|
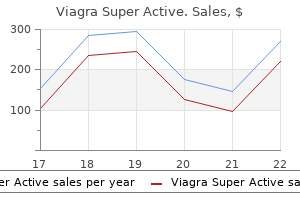
Viagra Super Active dosages: 100 mg, 50 mg, 25 mg
Viagra Super Active packs: 10 caps, 30 caps, 60 caps, 90 caps, 120 caps, 180 caps, 270 caps, 360 caps

Cheap viagra super active 50 mg fast deliveryThe check has been very helpful for the evaluation of sufferers with forearm dystonia (36�39). Appropriate methodological suggestions have been put ahead by Fuhr and Hallett (40). A low intensity electrical stimulus given to the nerve from the medial gastrocnemius muscle will, subsequently, activate the Ib afferents. The subsequent activation of the Ib inhibitory interneuron will trigger disynaptic inhibition on the soleus motoneurons. This takes place within the form of a small lower of the amplitude of the soleus H reflex between 4 and 6 ms after the medial gastrocnemius nerve stimulus. According to Zher and Stein (51), the increase in the measurement of the H reflex related to a remote muscle contraction is, partly as a outcome of elimination of presynaptic inhibition. Many research have examined the physiology of the H reflex modifications preceding a voluntary motion in response time experiments. The H reflex enhancement previous to a response is expounded to the motor instructions issued for the precise motion execution, quite than to any sensory suggestions alerts. This is probably the consequence of a rise in the excitability of the soleus motoneurons, with a concomitant improve in the quantity of presynaptic inhibition of the Ia afferent terminals. The dimension of the soleus H reflex can also be modulated during strolling, with facilitation within the stance section and inhibition within the swing section (58�60). Pierrot-Deseilligny and Bussel (45) devised an electrophysiological method to assess recurrent inhibition with the soleus H reflex. The method requires a stimulator able to delivering two stimuli of different intensity through the same pair of electrodes. The first stimulus is of low intensity, able to inducing a small amplitude H reflex (H1). The second stimulus, delivered 10�15 ms later, ought to be of supramaximal intensity. Because of that, all motor axons shall be depolarized and an antidromic volley might be generated. At that time, the orthodromic volley generated in a few motoneurons by the preceding stimulus, that would give rise to the H1, shall be travelling in a couple of motor axons and collide with the antidromic impulses. This decrease is as a result of of the effects of Renshaw cell activation on the motoneuron pool involved in the generation of H1. Renshaw cells inhibit the homonymous motoneuron, different neighbouring motoneurons, and in addition the Ia inhibitory interneurons projecting to the antagonist muscle (47). Presynaptic inhibition is mediated by an axo-axonal synapse on Ia afferent terminals themselves. In contrast to the opposite spinal mechanisms of motor control mentioned so far, presynaptic inhibition takes place at a presynaptic stage, due to this fact, leaving the motoneuron uninfluenced. Methods for electrophysiological testing of presynaptic inhibition contain activation of the Ia afferents of the identical muscle by means of vibration (46,48). Vibratory stimulation at the Achilles tendon depolarizes Ia afferent fibres, which trigger inhibition of the soleus H reflex and, at the same time, tonic activation of motoneurons (the tonic vibration reflex). Vibration-induced presynaptic inhibition may be overcome by muscle contraction, for example of the management of supraspinal buildings on spinal interneurons. As described in a earlier paragraph, presynaptic inhibition is a crucial technique of the central nervous system for management of reflexes. H reflex excitability changes after distant exterior stimuli External activation of the reticulospinal tract by auditory stimuli has been reported to cause enhancement of the soleus H reflex by several authors. These authors reported the synchronization of hopping with the robust beats of the musical piece, in such a means that the motor events were timed to make greatest use of the auditory facilitation of the segmental reflex. Delwaide and Schepens confirmed the discovering of Rossignol and Melvill-Jones (61), and reported that such facilitation was irregular in patients with reticulospinal tract dysfunction (62). Finally, activation of the corticospinal tract with cortical stimulation causes additionally modulation of the soleus H reflex. This was attributed to the truth that corticospinal projections to the soleus muscle are primarily inhibitory. Electrical or mechanical stimuli utilized wherever within the body are also capable of inducing modifications in the measurement of the soleus H reflex. Gassel and Ott (64) confirmed that cutaneous stimuli of the dorsal and plantar surfaces of the distal foot in humans induced reverse effects on the soleus H reflex, with brief latency facilitation with stimulation of the dorsum, and inhibition with plantar stimulation. Remote contraction of a muscle induces facilitation of each the tendon jerk and the H reflex (49�51).
