataract typically causes a gradual onset of blurred (rather than dim) vision or monocular diplopia with a standard or typically depressed visual subject without focal defects. Macular ailments trigger central imaginative and prescient loss or metamorphopsia (visual distortions). Age-related macular degeneration is a common cause of painless central vision loss in older sufferers; macular adjustments could be seen with the ophthalmoscope but are most unlikely to be seen without pharmacologic pupillary dilation. Central serous retinopathy causes central imaginative and prescient loss in younger sufferers from a fluid blister in the macula. Macular holes can lower visual acuity and trigger tiny central visible area defects. Cystoid macular edema can happen in association with diabetes, uveitis, and retinitis pigmentosa and cause central vision loss. Branch and central retinal artery occlusions cause acute, painless, monocular imaginative and prescient loss and focal visible area defects that can be just like these related to optic nerve problems. Papilledema Elevated intracranial stress from any cause can be transmitted to the optic nerve head and normally results in bilateral optic disc swelling, though typically asymmetrical and unilateral papilledema is possible. Although visible fields could show only enlargement of the physiologic blind spot from elevation of the peripapillary retina, the main visual concern with papilledema is the potential for peripheral imaginative and prescient loss, which may be asymptomatic and progress rapidly. Chronic papilledema could cause lack of the peripheral visual subject, with visible acuity affected solely very late in its course. Occlusion of the central retinal artery causes ischemia and opacification of the nerve fiber layer. This cream-colored edematous nerve fiber layer is most evident where the nerve fiber layer is thickest, in and around the macular space. Because of the anatomic peculiarities of the foveola, no axons can swell and thus obscure the traditional red colour of the uninvolved choroidal circulation, thereby giving rise to the classical cherry-red spot. A white, glistening cholesterol embolus is seen in a typical location, lodged at the bifurcation of a retinal arteriole. These flat crystalline emboli, not essentially occlusive, commonly accompany the sticky, lumen-filling, occlusive platelet-fibrin emboli originating from massive vessel atherosclerotic disease. The characteristic appearance of central retinal vein occlusion is hanging: flame-shaped hemorrhages (within the nerve fiber layer of the retina) are seen throughout the posterior pole along with engorged retinal veins and optic disc edema. Papilledema in a 19-year-old overweight lady with idiopathic intracranial hypertension. Brain magnetic resonance imaging was normal, and lumbar puncture showed a gap strain of 380 mm H2O. C and D, Visual fields demonstrate enlargement of the blind spots with further nasal and superior subject loss bilaterally. This graph demonstrates transient visual obscurations, which are transient episodes (lasting 1 to 5 seconds) of monocular or binocular visible blackout typically associated with postural modifications. Venous imaging with magnetic resonance or computed tomographic venogram is essential in these sufferers. Options embrace ventriculoperitoneal or lumboperitoneal shunting and optic nerve sheath fenestration. The vision loss with papilledema can be insidious and unappreciated by the patient, with extreme peripheral visual subject loss and poor outcomes, even within the presence of wonderful visible acuity. The elevated look of those discs with "buried" drusen could be confused with true optic disc edema. Depression of the retina simply temporal to the disc (nasal to the fovea) can cause "refractive" bilateral temporal visual subject defects that will simulate chiasmatic lesions. An infarct of the optic nerve head presumably occurs on account of occlusion of a quantity of of the posterior ciliary arteries that originate from the ophthalmic artery. The visible field defect tends to be everlasting, although minimal enchancment might happen over time. The prognosis for vision could be very poor on this situation, even with prompt correction of hypotension, hypovolemia, and hypoperfusion. Optic nerve sheath decompression, once considered a potential surgical therapy, was formally studied and shown to be ineffective, and presumably even harmful.
