|
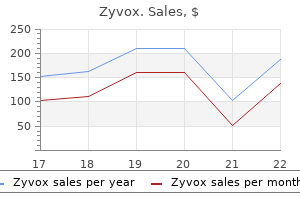
Zyvox dosages: 600 mg
Zyvox packs: 10 pills, 20 pills, 30 pills, 60 pills

Buy zyvox mastercardOther characteristic features are jitteriness and sympathetic overactivity (tachycardia, dilatation of pupils, and decreased bronchial and salivary secretions). Muscle tone is regular at rest, tendon reflexes are normoreactive or hyperactive, and ankle clonus is usually elicited. The Moro reflex is complete, and a single stimulus generates repetitive extension and flexion actions. Hypotonia is severe, and tendon reflexes, the Moro reflex, and the tonic neck reflex are absent as properly. Sucking and swallowing are depressed or absent, however the pupillary and oculovestibular reflexes are current. Generalized elevated intracranial pressure characterised by coma, bulging of the fontanelles, lack of pupillary and oculovestibular reflexes, and respiratory arrest typically develops between 24 and 72 hours of age. The encephalopathy begins to subside after the third day, and seizures decrease in frequency and eventually could cease. A bad end result is invariable if the amplitude remains suppressed for 2 weeks or a burst-suppression pattern is present at any time. Epileptiform exercise may also be present however is less predictive of the outcome than is background suppression. Clinical expertise indicates that management of seizures and upkeep of enough ventilation and perfusion will increase the prospect of a good end result. Seizures often stop spontaneously in the course of the second week, and long-term anticonvulsant therapy may not be needed. Organic Acid Disorders Characteristic of natural acid disorders is the accumulation of compounds, often ketones, or lactic acid that causes acidosis in biological fluids. The clinical displays differ significantly and several chapters comprise descriptions. Defects within the further metabolism of branched-chain amino acids are the natural acid problems that nearly all typically cause neonatal seizures. One is an acute, overwhelming disorder of the new child; the other is a persistent infantile kind. Newborns with the acute dysfunction are normal at delivery but inside a few days turn out to be lethargic, refuse to feed, and vomit. The survivors have a medical syndrome identical to the continual childish phenotype. Assays of isovaleryl-CoA dehydrogenase exercise utilize cultured fibroblasts, and molecular testing is out there. The medical phenotype correlates not with the share of residual enzyme exercise, but with the flexibility to detoxify isovaleryl-CoA with glycine. L-Carnitine, 50 mg/kg/day, is a helpful supplement to the diet of some youngsters with isovaleric acidemia. In acutely ill newborns, oral glycine, 250�500 mg/day, in addition to protein restriction and carnitine, lowers mortality. Arachidonic acid, docosahexaenoic acid, and vitamin B12 might turn into deficient and require supplementation in patients handled with dietary restriction of protein. Genetic transmission of the a number of defects on this pathway is by autosomal recessive inheritance. Propionyl-CoA, propionic acid, and methylmalonic acid accumulate and trigger hyperglycinemia and hyperammonemia. In 80% of these with full mutase deficiency, the symptoms seem during the first week after delivery; those with defects within the synthesis of adenosylcobalamin usually show symptoms after 1 month. Symptoms embody lethargy, failure to thrive, recurrent vomiting, dehydration, respiratory misery, and hypotonia after the initiation of protein feeding. Leukopenia, thrombocytopenia, and anemia are present in more than one-half of sufferers. Most die inside 2 months of analysis; survivors have recurrent acidosis, progress retardation, and cognitive impairment. Suspect the diagnosis in any newborn with metabolic acidosis, especially if associated with ketosis, hyperammonemia, and hyperglycinemia. Demonstrating an increased concentration of methylmalonic acid in the urine and elevated plasma glycine levels helps confirm the prognosis.
