|
Molly A. Schnirring-Judge, DPM, FACFAS - Director of Podiatric Clerkship Program
- Department of Surgery
- St. Vincent Charity Hospital
- Cleveland, Ohio
Zyloprim dosages: 300 mg, 100 mg
Zyloprim packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

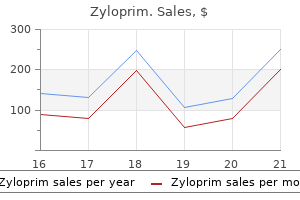
Purchase zyloprim from indiaWork Output of the Heart the stroke work output of the guts is the quantity of power that the guts converts to work during every heartbeat whereas pumping blood into the arteries treatment that works effective 100mg zyloprim. Minute work output is the total quantity of energy transformed to work in 1 minute; this is equal to the stroke work output times the guts rate per minute. Second, a minor proportion of the power is used to accelerate the blood to its velocity of ejection through the aortic and pulmonary valves, which is the kinetic vitality of blood flow part of the work output. Right ventricular exterior work output is normally about one sixth the work output of the left ventricle due to the sixfold difference in systolic pressures that the 2 ventricles pump. The further work output of each ventricle required to create kinetic power of blood move is proportional to the mass of blood ejected occasions the sq. of velocity of ejection. Ordinarily, the work output of the left ventricle required to create kinetic vitality of blood flow is simply about 1 p.c of the whole work output of the ventricle and due to this fact is ignored in the calculation of the total stroke work output. In certain irregular conditions, nevertheless, similar to aortic stenosis, in which blood flows with great velocity through the stenosed valve, greater than 50 percent of the total work output could additionally be required to create kinetic power of blood move. Also shown by the redlinesisthe"volume-pressurediagram,"demonstratingchanges in intraventricular volume and stress in the course of the regular cardiac cycle. The most essential parts of the diagram are the 2 curves labeled "diastolic strain" and "systolic stress. The diastolic strain curve is set by filling the center with progressively larger volumes of blood and then measuring the diastolic pressure immediately before ventricular contraction occurs, which is the enddiastolic stress of the ventricle. The systolic pressure curve is decided by recording the systolic pressure achieved throughout ventricular contraction at every quantity of filling. Therefore, up to this quantity, blood can circulate easily into the ventricle from the atrium. Above one hundred fifty milliliters, the ventricular diastolic stress increases rapidly, partly due to fibrous tissue within the heart that may stretch no extra and partly as a result of the pericardium that surrounds the heart turns into filled practically to its restrict. During ventricular contraction, the systolic strain will increase even at low ventricular volumes and reaches a most at a ventricular volume of 150 to one hundred seventy milliliters. For the normal proper ventricle, the utmost systolic strain is between 60 and 80 mm Hg. Phase I in the volume-pressure diagram begins at a ventricular volume of about 50 milliliters and a diastolic pressure of two to three mm Hg. The amount of blood that remains in the ventricle after the previous heartbeat, 50 milliliters, is called the endsystolic quantity. As venous blood flows into the ventricle from the left atrium, the ventricular volume usually will increase to about a hundred and twenty milliliters, known as the enddiastolic quantity, an increase of 70 milliliters. During ejection, the systolic pressure rises even greater due to nonetheless extra contraction of the ventricle. At the same time, the quantity of the ventricle decreases as a result of the aortic valve has now opened and blood flows out of the ventricle into the aorta. Thus, the ventricle returns to its starting point, with about 50 milliliters of blood left in the ventricle and at an atrial strain of 2 to three mm Hg. In experimental studies of cardiac contraction, this diagram is used for calculating cardiac work output. When the center pumps massive portions of blood, the area of the work diagram becomes a lot larger. That is, it extends far to the right because the ventricle fills with more blood throughout diastole, it rises a lot larger as a end result of the ventricle contracts with higher strain, and it normally extends farther to the left as a outcome of the ventricle contracts to a smaller volume-especially if the ventricle is stimulated to increased activity by the sympathetic nervous system. In assessing the For cardiac contraction, the preload is normally considered to be the end-diastolic strain when the ventricle has turn into crammed. The afterload of the ventricle is the strain in the aorta main from the ventricle. Chemical Energy Required for Cardiac Contraction: Oxygen Utilization by the Heart Heart muscle, like skeletal muscle, makes use of chemical power to provide the work of contraction. Approximately 70 to 90 p.c of this vitality is generally derived from oxidative metabolism of fatty acids, with about 10 to 30 percent coming from other vitamins, especially lactate and glucose. Therefore, the rate of oxygen consumption by the guts is a superb measure of the chemical energy liberated whereas the heart performs its work. The different chemical reactions that liberate this energy are discussed in Chapters 68 and sixty nine. The potential power represents further work that might be completed by contraction of the ventricle if the ventricle should completely empty all of the blood in its chamber with each contraction. Oxygen consumption has also been shown to be nearly proportional to the tension that happens in the coronary heart muscle throughout contraction multiplied by the duration of time that the contraction persists, referred to as the tensiontime index. Because tension is high when systolic pressure is high, correspondingly more oxygen is used. Also, much more chemical power is expended even at regular systolic pressures when the ventricle is abnormally dilated as a result of the center muscle pressure throughout contraction is proportional to pressure times the diameter of the ventricle. This turns into particularly important in heart failure when the guts ventricle is dilated and, paradoxically, the quantity of chemical vitality required for a given quantity of work output is greater than normal even though the center is already failing. During heart muscle contraction, a lot of the expended chemical vitality is converted into heat, and a much smaller portion is transformed into work output. The ratio of labor output to total chemical vitality expenditure known as the effectivity of cardiac con traction, or simply effectivity of the heart. In individuals with heart failure, this efficiency can decrease to as low as 5 to 10 percent. Basically, the Frank-Starling mechanism means that the larger the center muscle is stretched throughout filling, the greater is the drive of contraction and the larger the amount of blood pumped into the aorta. Or, stated one other method: Within physiological limits, the guts pumps all of the blood that returns to it by way of the veins. This stretching in turn causes the muscle to contract with increased drive as a outcome of the actin and myosin filaments are delivered to a more practically optimal diploma of overlap for pressure technology. Therefore, the ventricle, due to its increased pumping, automatically pumps the extra blood into the arteries. In addition to the important effect of lengthening the guts muscle, nonetheless another factor will increase heart pumping when its volume is increased. Stretch of the proper atrial wall immediately increases the guts rate by 10 to 20 %, which also helps enhance the quantity of blood pumped each minute, although its contribution is way less than that of the Frank-Starling mechanism. During strenuous exercise, the guts could additionally be required to pump 4 to seven occasions this amount. The fundamental means by which the volume pumped by the guts is regulated are (1) intrinsic cardiac regulation of pumping in response to modifications in volume of blood flowing into the guts and (2) management of heart rate and energy of coronary heart pumping by the autonomic nervous system. Ventricular Function Curves One of the most effective ways to express the functional capability of the ventricles to pump blood is by ventricular function curves. That is, every peripheral tissue of the physique controls its personal local blood flow, and all of the native tissue flows mix and return by means of the veins to the best atrium.