Discount viagra super active online mastercardNormal conduction velocities within the sinus node are slow (2 to 5 cm/sec), thus increasing the likelihood of intranodal conduction block. The sinus node is insulated electrically from the surrounding atrial myocytes, besides at a limited number of preferential exit sites. Neural and hormonal elements influence both the site of pacemaker activation, doubtless via shifting factors of preliminary exercise, and the purpose of exit from the sinus node advanced. At sooner rates, the sinus impulse originates in the superior portion of the sinus node, whereas at slower charges, it arises from a more inferior portion. Furthermore, preferential pathways of conduction were additionally discovered to exist between the sinus node and the atrial exit websites, thus doubtlessly contributing to the multicentricity of the sinus node complex. The blood provide predominantly comes from a large central artery, the sinus nodal artery, which is a branch of the best coronary artery in 55% to 60% of sufferers, and from the circumflex artery in 40% to 45%. Distention of the artery slows the sinus fee, whereas collapse causes an increase in price. Enhanced vagal exercise can produce sinus bradycardia, sinus arrest, and sinoatrial exit block, whereas increased sympathetic activity can enhance the sinus fee and reverse sinus arrest and sinoatrial exit block. Sinus node responses to brief vagal bursts start after a short latency and dissipate shortly; in contrast, responses to sympathetic stimulation begin and dissipate slowly. The speedy onset and offset of responses to vagal stimulation permit dynamic beat-to-beat vagal modulation of the heart price, whereas the gradual temporal response to sympathetic stimulation precludes any beat-to-beat regulation by sympathetic exercise. Transient slowing of the sinus rate or sinus arrest can complicate acute myocardial infarction, which is normally seen with acute inferior wall infarction and is caused by autonomic influences. Possible mechanisms for sinus bradycardia after an acute myocardial infarction include neurological reflexes (Bezold-Jarisch reflex), coronary chemoreflexes (vagally mediated), humoral reflexes (enzymes, adenosine, potassium [K+]), oxygenconserving reflex ("diving" reflex), and infarction or ischemia of the sinus node or the surrounding atrium. Most commonly related to this complication is the Mustard procedure for transposition of the good arteries and repair of atrial septal defects, especially of the sinus venosus type. In explicit, downregulation of the funny current (If) and malfunction of the calcium (Ca2+) clock (characterized by reduced sarcoplasmic reticulum Ca2+ release and downregulated ryanodine receptors in the sinus node) appear to account largely for atrial tachycardia�induced reworking of sinus node. The transformed atria are related to extra caudal activation of the sinus node complex, slower conduction time along preferential pathways, and solely modest shifts inside the useful pacemaker complicated. Drugs can alter sinus node function by direct pharmacological results on nodal tissue or not directly by neurally mediated effects. Hypervagotonia may be seen in hypersensitive carotid sinus syndrome and neurocardiogenic syncope. Well-trained athletes with increased vagal tone often may require some deconditioning to assist forestall symptomatic bradyarrhythmias. Patients typically are asymptomatic or have signs which would possibly be delicate and nonspecific, and the intermittent nature of these symptoms makes documentation of the related arrhythmia difficult at occasions. Symptoms, which may have been current for months or years, embrace paroxysmal dizziness, presyncope, or syncope, which are predominantly associated to extended sinus pauses. Episodes of syncope are often unheralded and can manifest in older patients as repeated falls. More delicate signs include gentle digestive disturbances, periodic oliguria or edema, and delicate intermittent dyspnea. The worst prognosis is related to the tachycardia-bradycardia syndrome (mostly because of the danger for thromboembolic complications), whereas sinus bradycardia is far more benign. In sufferers with frequent symptoms, 24- or 48-hour ambulatory Holter monitoring could be useful. Cardiac occasion monitoring or implantable loop recorders may be essential in patients with less frequent signs. Heart price response to the Valsalva maneuver (normally decreased) or upright tilt (normally increased) can be used to confirm that the autonomic nervous system itself is intact. Complete pharmacological autonomic blockade is used to determine the intrinsic heart price (see later). Exercise testing to assess chronotropic incompetence is of worth in sufferers with exertional symptoms (see later). Sinus bradycardia slower than forty beats/min (not related to sleep or bodily conditioning) is generally considered abnormal.