Discount 600mg zyvox visaHowever, the presence of muscle weak spot earlier than age 20 years is more likely to be relentlessly progressive, causing extreme distal weak point within the hands and toes by grownup life. Endocrine disturbances embody testicular atrophy, infertility in ladies, hyperinsulinism, diabetes, hypothyroidism, adrenal atrophy, and disturbances in growth hormone secretion. The foundation for the prognosis of myotonic dystrophy is usually the scientific features, the household historical past, and genetic evaluation. Studies to present the presence and number of trinucleotide repeats are commercially obtainable and are one of the best technique to detect asymptomatic people and best for prenatal prognosis. Myotonia frequently responds to drugs that stabilize membranes; mexiletine might be the best; procainamide, phenytoin, and carbamazepine are additionally helpful. Avoid statins, as they might increase weakness and pain, and vecuronium, which can cause malignant hyperthermia. The earliest characteristic of the illness is the event of contractures within the flexors of the elbows, the ankle tendon, and the extensors of the hand. This is followed by muscle weak point and wasting within the biceps and triceps muscular tissues, after which within the deltoid and different shoulder muscles. The development of symptoms is gradual, and the condition normally stabilizes by 20 years of age. In some sufferers, nevertheless, weak point progresses into grownup life and ambulation is finally misplaced. Bradycardia and syncope could precede muscle weakness or be delayed until the third decade. Female heterozygotes develop a cardiomyopathy late in life and require a pacemaker. Antithrombolytic brokers forestall stroke in patients with left ventricular dysfunction or arrhythmias. Avoid succinylcholine and halothane, which can enhance the chance of malignant hyperthermia. The mixture of acute weakness and rhabdomyolysis, as evidenced by myoglobinuria, indicates that muscle is degenerating quickly. This may occur in some issues of carbohydrate and fatty acid metabolism (see Chapter 8), after intense and unusual exercise, in some instances of infectious and idiopathic polymyositis, and in intoxication with alcohol and cocaine. Scapulo (Humeral) Peroneal Syndromes Progressive weak point and atrophy affecting the proximal muscle tissue of the arms and the distal muscular tissues of the legs could result from neuronopathy or myopathy. Ordinarily prodromal respiratory symptoms persist for 3�8 days before the onset of extreme symmetric muscle pain and weak spot, which can cause extreme disability inside 24 hours. Bed rest is required for 2�7 days till ache subsides, after which the patient recovers fully. Approximately 85%�90% of instances are demyelinating and 10%�15% are axonal in nature. This is especially necessary as a end result of the characteristic laboratory options may not be present on the onset of scientific symptoms. The two essential features are progressive motor weak spot involving a couple of limb, and areflexia. Frequently insidious sensory symptoms, usually ignored, precede the onset of weakness. These consist of fleeting dysesthesias and muscle tenderness in limbs which are soon to turn into paralytic. Weakness progresses rapidly, and roughly 50% of patients will reach a nadir by 2 weeks, 80% by 3 weeks, and the rest by four weeks. The weakness is normally ascending and comparatively symmetric qualitatively, if not quantitatively. Tendon reflexes are absent in all weak muscles and are absent even before the muscle is weak. Autonomic dysfunction (arrhythmia, labile blood strain, and gastrointestinal dysfunction) is usually associated, and a syndrome of acute autonomic dysfunction without paralysis may be a variant. Respiratory paralysis is uncommon, but by supporting respiratory perform during the important time of profound paralysis, full recovery is anticipated. At that time the concentration of protein could also be normal or elevated, and the number of mononuclear leukocytes per cubic millimeter may be 10 or fewer. Intubation is essential if vital capacity falls quickly to lower than 50% of normal.
Discount zyvox online master cardSurgery (systemic-to-pulmonary shunt or proper ventricular outflow repair) or interventional perforation and balloon dilatation of the pulmonary valve may be performed as soon as stability is achieved. Severe Ebstein malformation could present in the fetus with useful pulmonary atresia, proper ventricular myocardial illness, and duct-dependent pulmonary circulation. Enlargement of the right-sided cardiac structures and dilatation of the right atrium lead to lung hypoplasia and left ventricular dysfunction. The therapeutic objective is to scale back pulmonary vascular resistance by sufficient oxygenation and, if needed, by including inhaled nitric oxide. Maintaining ductal patency may be deleterious in some of these sufferers, and in some sufferers ductal closure has really improved hemodynamic stability30 by decreasing pulmonary vascular resistance and permitting the failing small right ventricle to produce antegrade flow to the lungs. Following the physiologic fall of pulmonary vascular resistance during postnatal transition, proper ventricular strain and volume load are reduced, and the best ventricle becomes capable of adequately serving the pulmonary circulation after a few days. If antegrade circulate across the pulmonary artery is established, the neonate could be steadily weaned off prostaglandins and air flow with out the necessity for further interventions. The neonate with congenital heart illness: Medical and interventional management magnitude of blending between both circulations. Intensive remedy includes upkeep of patency or reopening of the ductus arteriosus and creation of an unrestricted interatrial shunt by balloon atrioseptostomy. In transposition of the nice vessels, the left ventricle ejects into the pulmonary circulation by way of the pulmonary artery. As a result of the physiological reduction in the pulmonary vascular resistance, the left ventricular myocardial mass is subsequently decreased over time. Therefore, the anatomic correction has to be performed by an arterial change within the first 2�3 weeks after delivery to ensure a sufficiently developed and trained left ventricle. The clinical condition at arrival within the neonatal intensive care unit, together with metabolic acidosis and multiorgan failure, was considerably worse in the postnatally identified group. Prenatal diagnosis of transposition of the good arteries decreased postoperative mortality (0/68 neonates diagnosed prenatally versus 15/250 [6%] neonates recognized postnatally) and morbidity. The rider, nonetheless, is that there have been important preoperative variations with regard to earlier balloon atrioseptostomy and fewer neonates that required mechanical ventilation. Further research is required to confirm whether or not prenatal diagnosis confers long-term benefits. Methods Under ultrasound guidance or fluoroscopy, an uninflated balloon catheter is advanced via the right atrium and foramen ovale into the left atrium. The catheter may be launched by way of umbilical vein or femoral vein; both accesses are used relying on operator preference and affected person measurement. A profitable balloon atrioseptostomy ought to lead to an increased saturation (about 10% increase) or decreased interatrial gradient to roughly 3 mm Hg. Owing to a thick atrial septum and in different cardiac pathologies such as hypoplastic left coronary heart syndrome, a perforation by radiofrequency wire or a blade atrioseptostomy with or without stent placement may be required. The relevant dangers are blood loss, perforation, arrhythmia, and thromboembolism with subsequent cerebral infarction. Some reviews hyperlink embolic mind injury to balloon atrioseptostomy35,36 though this has been refuted by others. The mechanism of luminal enlargement by balloon dilatation may be difficult by tearing of the intima and media. This could lead to dissection of the intima and/or media and the next improvement of an aneurysm. Such mishaps should be avoided by acceptable choice of balloon diameter, inflation stress, balloon size, and compliance. Method the measurement of the annulus or vessel diameter is precisely outlined by echocardiography previous to the procedure and through angiography by the use of a calibrated markercatheter. Via a guidewire, the uninflated dilatation balloon is advanced to the stenotic vessel or valve. At probably the most slim position of the valve or vessel, the balloon is inflated underneath low stress.