Buy zyloprim 100 mg lowest priceMany of them have a adverse electrical cost shakira medicine discount zyloprim 300mg without a prescription, which gives most cells an overall unfavorable surface charge that repels other negatively charged objects. The glycocalyx of some cells attaches to the glycocalyx of other cells, thus attaching cells to one another. Many of the carbohydrates act as receptor sub stances for binding hormones, corresponding to insulin; when 14 sure, this mix activates attached inner proteins that, in turn, activate a cascade of intracellular enzymes. Some carbohydrate moieties enter into immune reactions, as discussed in Chapter 35. The jelly-like fluid portion of the cytoplasm during which the particles are dispersed is recognized as cytosol and incorporates mainly dissolved proteins, electrolytes, and glucose. Dispersed in the cytoplasm are neutral fats globules, glycogen granules, ribosomes, secretory vesicles, and five especially essential organelles: the endoplasmic reticu lum, the Golgi equipment, mitochondria, lysosomes, and peroxisomes. Also, their partitions are constructed of lipid bilayer membranes that include massive quantities of proteins, just like the cell membrane. The complete surface area of this structure in some cells-the liver cells, for instance-can be as a lot as 30 to 40 times the cell membrane area. Electron micrographs present that the house contained in the endoplasmic reticulum is linked with the house between the two membrane surfaces of the nuclear membrane. Substances formed in some elements of the cell enter the space of the endoplasmic reticulum and are then directed to different parts of the cell. Also, the huge floor space of this reticulum and the a quantity of enzyme methods attached to its membranes provide equipment for a serious share of the metabolic capabilities of the cell. The agranular reticulum functions for the synthesis of lipid substances and for other processes of the cells promoted by intrareticular enzymes. The Golgi equipment is often composed of four or extra stacked layers of skinny, flat, enclosed vesicles lying close to one side of the nucleus. The transported substances are then processed within the Golgi apparatus to type lysosomes, secretory vesicles, and other cytoplasmic components which would possibly be mentioned later in this chapter. Attached to the outer surfaces of many components of the endoplasmic reticulum are large numbers of minute granular particles called ribosomes. Where these particles are present, the reticulum is known as the granular endoplasmic reticulum. The lysosomes provide an intracellular digestive system that allows the cell to digest (1) broken cellular buildings, (2) meals particles that have been ingested by the cell, and (3) unwanted matter corresponding to micro organism. It is surrounded by a typical lipid 15 plasmic reticulum has no connected ribosomes. This half Unit I Introduction to Physiology: the Cell and General Physiology bilayer membrane and is crammed with massive numbers of small granules 5 to eight nanometers in diameter, that are protein aggregates of as many as 40 completely different hydrolase (digestive) enzymes. A hydrolytic enzyme is capable of splitting an organic compound into two or extra components by combining hydrogen from a water molecule with one part of the compound and mixing the hydroxyl portion of the water molecule with the other part of the compound. For instance, protein is hydrolyzed to kind amino acids, glycogen is hydrolyzed to kind glucose, and lipids are hydrolyzed to type fatty acids and glycerol. Ordinarily, the membrane surrounding the lysosome prevents the enclosed hydrolytic enzymes from coming in contact with other substances in the cell and therefore prevents their digestive actions. However, some circumstances of the cell break the membranes of some of the lysosomes, allowing release of the digestive enzymes. These enzymes then break up the natural substances with which they arrive in contact into small, extremely diffusible substances corresponding to amino acids and glucose. Several of the oxidases are able to combining oxygen with hydrogen ions derived from completely different intracellular chemicals to type hydrogen peroxide (H2O2). Hydrogen peroxide is a highly oxidizing substance and is utilized in association with catalase, one other oxidase enzyme current in massive portions in peroxisomes, to oxidize many substances that may otherwise be poisonous to the cell. For instance, about half the alcohol an individual drinks is detoxified into acetaldehyde by the peroxisomes of the liver cells in this method. Without them, cells could be unable to extract sufficient energy from the nutrients, and basically all mobile functions would stop. The cardiac muscle cells (cardiomyocytes), for example, use giant quantities of energy and have way more mitochondria than do fat cells (adipocytes), which are a lot much less active and use much less power. Further, the mitochondria are concentrated in these portions of the cell which are liable for the major share of its energy metabolism. Some mitochondria are only a few hundred nanometers in diameter and are globular in form, whereas others are elongated and are as large as 1 micrometer in diameter and 7 micrometers long; nonetheless others are branching and filamentous. Many infoldings of the inside membrane form Secretory Vesicles One of the necessary features of many cells is secretion of particular chemical substances. Almost all such secretory substances are fashioned by the endoplasmic reticulum� Golgi equipment system and are then released from the Golgi apparatus into the cytoplasm within the type of storage vesicles called secretory vesicles or secretory granules. The proenzymes are secreted later by way of the outer cell membrane into the pancreatic duct and thence into the duodenum, the place they become activated and carry out digestive features on the meals within the intestinal tract. In addition, the inside cavity of the mitochondrion is filled with a matrix that accommodates massive portions of dissolved enzymes that are essential for extracting power from vitamins. These enzymes operate in affiliation with the oxidative enzymes on the cristae to trigger oxidation of the vitamins, thereby forming carbon dioxide and water and on the same time releasing vitality. Cells which are confronted with increased energy demands-which occurs, for instance, in skeletal muscular tissues subjected to continual exercise training-may improve the density of mitochondria to supply the additional vitality required. The cytoskeleton of the cell not only determines cell shape but additionally participates in cell division, allows cells to move, and supplies a track-like system that directs the movement of organelles throughout the cells. Nucleus the nucleus, which is the management center of the cell, sends messages to the cell to develop and mature, to replicate, or to die. During mitosis, the chromatin material organizes in the type of highly structured chromosomes, which may then be simply recognized using the light microscope, as illustrated in Chapter three. The nuclear membrane, also referred to as the nuclear envelope, is actually two separate bilayer membranes, one inside the opposite. The outer membrane is Cell Cytoskeleton-Filament and Tubular Structures the cell cytoskeleton is a network of fibrillar proteins organized into filaments or tubules. These originate as precursor protein molecules synthesized by ribosomes in the cytoplasm. As an instance, giant numbers of actin filaments incessantly occur within the outer zone of the cytoplasm, known as the ectoplasm, to form an elastic assist for the cell membrane. A special sort of stiff filament composed of polymerized tubulin molecules is used in all cells to construct robust tubular buildings, the microtubules. Another example of microtubules is the tubular skeletal construction within the heart of each cilium that radiates upward from the cell cytoplasm to the tip of the cilium. Also, both the centrioles and the mitotic spindle of the mitosing cell are composed of stiff microtubules. Large complexes of protein molecules are hooked up on the edges of the pores so that the central area of each pore is just about 9 nanometers in diameter.