Syndromes - Vitamin E
- Apathy
- Urine pH
- Electroencephalogram (EEG)
- Night sweats
- Did the chills happen only once, or are there many separate occurrences (episodic)?
- Disfigurement
- Premature abdominal fullness after meals
Buy cheapest viagra super active and viagra super activeDetailed voltage maps extend the process time and falsely low voltage measurements (caused by suboptimal catheter contact) can lead to incorrect scar definition. Additionally, small areas of scar is most likely not detected, given the spatial resolution of at least 5 mm, covered by the 3. These imaging approaches can be used to accurately predict irregular voltage locations upfront of the mapping process, which can allow the electrophysiologist to think about areas of probably myocardial scar, obviate the need to carry out a whole point-by-point voltage mapping, determine falsely lowvoltage recordings in areas of regular perfusion because of suboptimal catheter contact, in addition to scale back procedure time and fluoroscopic publicity. Additionally, some imaging modalities are capable of characterize the transmural extent and intramyocardial location of scar tissue, which might doubtlessly assist to identify intramural and epicardial arrhythmia substrate, overcoming a limitation of endocardial voltage mapping. Alternatively, a quantity of factors may be acquired at totally different planes of the aorta because the catheter is dragged alongside the descending aorta, arch, and ascending aorta. Images are acquired in finish expiration and gated to the R wave or the pacing spike. Akinetic and thinned wall segments are marked in a separate quantity and labeled as scar on the ultrasound quantity map. Primary registration is carried out with landmark points and visible alignments, as previously discussed. At leftis a snapshot of theactivationwavefront projected on the endocardial floor (white = activation). At proper is similar immediate of activation in a cutaway view, showing the wireframe of the endocardial balloon-based electrode array. Sites of mid-diastolic endocardial exercise, which are probably adjacent to reentry circuit exits, are usually identifiable; in some circumstances, isthmuses may be recognized. The shade scale is adjusted to create a binary display, with unfavorable unipolar potentials in white on a purple background, producing a unipolar activation map. Diastolic activity and exit websites are then marked on the digital endocardium, and the mapping catheter is navigated to them by the locator. Until further studies define the right dynamic substrate mapping share that can be in contrast with the scar and scar border zone defined by contact mapping, areas having values less than 50% could additionally be defined as "abnormal myocardium. The guidewire is then withdrawn and the balloon inflated with a contrast-saline combination. High-pass filters are adjusted at the lowest value that minimizes the shift of the isoelectric baseline to keep away from confusing depolarization with repolarization. Projection of the virtual endocardial electrograms over this space is performed at completely different high-pass filter settings (1, 2, 4, eight, 16, and 32 Hz) to avoid misinterpretation with repolarization waveforms. Very low-amplitude alerts will not be detected, particularly if the space between the middle of the balloon catheter and endocardial surface exceeds 40 mm, limiting the correct identification of diastolic alerts. Additionally, detection and show of activation from two adjoining buildings, such because the papillary muscle and subjacent myocardium, is problematic. Care has to be taken to affirm that the digital electrogram is expounded to local activation and not baseline drift or repolarization. Poles 1 to 3 (distal) and a pair of to 4 (proximal) of the ablation catheter are used for recording, and poles 1 to 3 are used for stimulation. Three-dimensional electroanatomical mapping is usually used to aid mapping and ablation. During activation mapping, explicit websites of curiosity are sought, together with the next: (1) sites with irregular local bipolar electrogram (amplitude 0. Filtered unipolar electrograms can help ensure that the tip electrode, which is the ablation electrode, is answerable for the early part of the bipolar electrograms. Infarct areas are sought first and more data points are acquired round these areas. Sites with fractionated electrograms, multipotential electrograms, and/or isolated diastolic electrograms are tagged and catalogued on the 3-D mapping system for future revisiting and steerage. The greater the diploma of concordance between the morphology throughout pacing and tachycardia, the closer is the catheter to the exit website of the tachycardia isthmus. Additionally, intravenous procainamide (infused with a maximal loading dose of 15 mg/kg at a rate of 50 mg/min, followed by a steady infusion at a maximal fee of 0. These sites are tagged and catalogued by the 3-D mapping system for future revisiting and guidance.