Cheapest generic zyvox ukThe morphology of the arterial trunks is subsequent within the scope of study, followed by the description of the ventriculo-arterial junctions and the relationships of the arterial trunks to one another as they exit the ventricular mass. Morphologically proper atrium On outward look, many assume that the triangular tip of the best atrium is its appendage, when in reality the complete anterior wall of the proper atrium is the appendage. The appendage has a broad attachment to the smoothwalled venous element, this junction marked by the terminal groove. The superior and inferior caval veins serve as the systemic venous return with the venous return from the heart draining via the coronary sinus. The inferior caval vein and the coronary sinus be part of the best atrium inferiorly and alongside the diaphragmatic side. The superior caval vein joins the roof of the best atrium with the terminal crest crossing this junction anteriorly. The terminal crest is a distinguished muscle bundle on the inside surface of the proper atrium mendacity instantly adjoining to the above-mentioned terminal groove that marks the outward junction of the appendage with the venous part. Arising from the terminal crest are the pectinate muscles, which run in parallel fashion and extend laterally into the appendage. The pectinate muscles extend to the crux and into the diverticulum inferior to the orifice of the coronary sinus or the sub-thebesian sinus. The Eustachian and Thebesian valves take origin from the terminal crest and guard the openings of the inferior caval vein and the coronary sinus. The proper atrial vestibule is the slender, smooth-walled portion of the atrium that inserts into the hinge level of the tricuspid valve. The most constant morphological feature is the extent of the pectinate muscle tissue, that are sometimes confined to the appendage. The pulmonary veins enter the 4 corners of the roof of the smooth-walled vestibule, and the septal surface is fashioned by the flap valve at the ground of the oval fossa. The flap valve overlaps the outstanding superior interatrial fold and has a characteristic "horseshoe" appearance on this space. The left atrium has a significant body, which is the area becoming a member of the appendage, vestibule, and septum. The right ventricle is hypoplastic, the yellow arrows marking the anterior interventricular coronary artery. The pectinate muscle tissue arise from the terminal crest (red dots) and prolong across the atrioventricular junction. There is a narrow, clean vestibule (black double-headed arrows) that inserts into the hinge point of the tricuspid valve. The flap valve on the floor of the oval fossa is marked with black dots, and the right (black stars) and left (red star) pulmonary veins are simply appreciated. The morphologically proper ventricle the muscular walls of the best ventricle make up nearly all of the anterior aspect of the ventricular mass. The ventricles are assessed in a tripartite trend and are composed of an inlet, an apical trabecular component, and an outlet. The tricuspid valve guards the inlet, which extends from its hinge point to the attachments of the tendinous cords. The anterosuperior leaflet is supported by the anterior papillary muscle and the medial papillary muscle (muscle of Lancisi). Cardiac anatomy and examination of specimens Pulmonary valve Subpulmonary infundibulum Aortic valve 23 forming a real ring on the ventriculo-arterial junction. The pulmonary valve consists of three, semilunar leaflets that cross the ventriculo-arterial junction, incorporating a crescent of muscle at the base of each sinus. In the proper ventricle, the atrioventricular or tricuspid valve is separated from the arterial or pulmonary valve by the subpulmonary muscular infundibulum. Antero-superior leaflet the morphologically left ventricle the left ventricle has three elements simply as in the best ventricle: an inlet, an outlet, and an apical trabecular part. The mitral valve lies in the inlet, and it consists of two leaflets supported by tendinous cords that reach to two papillary muscle tissue. Each of the mitral valve leaflets is supported for probably the most half by tendinous cords that reach in a comparatively equal trend to every of the papillary muscular tissues. The apical trabecular element is the most constant part of the left ventricle. The aortic root marks the outlet of the left ventricle and is supported by muscle and fibrous tissue. The leaflets and sinuses of the aortic valve are named based on the origin of the coronary arteries from the aortic sinuses and with reference to their relative place to the pulmonary trunk.