Cheap 100mg zyloprim mastercardThe axis of the uterus is often dextrorotated by the presence of the sigmoid colon; this rotation have to be thought-about when performing a hysterotomy on the time of caesarean part to avoid injuring the big uterine vessels located bilaterally symptoms bladder cancer buy generic zyloprim 100mg on line. In order to compensate for this, the mom tends to straighten her cervical and thoracic backbone, and throw her shoulders again, leading to a compensatory lumbar lordosis. There can be a softening of the pubic symphysis and sacroiliac joints, attributable to manufacturing of relaxin and other pregnancy hormones, leading to mild pelvic instability that may result in a waddling gait. Softening also produces an increase in pelvic diameter, which is of profit in the course of the time of labour. Significant joint relaxation may lead to pubic symphysis diastasis, which, in extreme instances, could produce debilitating pain throughout strolling. Advances in three-dimensional ultrasound imaging allow the realtime visualization of the anatomical relationships and adaptations of the pelvic floor in being pregnant. They also allow detection of pelvic ground harm that might lead to symptomatic postpartum pelvic flooring prolapse (Dietz and Lanzarone 2005, Shek et al 2012). In early pregnancy, the placental disc occupies a large proportion of the uterine cavity and can typically appear to be situated close to the inner os. In nearly all of instances, growth and stretching of the uterus will normally draw the placenta upwards, away from the cervix, by the top of being pregnant. This situation known as placenta praevia and could be related to vaginal bleeding during pregnancy and labour. If the placenta covers the interior os, or the decrease edge is lower than 1�2 cm from the inner os, delivery by caesarean section is generally indicated. Normal trophoblastic growth includes the remodelling of maternal spiral arterioles to permit for low-resistance move into the intervillous space. Thus, the uteroplacental vasculature is a low-resistance, high-capacitance system. Abnormally invasive placentation can happen when trophoblastic tissue invades via the decidua basalis and reaches the myometrium; this can lead to a morbidly adherent placenta and significant maternal morbidity. In excessive cases, a placenta percreta can also invade into the maternal bladder mucosa. Note the hypervascularity attributable to the placental tissue invading into, and nearly through, the myometrial layer of the decrease uterine section, which is still covered with its serosal layer. The spiral umbilical vessels in the umbilical wire and their radiating branches are seen via the transparent amnion. Note the fringes of amnion and chorion, the majority of which have been cut away close to the placental margin. Progress is decided by the equilibrium between forces generated by myometrial contractions, particularly from the fundus, and the resistance of the cervix. Cervical resistance is misplaced and myometrial exercise results in isometric contractions that help descent of the fetus within the birth canal. The head of the fetus often enters the pelvis with the occiput facing laterally. As the top descends additional, the occiput contacts the gutter-shaped pelvic flooring shaped by levator ani and this promotes flexion and rotation of the occiput to the anterior place. With further descent, the occiput escapes beneath the pubic symphysis and the pinnacle is born by extension. At this point, the pinnacle of the fetus regains its normal relationship with its shoulders, and slight rotation (or restitution) of the pinnacle is seen. Further exterior rotation occurs as the main shoulder is directed medially by the maternal pelvic ground. The physique of the fetus is now born by lateral flexion as one shoulder slips beneath the symphysis and the posterior shoulder is drawn over the frenulum. Third stage Placenta after supply Separation of the placenta from the uterine wall takes place alongside the aircraft of the stratum spongiosum and extends past the placental area, detaching the villous placenta, with associated fibrinoid matrix and small amounts of decidua basalis; the chorio-amnion, together with a superficial layer of the fused decidua capsularis; and the decidua parietalis. When the placenta and membranes have been expelled, a thin layer of stratum spongiosum is left lining the uterus; it soon degenerates and is solid off in the early a part of the puerperium. Occasionally, the twine fails to reach the placenta itself and ends in the membranes as a velamentous insertion. After separation within the third stage of labour, maternal exsanguination is simply prevented by marked uterine contraction; the crisscrossing myometrial fibres act as a tourniquet, limiting blood flow to the realm that was the placental web site. This process is often expedited clinically by the administration of oxytocic medicine in an attempt to restrict maternal blood loss. Any situation that predisposes to poor uterine contraction, corresponding to retained placental tissue, will enhance the probability of postpartum haemorrhage. It is thickest at its centre (the original embryonic pole), and rapidly thins towards its periphery, where it continues as the chorion laeve. The umbilical cord is usually connected close to the centre of the fetal floor, and branches of the umbilical vessels radiate out underneath the amnion from this point; the veins are deeper and larger than the arteries. The maternal surface of the placenta is finely granular and mapped into some 15�30 lobes by a sequence of fissures or grooves. The placental lobes, which are often considerably loosely termed cotyledons, correspond, in large measure, to the main branches of the umbilical vessels. The grooves correspond to the bases of incomplete placental septa, which become more and more outstanding from the third month onwards. The septa are advanced constructions composed of components of the cytotrophoblastic shell and residual syncytium, together with maternally derived materials, including decidual cells, occasional blood vessels and gland remnants, collagenous and fibrinoid extracellular matrix, and, in the later months of pregnancy, foci of degeneration. In multiple pregnancies, the variety of placentas is decided by the zygosity; for example, in twin gestations, dizygotic pregnancies will at all times have two placentas (dichorionic). Monozygotic pregnancies often have a single placenta (monochorionic), but about one-third may have two placentas; the number is decided by the timing of splitting of the embryonic mass (see Ch. They travel unprotected via the membranes to the placenta, and this puts the fetus in danger as a end result of compression or tearing of the vessels can disrupt blood circulate to and from the fetus. This can be significantly problematic when the vessels present themselves throughout the cervical os, a condition known as vaso praevia. An accessory (succenturiate) placental lobe is often current, linked to the primary organ by membranes and blood vessels. A, the fetal floor and a thick ring of membranes on the fetal floor of the placenta. B, A part by way of the placenta, displaying that the membranes insert central to the edge of the placental disc. A chapter that provides a detailed evaluation of the supports of the vagina and the pelvic organs. A landmark study that prospectively identified levator trauma after vaginal delivery utilizing non-invasive three-dimensional ultrasound. An account that critiques the morphological and useful elements of the ovarian follicle, corpus luteum and germ cells using light microscopy, electron microscopy and quite a few drawings. A study that demonstrates the anatomical modifications that happen within the pelvic ground on the urethral hiatus throughout pregnancy. Badouraki M, Christoforidis A, Economou I et al 2008 Sonographic evaluation of uterine and ovarian improvement in normal ladies aged 1 to 12 years. Chen C, Huang L, Liu P et al 2014 Neurovascular quantitative examine of the uterosacral ligament related to nerve-sparing radical hysterectomy.