Generic 100mg viagra super activeAn outbreak of mediastinitis amongst heart transplant recipients apparently associated to a change within the United Network for Organ Sharing pointers. Major infection after pediatric cardiac surgical procedure: external validation of threat estimation model. Risk factors and risk adjustment for surgical site infections in pediatric cardiothoracic surgical procedure patients. Delayed sternal closure after pediatric cardiac operations; single middle expertise: a retrospective research. Postoperative mediastinitis in kids: epidemiology, microbiology, and risk components for gram-negative pathogens. A hospital-acquired outbreak of methicillin-resistant Staphylococcus aureus infection initiated by a surgeon service. The relationship between the nasalstaphylococcal-carrier state and the incidence of postoperative complications. Coagulase-negative staphylococci isolated from sternal wound infections after cardiac surgical procedure: attachment to and accumulation on sternal fixation chrome steel wires. Risk components for postoperative mediastinitis as a end result of methicillin-resistant Staphylococcus aureus. Staphylococcus aureus poststernotomy mediastinitis: description of two distinct acquisition pathways with different potential preventive approaches. Multiply betalactam resistant Enterobacter cloacae infections linked to the environmental flora in a unit for cardiothoracic and vascular surgery. Outbreak of invasive aspergillosis after major heart surgical procedure caused by spores within the air of the intensive care unit. Effect of time to onset on scientific features and prognosis of poststernotomy mediastinitis. Mediastinitis after cardiac surgical procedure: improvement of bacteriological analysis by use of multiple tissue samples and pressure typing. Descending necrotizing mediastinitis: two case reports and evaluate of the literature. Critical care transesophageal endosonography and guided fineneedle aspiration for analysis and administration of posterior mediastinitis. Perforation of the esophagus: correlation of site and trigger with plain movie findings. Low mortality after remedy for esophageal perforation: a single-center expertise. Procalcitonin for differential diagnosis of graft rejection and infection in patients with coronary heart and/or lung grafts. Accuracy of blood tradition for early analysis of mediastinitis in febrile patients after cardiac surgical procedure. Detection of mediastinitis after coronary heart transplantation by gallium-67 scintigraphy. Diagnosing sternal wound infections with 99mTc-labeled monoclonal granulocyte antibody scintigraphy. Role of epicardial pacing wire cultures in the analysis of poststernotomy mediastinitis. Usefulness of routine epicardial pacing wire culture for early prediction of poststernotomy mediastinitis. Report of a case of spontaneous perforation of the oesophagus efficiently handled by operation. Selective nonoperative management of contained intrathoracic esophageal disruptions. Endoscopic clips for closing esophageal perforations: case report and pooled analysis. Systematic review: momentary stent placement for benign rupture or anastomotic leak of the oesophagus. Conservative approach to the mediastinitis in childhood secondary to esophageal perforation. Transcervical drainage for descending necrotizing mediastinitis may be sufficient.