Generic zyvox 600mg otcFluid in the fetal airways is removed both by expulsion via the mouth on account of chest compression, or by absorption into the pulmonary circulation with the onset of breathing. Regular ventilation is established, and the umbilicalplacental circulation is terminated by disruption or clamping of the umbilical cord. Ventilation by room air is associated with a rise in the alveolar oxygen concentration and also with the rhythmic bodily expansion of the lung and elimination of alveolar fluid. It has been difficult to assess the function of every of those elements in contributing to the circulatory changes related to birth, as a outcome of they occur nearly simultaneously. We developed a fetal lamb preparation to look at the role of particular person delivery occasions in these changes. All of the catheters had been exteriorized to the maternal flank, and the ewe and fetus have been allowed to recuperate from surgery. Fetal vascular pressures and blood gases had been monitored, and blood flows have been measured repeatedly by the radionuclide-labeled microsphere technique. The effect of rhythmic enlargement of the lung was assessed by ventilating the fetus with a gas mixture of 5% carbon dioxide, 3% oxygen, and 92% nitrogen. With the fetus nicely oxygenated, the impact of occluding the umbilical cord was then assessed. Only a minor proportion of blood ejected by the proper ventricle passed through the ductus arteriosus to the descending aorta, almost all being distributed to the pulmonary circulation. The massive venous return to the left atrium elevated left atrial stress above that in the systemic veins and proper atrium; this resulted in closure of the foramen ovale, with solely insignificant move from the best to the left atrium. The elevation in left atrial pressure resulting from elevated pulmonary venous return to the left atrium closes the foramen ovale. The cessation of umbilical venous return may also contribute to closure of the foramen. Constriction of the ductus arteriosus (vide infra) completes the separation between the left and proper sides of the guts and the major arteries, ensuing in the sequence circulation attribute of the grownup. Perinatal modifications within the pulmonary circulation Rhythmic bodily expansion of the lungs and a rise in oxygen levels in the ventilating gasoline combination have independent however complementary roles in pulmonary vasodilatation. Pulmonary arterial stress gradually and progressively decreased under aortic levels. This mirrored the separation of systemic and pulmonary arteries by constriction of the ductus arteriosus. It resulted in a modest increase in systemic arterial stress and a small increase in the shunt by way of the ductus arteriosus from the aorta to the Circulation within the normal fetus and cardiovascular diversifications to start with gas might contribute to a lower in pulmonary vascular resistance primarily based on bodily phenomena alone. During fetal life, the alveoli include fluid, and the optimistic pressure from the amniotic cavity is transmitted through the thorax to the lungs. This would tend to compress the pulmonary vessels alongside the alveoli and small bronchi. During supply of the fetus, airway fluid is eliminated; spontaneous breathing ends in the development of a unfavorable intrapleural stress, with a gradient from the airways outward to the pleura, and this tends to dilate pulmonary vessels. However, as proven experimentally in fetal lambs, positivepressure ventilation with no change in blood gas concentrations also reduces pulmonary vascular resistance. Physical factors that could presumably contribute to this are adjustments in floor forces on the alveoli. When the alveoli are crammed with gasoline, a powerful surface rigidity on the gas-fluid interface tends to collapse the alveoli. This would result in a force tending to dilate pulmonary vessels related to the alveoli, and thus lower pulmonary vascular resistance. The role of potassium channels within the response is supported by research in fetal lambs showing that potassium channel blockers trigger pulmonary vasoconstriction. Functional responses of the pulmonary circulation are significantly higher in the fetus than in the grownup, due to differences in morphology of the small pulmonary arteries. The pre-acinar arteries in the fetal lung have a thick wall with a prominent easy muscle layer. After birth, the pulmonary arterioles have a thinner muscular media as a outcome of a rise in lumen dimension.
Syndromes - Fundoscopy
- Prothrombin time
- AV malformation
- Fetal death
- Eat a balanced diet with extra whole grains, vegetables, and fruit, and less or no salt and sugar.