Discount zyloprim american expressIn the absence of the menisci treatment atrial fibrillation purchase 100mg zyloprim fast delivery, the load is carried by a a lot smaller area of cartilage, leading to greater contact stresses on the articular cartilage. The anterior�posterior movement of the menisci is approximately half the magnitude of the anterior�posterior motion of the femur, suggesting that the conformity of the joint adjustments during flexion of the knee joint. The distal side of the femur, resting on the menisci in the prolonged knee, has a large radius of curvature and thus suits in opposition to the entire area of the menisci. However, because the knee flexes, the smaller radii of the posterior parts of the femoral condyles trigger the femur to carry off the Medial compartment Lateral compartment Medial pivot in concave tibial plateau the knee acts as a bearing that transmits forces and actions between the limb segments. Load-bearing synovial joints transfer with remarkably little friction and their surfaces should withstand many tens of millions of impact hundreds, which are inclined to cause fatigue failure and breakdown of the surfaces. During walking, each step includes phases of action that change the loading and velocity circumstances on the knee joint. At the time of heel strike, a large influence load acts to compress the surfaces collectively. In the mid-stance part, the flexion�extension movement again entrains the synovial fluid in between the joint surfaces, producing what is known as a hydrodynamic effect: the fluid is trapped between the surfaces by the motion and subsequently it acts to separate them. If the squeeze-film effect were inadequate, then the joint surfaces would come into direct contact were it not for the fact that the synovial fluid incorporates massive protein molecules that are trapped on the cartilage surfaces when the fluid is expelled. This molecular layer acts as a boundary lubricant, protecting the cartilage in the same means that grease protects a synthetic bearing. Many aspects of the arthritic breakdown of the cartilage can be explained on the idea of lubrication biomechanics. Thus, in joints affected by osteoarthrosis, synovial fluid is thought to have a lower viscosity than that in regular joints. The viscosity is lower still in joints afflicted with rheumatoid arthritis and is unable to forestall attritional damage to the cartilage surfaces. Disruption of any of these passive restraints may cause a mechanical instability, which is an abnormally elevated displacement because of an applied drive (in biomechanical phrases this is called excess laxity). The muscles provide the loading to move the joint: quadriceps femoris, hamstrings and gastrocnemius control each flexion/extension and medial�lateral rotation. However, additionally they cause anterior�posterior shear forces which would possibly be resisted primarily by the cruciate ligaments. This tethering effect is critical in permitting the joint to transfer physiologically, sustaining congruency and stability. The passive stabilizers of the joint act by resisting unwanted displacements between the bones. When the muscular tissues or another exterior force (due to physique weight or impact) cause the bones to displace, the ligaments are stretched, and so develop tensile forces that resist the 1396 On testing the laxity in any of the degrees of freedom of the joint. These are termed primary restraints, and are exemplified by the cruciate ligaments and the tibial and fibular collateral ligaments. Secondary restraints are less properly aligned but still have a big restraining impact. With an absent anterior cruciate ligament, the tibial collateral ligament can resist the applied drive; nevertheless, it does so by being loaded to a much larger stage than the original loading on the anterior cruciate ligament. The dimension of the lines within the vector diagram demonstrate this precept: though joint laxity might stay regular initially following rupture of a main restraint, it might subsequently outcome in the overload of a secondary restraint and, in the end, in additional gentle tissue failure. The patellofemoral joint is most heavily loaded during weightbearing actions when the knee is flexed. Analyses of rising from a chair have predicted that the patellar ligament tension at 90� of knee flexion could also be larger than the tibiofemoral joint, which is loaded on the identical time (Amis and Farahmand 1996). In the frontal airplane, quadriceps femoris and the patellar ligament tensions mix to trigger a lateralizing pressure vector termed the Q-angle impact. Clinically, the Q angle is modified by the place of hip rotation, tibial rotation and quadriceps femoris rigidity. Contraction of quadriceps femoris, subsequently, tends to displace the patella laterally, which is resisted by the geometry of the joint and by the ligaments. Vastus medialis obliquus acts medially and posteriorly as much as it acts proximally, and so its pressure helps to resist the Q-angle impact. This ligament is the one most necessary stabilizer of the posterolateral region of the knee and resists lateral rotation of the tibia on the femur. Failure to acknowledge and reconstruct damage to this ligament and to the related ligamentous constructions is the most typical purpose for a poor result from an otherwise well-performed operation for repair of ruptured cruciate ligaments. Fleshy fibres broaden from the inferior restrict of the tendon to type a considerably triangular muscle that descends medially to be inserted into the medial two-thirds of the triangular space above the soleal line on the posterior surface of the tibia, and into the tendinous expansion that covers its surface. An further head might come up from the sesamoid bone in the lateral head of gastrocnemius. Popliteus minor runs from the posterior floor of the lateral tibial condyle, medial to plantaris, to the indirect popliteal ligament. Peroneotibialis runs deep to popliteus from the medial side of the fibular head to the upper finish of the soleal line. Gastrocnemius, plantaris, the popliteal vessels and the tibial nerve all lie posterior to the enlargement. The popliteal tendon is intracapsular and is deep to the fibular collateral ligament and the tendon of biceps femoris. It is invested on its deep surface by synovial membrane, and grooves the posterior border of the lateral meniscus and the adjoining part of the tibia before it emerges inferior to the posterior band of the arcuate ligament. There are additional contributions from the nutrient artery of the tibia (from the posterior tibial artery), the proximal part of the posterior tibial artery, and the posterior tibial recurrent artery. Actions Popliteus rotates the tibia medially on the femur or, when the tibia is mounted, rotates the femur laterally on the tibia. Its connection with the arcuate popliteal ligament, fibrous capsule and lateral meniscus has led to the suggestion that popliteus may retract the posterior horn of