Order 25 mg viagra super active with amexIt is well-known that thermal injury produces denaturation of extracellular proteins, particularly collagen. Thermally induced collagen shrinkage has been nicely documented in animal and human studies. This is brought on by a decline in the arteriovenous gradient in addition to compression by the growing tissue edema. As a consequence, the concerned alveoli are affected by the ensuing ischemia and surrounding edema, resulting in atelectasis, infarction, or susceptibility to infections. With the resulting alterations in pulmonary hemodynamics, redistribution of blood flow occurs with the opening of vascular channels or neovascularization by which tissue hypoxia is understood to play a job. Hence, the venous drainage of the affected section becomes mainly dependent on the ipsilateral veins draining the wholesome lobes. If the ipsilateral vein(s) can also be stenosed, the impedance to the pulmonary circulate increases, including to the hemodynamic burden. Color flow distinction imaging can be helpful for identifying the location of the orifice of essentially the most tightly stenotic vessels. Chest radiography often reveals parenchymal consolidation, pleural effusion, or both. Ventilation/perfusion scanning may be done to characterize the useful significance of the stenosis. A excessive degree of suspicion is important to avoid performing misleading diagnostic procedures and to enable proper and immediate management. The preliminary manifestation is generally dyspnea on exertion, which usually evolves over the course of 1 to three months. Both pleuritic chest pain and hemoptysis are doubtless associated to full vessel or branch occlusion. Symptoms could improve spontaneously over time in a big share of sufferers. In one report, this improvement occurred in 50% of sufferers and was all the time associated to improvement within the radiological abnormalities beforehand detected,although other hemodynamic compensatory mechanisms. It can be important to think about the age, functional capability, and associated comorbidities in addition to anatomical and technical elements pertaining to the stenotic vein when making a choice concerning interventional therapy in asymptomatic sufferers. Unfortunately, both in-stent and in-segment restenosis can recur in as much as 61% of sufferers, and repeat intervention is warranted in symptomatic sufferers. The risk of esophageal damage likely is enhanced by rising the magnitude and duration of local tissue heating. The presenting signs can include hematemesis, sepsis, or air embolization and stroke. The leading symptom of esophageal perforation is excessive fever or severe chest or epigastric pain. The dramatic neurological issues occur with a delay of no less than a couple of hours after the first symptoms. Endoscopy is a diagnostic modality that should be averted as a result of insufflation of the esophagus with air can lead to a devastating cerebrovascular accident and death secondary to a big air embolus. Immediate surgical procedure (within a quantity of hours after the primary symptoms) can doubtlessly stop neurological problems and presumably end in a high survival fee, without residue. However, due to the rarity of this complication, it stays unproven whether or not the use of these approaches lowers or eliminates the chance of esophageal perforation or fistula formation, and the optimal approach has not but been decided. Radiation exposures during the totally different interventional procedures are extremely variable. Cardiac catheterizations typically expose patients to a median dose of 250 rad (2. Percutaneous coronary interventions are notably harmful (average dose, 640 rad [6. Although these symbolize commonplace exposure estimates, interventional procedures are extremely variable. This discovering is putting and speaks to the effectiveness of the techniques that use a number of technologies to reduce radiation exposure, such as final image hold, pulsed fluoroscopy, and extra filters. The threshold for transient erythema and epilation is 2 to 3 Gy, for acute pores and skin harm is 2 to eight Gy, and for chronic radiation injury is 10 Gy.