- Retinitis
- Testicular torsion
- Feel alone
- Partial or complete arm paralysis
- Fatigue
Discount zyvox master cardThe major type of cardiomyopathy consists within the majority of idiopathic cases,228 and genetic-metabolic, familial, and inflammatory issues had been additionally described. As in different illnesses, placentomegaly is likely to be an necessary issue for the maternal hyperdynamic and hypertensive state, the "mirror syndrome. In fetuses with sacrococcygeal teratoma, massive tumors with a high proportion of strong tissue demand high amounts of blood for supply of the tumor with nutrients and oxygen. Therefore, a high share of mixed cardiac output is sacrificed exclusively for the perfusion of the teratoma, causing excessive cardiac output; moreover, increased cardiac output may occur because of intratumoral arteriovenous shunting. Not so widespread is the following development of generalized hydrops fetalis and placentae being correlated with a really high spontaneous dying rate. In utero treatment of a fetus with a teratoma developing hydrops depends on a number of elements. In explicit, cases with a big intracorporeal portion compressing and displacing other organs have a poorer prognosis than cases with predominantly extracorporeal parts. In fetuses with a sacrococcygeal teratoma of the extracorporeal type, the presence of a completely solid tumor with its threat for malignancy and hypervascularization seems to be an important negative prognostic issue. Prenatal debulking of the tumor and devascularization in untimely fetuses with sacrococcygeal teratoma and subsequent hydrops could significantly reduce the cardiac output and may thus be the most effective remedy option prior to viability. However, open fetal surgical procedure is associated with major fetal and maternal dangers (preterm prelabor rupture of the membranes, preterm delivery, uterine scarring, and hemorrhage) and exhibits a excessive fetal mortality in already hydropic fetuses. However, if pregnancies difficult by high-risk sacrococcygeal teratoma will manifest indicators of fetal or maternal decompensation, or each, between 27 and 32 weeks of gestation, preemptive early supply results in surprisingly good outcomes in the absence of fulminant hydrops. In addition, anemia due to a Kasabach-Merritt sequence and/or hemorrhage might occur in these tumors and increase the excessive cardiac output state. Sinus venosus atrial septal defect with partially anomalous pulmonary venous return and discrete aortic coarctation are probably related to the increased blood move by way of the low resistance circuit of the vein of Galen early in gestation. Other examples of secondary dilated cardiomyopathies with extra direct myocardial injury may be observed in fetuses with infections, for example, coxsackievirus,302 adenovirus,303,304 and parvovirus B19,305�313 or by maternal autoantibody-induced myocarditis, largely related to atrioventricular block. A secondary cardiomyopathy of dilated but additionally hypertrophic kind can more regularly be found in the recipient twin of twin-twin transfusion syndrome and in fetuses with longstanding tachy- and bradyarrhythmia. In the recipient twin of continual fetofetal transfusion syndrome, increased pulsatility of the systemic veins suggests elevated central venous blood strain. Elevated afterload and preload by arterial hypertension and hypervolemia, respectively, trigger important ventricular pressure and volume load. Furthermore, transient hydrops and important increase of venous pulsatility could occur in some donor fetuses after laser coagulation for extreme twintwin transfusion syndrome and indicate a hemodynamic adaptation response following interruption of the transfusion course of. Massive bilateral and unilateral pleural effusion attributable to a localized and generalized lymphatic disorder, elevated venous stress, and cardiac compression resulting in generalized hydrops. Under these problems, primary hydrothoraces most regularly outcome from an area pleuromediastinal lymph vessel disturbance. More rarely presented are ailments with generalized lymphatic problems, as Noonan and a quantity of pterygium colli syndrome, congenital lymphedema syndrome, or congenital pulmonary lymphangiectasia. Large chest lots may trigger cardiac compression with low cardiac output state, and impairment of lymphatic and venous return. Cardiac compression, disturbance of venous return, and lymphatic tissue drainage with consecutive hydrops fetalis may be brought on by congenital excessive airways obstruction sequence, typically as part of Fraser syndrome. If fetal hydrops is related, further indicators of congestive heart failure are often identifiable. These include lowered ventricular fractional shortening, tricuspid and/or mitral valve regurgitation, and increased 574 Fetal Cardiology instances with unclear etiology. Therefore, aggressive in utero and perinatal administration must be rigorously thought of and will only be performed with informed consent by the extensively endorsed mother and father. On his proper aspect, the higher and the lower proper leg have been edematous and massively swollen by bony and soft tissue hypertrophy, as properly. Color Doppler imaging visualized hypervascularization and hyperperfusion of the right higher leg. Locally circumscribed or more general hyperechogenicity of the ventricular myocardium could counsel myocardial infection. In all circumstances of fetal cardiomyopathy, a detailed seek for the underlying disease should be performed, as a outcome of the precise diagnosis is the important thing to the prognosis, perinatal administration, and sufficient counseling of the mother and father.