the lateral meniscus throughout lateral rotation of the femur and flexion of the knee joint, thus defending the meniscus from being crushed between the femur and the tibia during these actions. The muscle is markedly active in crouching, perhaps to present stability as the tibia rotates medially throughout flexion of the knee. However, the primary operate is more probably to be provision of dynamic stability to the posterolateral a half of the knee by preventing excessive lateral rotation of the tibia, partly by its direct action, but more significantly by tensing the popliteofibular ligament. A superficial arterial network spreads between the fascia and skin across the patella and within the fat deep to the patellar ligament. The vessels involved are the superior, middle and inferior genicular branches of the popliteal artery; descending genicular branches of the femoral artery and descending branch of the lateral circumflex femoral artery; circumflex fibular artery; and anterior and posterior tibial recurrent arteries. Medially, this tendon is joined by collagenous fibres arising from the arcuate popliteal ligament; the fibrous capsule adjacent to the lateral meniscus; and the outer margin of the meniscus. They are normally incidental findings in the dissection room, or might come to light in the midst of angiographic examination. Some variations in vascular anatomy could additionally be symptomatic and will necessitate surgical correction; other variations, while asymptomatic, may affect technical issues throughout vascular surgical procedures. Anatomical variations of the femoral, profunda femoris, anterior and posterior tibial and fibular arteries have been described elsewhere in this Section. It descends laterally from the opening in adductor magnus to the femoral intercondylar fossa, inclining obliquely to the distal border of popliteus, the place it divides into the anterior and posterior tibial arteries.
Buy cheap zyloprim 100 mg lineIt crosses the tendon of flexor digitorum longus from lateral to medial medicine to stop runny nose cheap zyloprim 300 mg, curving obliquely superior to it. At the crossing point (knot of Henry), it gives off two sturdy slips to the medial two divisions of the tendons of flexor digitorum longus after which crosses the lateral part of flexor hallucis brevis to reach the interval between the sesamoid bones underneath the top of the first metatarsal. The tendon is retained in position over the lateral part of flexor hallucis brevis by the diverging stems of the distal band of the medial intermuscular septum. The distal extent of the muscle stomach is a particular characteristic; in the posteromedial surgical approach to the ankle, flexor hallucis longus is instantly identifiable by the reality that muscle fibres are evident virtually to calcaneal level. In athletes, the muscle fibres may be current up to now inferiorly into the tendon as to be vulnerable to impingement when pulled into the tunnel at the talus. The connecting slip to flexor digitorum longus varies in dimension; it normally continues into the tendons for the second and third toes however is typically restricted to the second toe and occasionally extends to the fourth toe. The medial process arises from the posterior floor of the interosseous membrane, besides at its most distal half, and from a lateral space on the posterior surface of the tibia between the soleal line above and the junction of the middle and lower thirds of the shaft below. The lateral half arises from a medial strip of the pos terior fibular floor in its higher twothirds. The muscle additionally arises from the transverse intermuscular septum, and from the intermuscular septa that separate it from adjoining muscle tissue. It then passes deep to the flexor retinaculum and superficial to the deltoid ligament to enter the foot. The extra superficial and larger division, which is a direct continuation of the tendon, is connected to the tuberosity of the navicular, from which fibres continue to the inferior floor of the medial cuneiform. A tendinous band also passes laterally and slightly proximally to the tip and distal margin of the sustentaculum tali. The deeper lateral division gives rise to the tendon of origin of the medial limb of flexor hallucis brevis, and then continues between this muscle and the navicular and medial cuneiform to end on the intermediate cuneiform and the bases of the second, third and fourth metatarsals; the slip to the fourth metatarsal is the strongest. An extra muscle, the tibialis secundus, has been described working from the again of the tibia to the capsule of the ankle joint. Relations the superficial floor of tibialis posterior is separated from soleus by the transverse intermuscular septum, and is said to flexor digitorum longus, flexor hallucis longus, the posterior tibial vessels, the tibial nerve and the fibular vessels. The deep surface is in touch with the interosseous membrane, tibia, fibula and ankle joint. Vascular provide Tibialis posterior is equipped by quite a few branches of small calibre arising from the posterior tibial and fibular arteries. The tendon is equipped by arteries of the medial malleolar network and by the medial plantar artery. Deeply situated are the fibula, tibialis posterior, fibular vessels, distal a half of the interosseous membrane and the talocrural joint. Lat erally lie fibularis longus and fibularis brevis; medially are tibialis pos terior, posterior tibial vessels and the tibial nerve. Flexor hallucis longus is a vital surgical landmark on the ankle; staying lateral to it prevents damage to the neurovascular bundle. Actions Tibialis posterior is a strong muscle that, on contraction, has an excursion of solely 1�2 cm. It is phasically active in strolling, throughout which it in all probability acts with the intrinsic foot musculature and the lateral leg muscular tissues to management the degree of pronation of the foot and the distribution of weight by way of the metatarsal heads. It is alleged that when the physique is supported on one leg, the invertor action of tibialis posterior, exerted from beneath, helps to keep steadiness by resisting any tendency to sway laterally. Tibialis posterior is also essential in the maintenance of the medial part of the longitudinal arch of the foot. In chubby individuals with pes planus (flat foot deformity), unaccustomed exercise may find yourself in irritation and degeneration of the terminal portion of the tendon, which leads to elongation of the tendon, attenuation of the spring liga ment and progressive collapse of the medial longitudinal arch. Vascular provide Flexor hallucis longus is provided by quite a few branches of the fibular artery. Innervation Flexor hallucis longus is innervated by branches of the tibial nerve, L5, S1 and S2 (mainly S1). Testing Flexor hallucis longus is tested by flexion of the hallux against resistance. When the foot is off the ground, each muscle tissue flex the phalanges, performing totally on the distal