Order generic pravacholThus cholesterol test canada order 20mg pravachol visa, for n completely different states, each state is said to comprise log2 (n) bits of data. A bit is the knowledge essential to full a single binary operation, such as turning a change on or off. If one point of contact between two cells within the brain (a synapse) is taken into account a easy on-off device (switch), the human central nervous system might have as many as 1015 switches. This allows the brain to occupy at least (210)15 completely different states and thus maintain 1015 bits of data. Changes in information occur when the on-off switches are activated or deactivated in different combinations. The electrical membrane potential differences exist when ion concentrations vary throughout selectively permeable membranes. The selective permeabilities to the main extracellular and intracellular cations (sodium, potassium, calcium) decide the membrane potential distinction at a price that is sort of far faraway from the equilibrium potential of each of those ions, relying on the permeability of the membranes to every of the ions. Energy is needed to assist the ion transport that maintains these concentration gradients always, together with periods of rapidly altering practical activity. Neurons and different cells within the mind impose their metabolic needs on the mind by being topic to excitatory or inhibitory modifications in membrane permeability to sodium, potassium, chloride, and calcium ions. The increased exercise is required to keep the resting steadystate potential and ion gradients during and after dynamic changes within the potential. This implies that the actual initiation and regulation of impulse activity can take place with little or no change in the vitality turnover fee. The traditional "sodium concept" explains each the origin of the membrane potential and the graded or alternating depolarization of cells induced by the presence of sodium, calcium, potassium, and chloride equivalents as free ions within the intracellular and extracellular spaces, in addition to the action on, and the action of, particular ion channels in the plasma membranes throughout which the ions transfer. The conductances of sodium and potassium associated with the resting membrane potential and the increased conductances associated with excitation above a baseline or a resting or "default" common are matched by the active ion pumping that strives to preserve constant ion concentrations. A, Ordinates present oxygen (left) and glucose (right) metabolic charges for five distinct ranges of practical activity. B, Abscissa, practical stage on a scale from 0 to 4; ordinates, log2 scale of oxygen (left) and glucose (right) metabolic charges in models of �mol/g/min. In the steady state, a chloride flux matches the difference between the sodium and potassium fluxes and thus renders the total ion flux electroneutral. In steady-state conditions, the ion fluxes equal the diffusion charges in the opposite instructions. The resulting half-life of sodium in the cells is less than 1 minute under regular circumstances. The precise ion concentrations and the permeability of the membrane to the ions together determine the membrane potential distinction. Intuitively, it makes sense that the potassium ion, which has greater permeability in the membrane, has the major influence on the signal and magnitude of the membrane potential distinction. In the regular state, the obvious average potassium and sodium ion permeabilities, or the membrane permeability�surface space products, could be calculated from the potassium and sodium ion transport fluxes. The common ion concentrations vary amongst cells and tissue; typical values are listed in Table 49-1. Internal brain states regulate sensory perception, sensorimotor coordination, and learning, as reflected in several patterns of cortical synchrony. The concern hinges on the definitions of baseline and common functional exercise in relation to the totally different charges of metabolism in these states. Work by Shulman and colleagues implies that steady-state functional exercise is expounded to rates of release of the excitatory neurotransmitter glutamate and the linearly correlated charges of energy metabolism. These rates turn out to be about twice the rates associated with a very inactive however intact baseline state, which in flip are about twice the charges associated with the state of absent ion transport. To estimate chloride permeability, it was necessary to use a simplified type of the equation. By categorical increment is meant a change from one basic state of functional activity to the subsequent. The equation has an fascinating similarity to the formulation (see earlier) for a system that holds S bits of information. It in all probability