Buy on line zyvoxThree histological variants exist: choroid plexus papillomas, atypical papillomas, and choroid plexus carcinomas. Choroid plexus papillomas are 5 times extra frequent than choroid plexus carcinomas. Choroid plexus tumors usually come up from the lateral ventricle, but also might occur within the third ventricle. If the tumor is pedunculated, its motion may cause intermittent ventricular obstruction by a ball-valve mechanism. The typical course is one of speedy progression, with just a few weeks from first symptoms to analysis. Infants with choroid plexus tumors have macrocephaly and infrequently are thought to have congenital hydrocephalus. Multilobular, calcified, contrast-enhancing intraventricular lots are characteristic of choroid plexus tumors. Congenital hydrocephalus occurs in approximately 1:1000 births and is generally associated with different congenital malformations. Based on the significant cognitive sequelae caused by irradiating the younger mind, a protocol of irradiation avoidance has been applied by the Head Start oncology consortium, consisting of maximal surgical resection adopted by excessive dose chemotherapy. The 3- and 5-year progression-free survival rates were 58% and 38%, and the general survival at three and 5 years was 83% and 62%. The frequent glial tumors of childhood so as of frequency are astrocytoma, ependymoma, and oligodendroglioma. Oligodendroglioma occurs completely in the cerebral hemispheres, whereas astrocytoma and ependymoma have either a supratentorial or an infratentorial location. The choroid plexus receives its blood provide from the anterior and posterior choroidal arteries, branches of the interior carotid artery, and the posterior cerebral artery. Yet the extent of surgical resection is the one most necessary issue that determines the prognosis of a choroid plexus papilloma. There are two autosomal dominant glioma-predisposing syndromes: tuberous sclerosis (subependymal large cell astrocytoma) and neurofibromatosis sort I (pilocytic astrocytoma of the optic pathway and hypothalamus). There are six epigenetically distinct subgroups of glioblastomas (K27, G34, receptor tyrosine kinase [M6], mesenchymal [M1/M2] and isocitrate dehydrogenase). The initial options of glial tumors in children depend upon location and may include seizures, hemiparesis, and motion disorders affecting one side of the physique. Tumors infiltrating the basal ganglia and internal capsule are much less more doubtless to trigger seizures than tumors nearer to cortical structures. A slow-growing tumor may not trigger a mass impact as a end result of surrounding neural structures accommodate infiltrating tumors. Such tumors may trigger solely seizures for a quantity of years earlier than inflicting weak spot of the contralateral limbs. The preliminary options in children with medullary tumors may be progressive dysphagia, hoarseness, ataxia, and hemiparesis. Cervicomedullary tumors cause neck discomfort, weakness or numbness of the palms, and an asymmetric quadriparesis. A mass impact collapses one ventricle, shifts midline structures, and places strain on the aqueduct. When herniation happens or when the lateral ventricles are dilated because of pressure on the aqueduct, the early options of headache, nausea, vomiting, and diplopia are followed by generalized weak spot or fatigability, lethargy, and declining consciousness. Other neurological findings depend upon the site of the tumor and will include hemiparesis, hemisensory loss, or homonymous hemianopia. High-grade gliomas have patchy areas of low and high density, typically proof of hemorrhage, and cystic degeneration. A mass effect occurs in half of low-grade astrocytomas and almost all high-grade tumors. Headache and nausea incessantly are relieved inside 24 hours; neurological deficits enhance as nicely. Recurrent tumors obtain carboplatin containing chemotherapy and/or conformal radiation therapy. Children with high-grade gliomas receive surgical resection with radiation therapy and presumably chemotherapy. Children with anaplastic astrocytomas have lower than a 30% 5-year survival price even with radiotherapy, and youngsters with glioblastoma multiforme have lower than a 3% 5-year survival.

Cheap zyvox 600 mg without prescriptionA Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts, Chapter 31, 3rd ed. A Practical Guide to Fetal Echocardiography: Normal and Abnormal Hearts, Chapter eight, 3rd ed. The left pulmonary artery may be seen originating from the principle pulmonary trunk beneath the ductus. As the video sweeps to the 4cv, we see the small, hypoplastic aortic root and aortic valve, in affiliation with a posteriorly malaligned ventricular septal defect, which is typical of this abnormality. However, the primary systematic investigation of fetal cardiac anatomy has now shifted in plenty of areas to the first and early second trimesters of pregnancy. Characteristic modifications in structural anatomy, once the province of the embryologist and pathologist, can now be imaged in great detail. The phrases sonoembryology 9 and embryography10 have been coined and used in this context. The level has been reached where embryonic development, somewhat than technical obstacles, is the limiting think about early imaging and detection of structural anomalies. Intrauterine, quite than postnatal, transfer improves neonatal situation for surgery and will reduce early morbidity and mortality. By fifty six days postfertilization, the fetal coronary heart is shaped and a four-chamber structure established. Several investigators have described regular fetal coronary heart anatomy in early gestation. The coronary heart steadily attains a tubular construction that resembles a triocular cavity at the finish of the 10th gestational week. The aorta could be seen on the finish of the ninth week, and by the top of the 12th week the brachiocephalic and carotid arteries are readily seen in each fetus. Linear correlation was discovered between gestational age and measurements of the proper and left ventricles. The ratio between the fetal heart and the transverse diameter of the chest was virtually constant at that interval. The advantage of those highfrequency transducers is the ability to provide a clearer image because of higher axial and lateral resolution,23,27 making