phalanges. When the foot is on the ground and underneath load, they act synergistically with the small muscular tissues of the foot and, particularly in the case of flexor digitorum longus, with the lumbricals and interossei to preserve the pads of the toes in firm contact with the bottom, enlarging the weightbearing space and helping to stabilize the heads of the metatarsals, which type the fulcrum on which the physique is propelled forwards. Activity within the lengthy digital flexors is minimal throughout quiet standing, so they apparently contribute little to the static maintenance of the longitudinal arch, however they turn into very lively during toeoff and tiptoe actions. Testing tibialis posterior operate is essential in establishing a analysis of a standard fibular nerve neuropathy and differentiating it from an L5 radiculopathy, that are two common clinical situations. In a standard fibular nerve neur opathy, tibialis posterior has regular operate, whereas in an L5 radicul opathy, tibialis posterior is weak. Descending on the anterior aspect of the membrane, it approaches the tibia and, distally, lies anterior to it. At the ankle, the anterior tibial artery is positioned approximately midway between the malleoli, and it continues on the dorsum of the foot, lateral to extensor hallucis longus, as the dorsalis pedis artery. Its operate could additionally be replaced by perforating branches from the posterior tibial artery or by the perforating department of the fibular artery. It can also be larger than regular, during which case its territory of supply within the foot may be elevated to embody the plantar floor. Proximally, it lies between tibialis anterior and extensor digitorum longus, then between tibialis anterior and extensor hallucis longus. Its proximal twothirds are coated by adjoining muscle tissue and deep fascia, its distal third by the pores and skin, fasciae and extensor retinacula. The deep fibular nerve, curling laterally round the fibular neck, reaches the lateral side of the artery where it enters the extensor area, is then anterior to the artery in the middle third of the leg, and becomes lateral once more distally. Branches the named branches of the anterior tibial artery are the posterior and anterior tibial recurrent, muscular, perforating, and anterior medial and lateral malleolar arteries. Posterior tibial recurrent artery the posterior tibial recurrent artery is an inconstant department that arises earlier than the anterior tibial artery reaches the extensor compartment of the leg. It ascends anterior to popliteus, anastomosing with the inferior genicular branches of the popliteal artery. Anterior tibial recurrent artery the anterior tibial recurrent artery arises near the posterior tibial recurrent artery. It ascends in tibialis anterior, ramifies on the front and sides of the knee joint, and joins the patellar anastomosis, which interconnects with the genicular branches of the popliteal and circumflex fibular arteries. Some then pierce the deep fascia to supply the pores and skin, while others traverse the interosseous membrane to anastomose with branches of the posterior tibial and fibular arteries. Perforating branches Most of the fasciocutaneous perforators move along the anterior fibular fascial septum behind extensor digitorum longus earlier than penetrating the deep fascia to supply the skin. Anterior medial malleolar artery the anterior medial malleolar Profunda femoris artery artery arises approximately 5 cm proximal to the ankle. It passes pos terior to the tendons of extensor hallucis longus and tibialis anterior medial to the joint, the place it joins branches of the posterior tibial and medial plantar arteries. Anterior lateral malleolar artery the anterior lateral malleolar Femoral artery artery runs posterior to the tendons of extensor digitorum longus and fibularis tertius to the lateral facet of the ankle and anastomoses with the perforating department of the fibular artery and ascending branches of the lateral tarsal artery. It descends medially in the flexor compartment and divides underneath abductor hal lucis, midway between the medial malleolus and the calcaneal tubercle, into the medial and lateral plantar arteries.
Buy genuine zyloprim onlineThe increase in blood volume tends to enhance venous return to the guts treatment quotes and sayings buy cheap zyloprim 300mg line, which, in turn, causes the left ventricle to pump with the extra energy required to overcome the irregular pumping dynamics. For this purpose, even in individuals with extreme mitral stenosis, no murmur may be heard through the first third of diastole. Then, after partial filling, the ventricle has stretched enough for blood to reverberate and a low rumbling murmur begins. It is clear from these phonocardiograms that the aortic stenotic lesion causes the loudest murmur, and the mitral stenotic lesion causes the weakest murmur. The phonocardiograms present how the intensity of the murmurs varies throughout different portions of systole and diastole, and the relative timing of every murmur can additionally be evident. This action will increase work load and oxygen consumption of the ventricle, necessitating increased coronary blood flow to ship this oxygen. The excessive wall rigidity of the ventricle, nonetheless, causes marked decreases in coronary move during systole, significantly in the subendocardial vessels. With aortic regurgitation the intraventricular diastolic stress also will increase, compressing the inside layer of the guts muscle and lowering coronary blood move. Aortic diastolic stress decreases throughout aortic regurgitation, which may also lower coronary blood flow and cause ischemia of the heart muscle. In the early phases of aortic Aortic Valvular Lesions May be Associated with Inadequate Coronary Blood Flow. The buildup of blood in the left atrium causes progressive enhance in left atrial stress, ultimately ensuing in the growth of great pulmonary edema. This pathway could eventually turn into so long that it predisposes to the development of excitatory signal circus movements, as discussed in Chapter 13. Therefore, in late phases of mitral valvular disease, particularly in mitral stenosis, atrial fibrillation often occurs. This growth further reduces the pumping effectiveness of the heart and causes additional cardiac debility. As stenosis or aortic regurgitation, the intrinsic ability of the left ventricle to adapt to increasing masses prevents significant abnormalities in circulatory operate in the particular person throughout rest, aside from increased work output required of the left ventricle. Therefore, appreciable levels of aortic stenosis or aortic regurgitation usually occur earlier than the particular person knows that he or she has serious heart disease (such as a resting left ventricular systolic strain as excessive as 200 mm Hg in persons with aortic stenosis or a left ventricular stroke quantity output as excessive as double normal in persons with aortic regurgitation). As