reveals that distinct inner brain states dynamically regulate cortical membrane potential synchrony during habits and outline specific levels of cortical processing. In contrast, the nonfunctional baseline on this context is the state of absent useful activity. A rule of thumb derived from current experiments with dwelling intact mammalian brains estimates that solely about one fourth of the conventional vitality turnover maintains the minimal ion transport required within the absence of functional activity, as seen with isoelectricity on the electroencephalogram. It is in all probability going that maintenance of the membrane potential makes the main contribution to mind power use at the nonfunctional baseline (stage 1). The fraction of metabolism of isolated brain tissue associated with the transport of sodium and potassium is approximately half of the metabolism of the low functional state of isolated mind tissue. The state exists in conditions of severed cortical connections, coma, vegetative and minimally acutely aware states, or anesthesia. In these conditions, the metabolic price is close to 50% of the conventional resting awake or default average. Normal(Default)andPhysiologicallyElevated FunctionalStates(Stages3and4) the traditional or default metabolic stage refers to the awake and normally functioning mammalian brain. This stage has been studied extra comprehensively in awake humans than in other mammals. Stage three metabolism refers more accurately to the cerebral cortex of a resting awake human, whereas whole-brain values tend to symbolize a mixture of stage 2 and stage three metabolic states. The 10% nonoxidative metabolism of glucose leads to a rate of lactate production of about 5 to 7 �mol/hg per minute. However, with lactate manufacturing and uncoupling in mitochondria, the typical gain is lower than 30 mol per molecule of glucose. The finances additionally consists of processes similar to biosynthesis during useful activity in vivo and neurotransmitter vesicle formation, fusion, and release. According to the price range, 90% of the vitality turnover is devoted to "synaptic" exercise and hence maintenance of membrane potential associated with useful activity in the brain. Magnetic resonance spectroscopic measurements generally yield decrease values of lactate in vivo (0. Effect of photic stimulation on human visual cortex lactate and phosphates utilizing 1H and 31P magnetic resonance spectroscopy. Human brain oxygen consumption may increase to as much as 300 �mol/hg per minute beneath some physiologic circumstances, accompanied by increased glucose consumption to as much as 50 �mol/hg per minute. In the brains of very active rats, Silver and Erecinska found slight decreases in the extracellular glucose focus, as determined via a glucose-sensitive microelectrode placed in mind tissue. The lower affinities mean that the transporter turnover numbers are higher, which makes the approach to a model new steady state quicker, other factors being equal. For the same reason, export of pyruvate to the circulation is no more than 10% of that of lactate and thus could additionally be ignored within the larger perspective of brain energy metabolism. Thus, on average, the speed of pyruvate entry into mitochondria can rise fivefold as the protein approaches saturation. Such a profile favors cardio glycolysis, particularly the production of lactate within the presence of regular oxygen pressure.
References - Hernigou P, Pascale W, Pascale V, Homma Y, Poignard A. Does primary or secondary chondrocalcinosis influence long- term survivorship of unicompartmental arthroplasty? Clin Orthop Relat Res 2012; 470(7):1973-9.
- Scotti RJ, Garely AD, Greston WM, et al: Paravaginal repair of lateral vaginal wall defects by fixation to the ischial periosteum and obturator membrane, Am J Obstet Gynecol 179(6 Pt 1):1436n1445, 1998.
- Robertson CF, Rubinfeld AR, Bowes G. Deaths from asthma in Victoria: a 12-month survey. Med J Aust 1990; 152: 511-517.
- Elmqvist D, Lambert EH. Detailed analysis of neuromuscular transmission in a patient with the myasthenic syndrome sometimes associated with bronchogenic carcinoma. Mayo Clin Proc. 1968;43:689-713.
- Ellis SG FINESSE: Abciximab-only- and lytic/abciximabfacilitated PCI no better than primary PCI. theheartorg. 2007:http://www.theheart.org/article/809837.
- Bianco K, Small M, Julien S, et al. Second-trimester ductus venosus measurement and adverse perinatal outcome in fetuses with congenital heart disease. J Ultrasound Med. 2006; 25:979- 82; quiz 83.
- Dhir V, Itoi T, Fockens P, et al. Novel ex vivo model for hands-on teaching of and training in EUS-guided biliary drainage: creation of 'Mumbai EUS' stereolithography/3D printing bile duct prototype (with videos). Gastrointest Endosc. 2015;81:440-446.
|