small structures extra distinguishable. Certain views may be limited by the fixed linear axis of the ultrasound probe during the transvaginal examination, and fetal place often dictates the views that could be imaged. Consequently, certain maneuvers and manipulations are frequently wanted to be able to obtain one of the best planes and views in an inexpensive examination time. The institution of stomach situs and cardiac position should be the first step within the evaluation of the fetal cardiovascular system. The shade image exhibits the trachea, coronary heart and great vessels, liver, and stomach with the 5 planes of insonation superimposed. The ventricles are also approximately equal in dimension, with the morphological proper ventricle distinguished by the attribute moderator band at the apex. While some disparity in ventricle measurement may be normal significantly in late gestation, marked distinction in size ought to elevate suspicion of such defects as hypoplastic left coronary heart or coarctation of the aorta. The utility of including the outflow tracts to fetal heart screening is nicely established within the literature,54,69�75 supported by worldwide pointers,56,fifty seven,sixty one and has been shown to increase anomaly detection, 54,55,70,76,seventy seven significantly in (b) left. Abnormalities in cardiac situs, axis, or place require detailed evaluation for situs abnormalities, and structural or chromosomal anomalies. In addition, a shift in cardiac position can be indicative of space-occupying lesions or diaphragmatic hernia. In most circumstances, the pulmonary veins could be seen at their entry into the left atrium. In this aircraft, the pulmonary artery is seen originating from the morphologic proper ventricle. Diagnostic early echocardiography Diagnosis of cardiac anomalies follows the segmental approach to fetal echocardiography. At the top of the first trimester, a number of abnormal connections of the fetal venous system are acknowledged and are categorized as follows: pathologies of the cardinal vein, umbilical veins, vitelline veins, and anomalous pulmonary venous connections. One of the biggest sequence, together with 12,793 sufferers over a 5-year interval, originated in Israel and was reported by Bronshtein et al.
Discount zyvox 600mg free shippingDuring the first months, the skin might have a musty odor due to phenylacetic acid in the sweat. Developmental delay is typically obvious by the third month and always before the end of the primary 12 months. Behavioral disturbances characterised by hyperactivity and aggressiveness are frequent; focal neurological deficits are unusual. Plasma amino acid analysis together with phenylalanine concentration, phenylalanine to tyrosine ratio, and an entire amino acid profile confirms the prognosis. Plasma phenylalanine concentrations above a thousand mol/L within the untreated state are diagnostic. The use of molecular genetic testing is primarily for genetic counseling and prenatal testing. Blood phenylalanine levels lower than 25 mg/dL and a traditional focus of tyrosine characterize benign variants of phenylketonuria. Disturbances in tetrahydrobiopterin underlie the malignant forms of phenylketonuria. Seizures are the initial symptom and cognitive impairment and motor deficits come later. Transitory tyrosinemia occurs in 2% of full-term newborns and in 2% of untimely newborns. Recent research counsel that the plasma phenylalanine goal must be 240 mol/L to anticipate normal neurocognitive outcomes. Disorders of Lysosomal Enzymes Lysosomes are cytoplasmic vesicles containing hydrolytic enzymes that degrade the products of mobile catabolism. The causes of lysosomal enzyme issues are impaired enzyme synthesis, abnormal enzyme focusing on, or a defective accent issue wanted for enzymatic processing. When lysosomal enzymes are impaired, irregular storage of supplies happens inflicting cell damage and death. Cognitive impairment and regression are features of many lysosomal enzyme storage ailments. In some diseases, similar to acid lipase deficiency (Wolman disease) and ceramide deficiency (Farber lipogranulomatosis), cognitive impairment occurs, however is neither a outstanding nor an initial function. Deficiency of the enzyme glucocerebrosidase (glucosylceramide -glucosidase) causes the lysosomal storage of glucocerebrosides. While Gaucher illness encompasses a continuum of scientific findings, the identification of five clinical subtypes is useful in figuring out prognosis and management. Head retraction, an early and characteristic sign, probably is due to meningeal irritation. Difficulties in sucking and swallowing, trismus, and oculomotor palsies are typical. Assay of acid -glucosylceramidase enzyme activity in peripheral blood leukocytes or different nucleated cells is reliable for analysis. Glucosylceramidase enzyme activity in peripheral blood leukocytes is 0%�15% of normal. Molecular genetic testing is available, however biochemical testing may still be required to confirm the diagnosis. Symptomatic therapy for Gaucher disease includes partial or whole splenectomy for large splenomegaly and thrombocytopenia, transfusion of blood for severe anemia and bleeding, analgesics for bone ache, joint substitute surgery for reduction from chronic pain and restoration of operate, and supplemental therapy corresponding to oral bisphosphonates for severe osteopenia. Enzyme alternative therapy, utilizing imiglucerase, is effective in reversing the hematological and liver/ spleen involvement. Within 2�4 months, the infant is in a everlasting place of opisthotonos and all previously achieved milestones are lost. Blindness happens, and earlier than 1 12 months 90% of those infants are both lifeless or in a continual vegetative state. Several variant forms of globoid leukodystrophy with different medical features exist: childish spasm syndrome (see Chapter 1), focal neurological deficits (see Chapters 10 and 11), and polyneuropathy (see Chapter 7). Deficient activity of galactocerebrosidase in leukocytes or cultured fibroblasts establishes the prognosis. Several states are considering including Krabbe illness to the standardized newborn screen. Hematopoietic stem cell transplantation slows the course of disease in children with infantile-onset Krabbe illness identified before symptom onset.