a consequence, the left ventricle dilates and cardiac output begins to fall; blood concurrently dams up within the left atrium and in the lungs behind the failing left ventricle. The left atrial pressure rises progressively, and at imply left atrial pressures above 25 to forty mm Hg, critical edema appears in the lungs, as discussed intimately in Chapter 39. This increased blood quantity will increase venous return to the heart, thereby serving to to overcome the effect of the cardiac debility. Therefore, after compensation, cardiac output may fall only minimally until the late levels of mitral valvular illness, even though the left atrial pressure is rising. As the left atrial pressure rises, blood begins to dam up within the lungs, eventually all the method in which back to the pulmonary artery. In addition, incipient edema of the lungs causes pulmonary arteriolar constriction. These two results collectively increase systolic pulmonary arterial pressure and likewise proper ventricular strain, generally to as excessive as 60 mm Hg, which is greater than double regular. This elevated pressure, in turn, causes hypertrophy of the proper side of the heart, which partially compensates for its increased workload. Therefore, either of those circumstances reduces net movement of blood from the left atrium into the left ventricle. Therefore, all of the dynamic abnormalities that occur in the various kinds of valvular heart disease turn into tremendously exacerbated. Even in persons with mild valvular coronary heart illness, during which the signs may be unrecognizable at rest, severe symptoms usually develop throughout heavy exercise. Also, in sufferers with mitral illness, train may cause a lot damming of blood within the lungs that severe or even lethal pulmonary edema may ensue in as little as 10 minutes. Therefore, the muscles of the body fatigue rapidly due to too little improve in muscle blood flow. There are three major kinds of congenital anomalies of the guts and its related vessels: (1) stenosis of the channel of blood move at some point in the heart or in a carefully allied main blood vessel; (2) an anomaly that permits blood to move backward from the left aspect of the center or aorta to the proper side of the center or pulmonary artery, thus failing to circulate through the systemic circulation, which is called a left-to-right shunt; and (3) an anomaly that enables blood to flow immediately from the best side of the heart into the left facet of the heart, thus failing to move by way of the lungs-called a right-toleft shunt. For occasion, congenital aortic valve stenosis leads to the same dynamic effects as aortic valve stenosis brought on by other valvular lesions, particularly, cardiac hypertrophy, heart muscle ischemia, reduced cardiac output, and a tendency to develop severe pulmonary edema. Another type of congenital stenosis is coarctation of the aorta, usually occurring close to the extent of the diaphragm. This stenosis causes the arterial stress within the higher a part of the body (above the extent of the coarctation) to be much higher than the stress within the lower body due to the good resistance to blood circulate via the coarctation to the lower body; a part of the blood should go across the coarctation by way of small collateral arteries, as discussed in Chapter 19. This mechanism permits instant recirculation of the blood by way of the systemic arteries of the fetus without the blood going through the lungs. Therefore, resistance to blood flow via the lungs is so nice that the pulmonary arterial stress is high in the fetus. Also, because of low resistance to blood flow from the aorta via the massive vessels of the placenta, the pressure within the aorta of the fetus is decrease than normal-in truth, decrease than within the pulmonary artery. This phenomenon causes almost all the pulmonary arterial 288 as a baby is born and begins to breathe, the lungs inflate; not only do the alveoli fill with air, but in addition the resistance to blood move through the pulmonary vascular tree decreases tremendously, permitting the pulmonary arterial strain to fall. Simultaneously, the aortic strain rises because of sudden cessation of blood circulate from the aorta via the placenta. As a end result, ahead blood flow via the ductus arteriosus ceases all of a sudden at start, and in fact, blood begins to flow backward via the ductus from the aorta into the pulmonary artery. However, because the youngster grows older, the differential between the high stress in the aorta and the lower pressure in the pulmonary artery progressively increases, with corresponding improve in backward circulate of blood from the aorta into the pulmonary artery. Also, the excessive aortic blood pressure normally causes the diameter of the partially open ductus to improve with time, making the situation even worse. This sound is rather more intense during systole when the aortic pressure is excessive and far less intense throughout diastole when the aortic stress falls low, in order that the murmur waxes and wanes with each beat of the center, creating the so-called machinery murmur. In fact, this procedure was one of the first successful coronary heart surgeries ever performed. Because the pulmonary artery is stenosed, much lower than regular amounts of blood move from the best ventricle into the lungs; as an alternative, a lot of the blood passes directly into the aorta, thus bypassing the lungs. Stenosis of pulmonary artery Aorta with a patent ductus, one half to two thirds of the aortic blood flows backward through the ductus into the pulmonary artery, then through the lungs, and eventually again into the left ventricle and aorta, passing through the lungs and left side of the heart two or more occasions for every one time that it passes through the systemic circulation. Indeed, early in life, the arterial blood is often better oxygenated than normal because of the additional instances it passes through the lungs. The main results of patent ductus arteriosus on the patient are decreased cardiac and respiratory reserve. The left ventricle is pumping about two or extra occasions the conventional cardiac output, and the maximum that it could pump after hypertrophy of the heart has occurred is about four to seven instances normal. Therefore, during train, the online blood circulate by way of the remainder of the physique can never increase to the degrees required for strenuous activity. With even reasonably strenuous train, the individual is more likely to turn out to be weak and may even faint from momentary coronary heart failure. The excessive pressures in the pulmonary vessels caused by excess move via the lungs may also result in pulmonary congestion and pulmonary edema. As a result of the extreme load on the center, and particularly as a end result of the pulmonary congestion becomes progressively extra severe with age, most patients with uncorrected patent ductus die from coronary heart illness between ages 20 and 40 years.
Discount zyloprim 300 mg without a prescriptionThe anteroinferior floor is roughened by the attachment of the medial thigh muscular tissues medications not to be taken with grapefruit buy zyloprim online. The smooth posterior floor is partly divided into perineal and pelvic areas, just like the inferior pubic ramus. The higher border completes the obturator foramen; the tough decrease border, along with the medial border of the inferior pubic ramus, contributes to the pubic arch. The fascia overlying the superficial muscle tissue of the perineum is attached beneath the ridge between the perineal and pelvic areas of the posterior floor of the ischial ramus. Above the ridge, areas give attachment to the crus of the penis or clitoris and the external urethral sphincter. The decrease border of the ramus provides an attachment for the fascia lata and the stratum membranosum perinei. Section 9 Bones ischial tuberosity the ischial tuberosity is divided practically transversely into higher and lower areas. The upper space is subdivided by an oblique line into superolateral and inferomedial elements. The lower area, narrowing because it curves on to the inferior ischial facet, is subdivided by an irregular vertical ridge into lateral and medial areas. The medial space is roofed by fibroadipose tissue that often incorporates the sciatic bursa of gluteus maximus, which helps the body in sitting. Medially, the tuberosity is limited by a curved ridge that passes on to the ramus and which gives attachment to the sacrotuberous ligament and its falciform process. The sacrospinous ligament is connected to its margins, separating the larger from the lesser sciatic foramen. The ligament is crossed posteriorly by the inner pudendal vessels, pudendal nerve and the nerve to obturator internus. Muscle attachments Part of obturator externus is connected to the decrease femoral floor of the ischial body. Part of obturator externus, the anterior fibres of adductor magnus and, close to the decrease border, gracilis are all connected to the anterior surface of the ischial ramus. Between adductor magnus and gracilis, the attachment of adductor brevis may descend from the inferior pubic ramus. The perineal space faces medially; its higher half is expounded to the crus of the penis or clitoris, and its lower part provides attachment to sphincter urethrae, ischiocavernosus and the superficial transverse perineal muscle. The upper area of the tuberosity is subdivided by an oblique line right into a superolateral part for semimembranosus and an inferomedial part for the long head of biceps femoris and semitendinosus. The lower area is subdivided by an irregular vertical ridge into lateral and medial areas. Superomedial to the tuberosity, the posterior surface has a wide, shallow groove, usually coated by hyaline cartilage, with a bursa between it and the tendon of obturator internus. Gemellus inferior is connected to the decrease margin of the groove, near the tuberosity. Forceful contraction of the hamstrings can lead to an avulsion fracture of the ischial tuberosity. The pelvic floor of the ischial backbone provides attachment to coccygeus and to essentially the most posterior fibres of levator ani. Obturator internus is connected to the upper a half of the graceful pelvic ischial surface and converges on the bony part of the lesser sciatic foramen, covering the rest of this surface apart from the pelvic side of the ischial spine; the muscle and its fascia separate the bone from the ischio-anal fossa. Branches of the obturator, medial circumflex femoral and inferior gluteal arteries provide the ischium. It is used here within the skeletal sense, to describe the irregular osseous girdle between the femoral heads and fifth lumbar vertebra. It is massive because its main perform is to withstand the forces of body weight and musculature. In this section, its obstetric, forensic and anthropological significance will be thought-about. The pelvis may be considered having higher and lesser segments, the true and false pelves. The segments are arbitrarily divided by an indirect aircraft passing via the sacral promontory posteriorly and the lineae terminales elsewhere. Each linea terminalis contains the iliac arcuate line, pectineal line (pecten pubis) and pubic crest. The pelvic brim is obstetrically important and has additionally long been measured for anthropological reasons, as has the pelvic cavity. This junctional zone is structurally large and forms powerful arches from the acetabular fossae to the vertebral column around the visceral cavity, which is a half of the stomach. The transverse diameter is the utmost distance between similar factors (assessed by eye) on opposite sides of the pelvic brim, and is on common 12. The oblique diameter is measured from the iliopubic ramus to the other sacroiliac joint, and is on common 12 cm in the adult male and 12. In kids, dimensions of the thorax and spine are considerably correlated with the width of the pelvic inlet, which are age-independent predictors of paediatric chest width and could additionally be helpful in assessing progress of the thorax and backbone in youngsters with early-onset spinal deformity (Emans et al 2005). The anteroposterior diameter is measured between the midpoints of the third sacral phase and posterior surface of the pubic symphysis, and is about 10. The transverse diameter is the widest transverse distance between the facet partitions of the cavity, and often the best transverse dimension in the whole cavity. The indirect diameter is the distance from the lowest point of one sacroiliac joint to the midpoint of the contralateral obturator membrane, and measures about eleven cm in the adult male and thirteen. Articulated bony pelvis the lesser pelvis encloses a real basin when gentle tissues of the pelvic flooring are in place. Of obstetric importance, it has a curved median axis, and superior and inferior openings. The pelvic floor, viscera and subjacent perineal sphincters shut the inferior opening. Pelvic outlet (inferior pelvic aperture) Cavity of the lesser pelvis the cavity of the lesser pelvis is brief, curved, and markedly longer in its posterior wall. Laterally on all sides, its margins are the graceful quadrangular pelvic side of the fused ilium and ischium. The region so enclosed is the pelvic cavity correct, via which pass Less common in define than the pelvic inlet, the pelvic outlet is indented behind by the coccyx and sacrum, and bilaterally by the ischial tuberosities. Posteriorly and laterally on each side are the sciatic notches between the sacrum and ischial tuberosities. Its anterior limbs are the ischiopubic rami (joined by the inferior pubic ligament) and its posterior margins are the sacrotuberous ligaments, with the coccyx in the midline. The outlet is thus not inflexible in its posterior half, being limited by ligaments and the coccyx, all barely yielding.
References - Cowan KN, Jones PL, Rabinovitch M. Elastase and matrix metalloproteinase inhibitors induce regression, and tenascin-C antisense prevents progression, of vascular disease. J Clin Invest 2000;105(1):21-34.
- Pinoli M, Marino F, Cosentino M. Dopaminergic regulation of innate immunity: A review. J Neuroimmune Pharmacol. 2017; 12(4):602-623.
- Keane MG, Pyeritz RE: Medical management of Marfan syndrome, Circulation 117:2802, 2008.
- Ma B, Landman EB, Miclea RL, et al. WNT signaling and cartilage: of mice and men. Calcif Tissue Int 2013; 92(5):399-411.
- Stinger HK, Spinella PC, Perkins JG, et al. The ratio of fi brinogen to red cells transfused affects survival in casualties receiving massive transfusions at an army combat support hospital. J Trauma. 2008;64:S79-S85.
- Taha MO, Miranda-Ferreira R, Paez RP, et al: Role of l-arginine, a substrate of nitric oxide biosynthesis, on intestinal ischemiareperfusion in rabbits. Transplant Proc 42:448, 2010.
|