600mg zyvox free shippingWhile there would be the inevitable requirement for pulmonary homograft replacement with growth, encouraging early expertise with this process obliges us to consider its adoption when primary palliation fails. Surgical palliation is both by the "Norwood" route or primary cardiac transplantation. Classically, the Norwood procedure was carried out with a Blalock-Taussig shunt offering pulmonary blood move,19 although many now use a right ventricular to pulmonary artery conduit (Sano shunt 20) instead. The relative benefits of these approaches remain disputed; overall survival for standard surgery is at present 86%�92%. Comparing typical surgical procedure to major cardiac transplantation, data show that related results can be achieved with both technique in units with adequate exercise,21 though some units report one hundred pc survival for a hybrid approach of shortterm interventional palliation followed by transplantation. This involves stenting the ductus arteriosus, banding the department pulmonary arteries, and reaching an unrestrictive interatrial communication. Originally attempted in 199723 with poor outcomes, there has lately been a revival in interest with considerably improved outcomes. When performed in facilities with in depth experience, the results are on par with surgery24�26; it should be noted that the crude knowledge appear poorer, but many facilities reserve a hybrid approach for higher-risk people with significant comorbidities (low birth weight, intestine ischemia, cerebral bleeds, and so on. The hybrid method also has the advantage of permitting simple transference between single- and two-ventricle circulations if the preliminary assessment suggests that the left ventricle is of borderline measurement. However, the second-stage process following preliminary hybrid palliation is a tour de force. Long-term survival and freedom from reintervention at 10 years are 70%�100%29,30 and 50%� 79%,29,31 respectively, with 2. Therefore, after resuscitation using prostaglandin to maintain the arterial duct, surgical restore should be undertaken. For a single-stage approach, early mortality is 0%�12% and late mortality 20%�25%, 32,33 even in small, untimely infants, compared to 8%�37% and 4%�26%, 32,34,35 respectively, for the two-stage approach, though it should be emphasized that these outcomes pertain to totally different surgical eras. When left ventricular outflow tract obstruction is also famous at presentation, the surgical threat is considerably greater, with 42% early and 50% late mortality. Current surgical apply is to restore the arch using an end-to-side anastomosis, having excised all ductal tissue, although an augmented subclavian/carotid flap may be useful significantly in advanced interrupted aortic arch (such as with truncus arteriosus). The repair is accomplished using a conduit between the best ventricle and pulmonary artery. In milder types, when assessment concludes that mitral valve measurement is sufficient for a two-ventricle restore, the choices are balloon valvuloplasty or surgical repair. Which therapy is best is uncertain, as balloon 756 Fetal Cardiology where the prevailing philosophy advocates initial palliation, a Blalock-Taussig shunt is carried out. In some sufferers, the pulmonary arteries are severely hypoplastic or absent, and the patient might have main aortopulmonary collateral arteries. Using such methods, full correction might later be achieved in up to one hundred pc of patients51; small collateral vessels might later be coiled by interventional catheter techniques. For kids in whom pulmonary blood move is primarily depending on major aortopulmonary collateral arteries somewhat than native pulmonary arteries, afferent conduits to the lungs must be constructed from the collaterals, a course of known as "unifocalization. This maximizes the opportunity for sufficient vessel growth and may be achieved in as much as 90% of patients55 with an early mortality of 3%�10. However, owing to poorly developed collateral vessels, some patients still require staged unifocalizations by way of thoracotomies. If the coarctation is unsuspected, the infant might current in extremis with low cardiac output and extreme metabolic acidosis. While this temporizing measure often allows recovery from the consequences of hypoperfusion, this is an unstable circulation, and any benefit derived shall be short-lived; definitive therapy should therefore not be imprudently delayed. The optimum definitive administration of native aortic coarctation remains controversial. Balloon aortoplasty of native aortic coarctation has shown a 91%�100% primary success price. However, for recoarctation following primary surgical restore, balloon aortoplasty is now the treatment of selection, with an 88%�91% success price. Historically, surgery has been the mainstay of therapy; patch aortoplasty, subclavian flap aortoplasty, and coarctation resection with end-to-end anastomosis have been used.
|