Proven viagra super active 100 mgThe physiological part cancellation affects muscle responses relatively little as a outcome of, with the same slight shift in latency, longer period motor unit potentials nonetheless superimpose nearly in part rather than out of section (15). In evaluating peripheral neuropathies with segmental block, the dimensions of the recorded response serves as a measure of the variety of excitable nerve axons. In a demyelinating neuropathy, an extended length motor response additionally diminishes dramatically merely due to part cancellation between normally conducting and pathologically sluggish fibres (15). This sort of section cancellation reduces the amplitude of the muscle response properly past the standard physiological limits, giving rise to a misunderstanding of motor conduction block. A maximal phase cancellation outcomes from a latency shift within the order of onehalf the total duration of unit discharge. With further separation, extreme desynchronization might now counter the physiological section cancellation, generally paradoxically growing the scale of the response. The generally used criteria based on share discount to distinguish pathological from physiological temporal dispersion really holds only in completely standardized studies because variables such as the interelectrode distance between the 2 recording electrodes influences the result substantially (100). As an alternative means, segmental stimulation at greater than two websites enable testing the linear relationship between the latency and the dimensions of the recorded responses in physiological phase cancellation (101). Composite scores as opposed to individual values could improve sensitivity and reproducibility of nerve conduction abnormalities (95). Clinical assessment of conduction block Criteria for conduction block A disproportionately small compound muscle action potential elicited by proximal as in contrast with distal stimulation serves as a measure of conduction block. This discovering often suggests a demyelinating lesion, though it might outcome from different reversible Table 6. Amplitude of the evoked response, measured from the baseline to the unfavorable peak. Latency, measured to the onset of the evoked response, with a standard distance of seven cm between the cathode and the recording electrode. The combination of clinical and electrophysiological findings delineates motor conduction block extra conclusively (105). A vigorous twitch and a large amplitude response elicited by distal stimulation help document conduction block, if associated with clinical weakness and a paucity of voluntarily activated motor unit potentials. The absence of F waves often implies proximal conduction block (15), though a sustained period of immobility can also leads to reversible inexcitability of the anterior horn cells. Dissimilar responses elicited by distal and proximal stimuli might outcome from the use of a submaximal stimulus. Structural abnormalities may render the nerve phase inexcitable despite the usage of ordinarily sufficient stimulation as reported in some circumstances of multifocal motor neuropathy. Such a failure to excite the involved phase maximally could erroneously recommend a conduction block. In these cases, however, stimulation of a more proximal, unaffected nerve phase will evoke a comparatively normal, albeit pathologically dispersed response. The presence of anomalous branches such because the Martin�Gruber anastomosis may result in a confusing pattern of responses, typically mimicking a conduction block. The diagram exhibits stimulation on the calf barely lateral to the midline within the lower third of the leg, and recording with floor electrodes positioned behind the lateral malleolus. Reproduced from Kimura, J, Electrodiagnosis in diseases of nerve and muscle: ideas and follow, 4th edn, copyright (2013), with permission from Oxford University Press. Electromyography reveals little or no evidence of denervation despite poor recruitment of motor unit potentials, which fire quickly to compensate for the blocked fibres. Selective damage of the myelin sheath also can cause pathological temporal dispersion and repetitive discharges, broadening the evoked action potential. The traditional criterion for motor conduction block consists of a reduction in amplitude ratio larger than 50% with lower than 15% increase in length. Central latency = F - M, the place F and M symbolize latencies of the F wave and M response. Conduction velocity = 2D/ (F - M -1), where D signifies the gap from the stimulus level to C7 or T12 spinous course of.
triiodothyroacetic acid (Tiratricol). Viagra Super Active. - What other names is Tiratricol known by?
- Treating thyroid cancer when taken with the drug levothyroxine.Thyroid problems in infants.
- How does Tiratricol work?
- Are there any interactions with medications?
- What is Tiratricol?
- Reducing cellulite.
- Weight loss.
- Improving thyroid function.
- Dosing considerations for Tiratricol.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96530
Buy 50mg viagra super active free shippingA everlasting small space of facial anaesthesia, often lateral to the chin, can hardly ever happen. Interpretation of interictal recordings Focal slowing As within the case of scalp recordings, focal slowing of the background exercise suggests the presence of underlying pathology. Epidural peg electrodes these consist of mushroom-shaped plastic typically positioned in a burr hole to allow epidural recording of brain exercise. Interictal activity recorded with intracranial electrodes ought to be interpreted cautiously. Each patient usually reveals several patterns of epileptiform discharge occurring independently at totally different websites, not essentially on the website of seizure onset, and infrequently including the hemisphere contralateral to seizure onset (3,4). Discharges are normally extra outstanding on the epileptogenic facet, significantly during sleep intervals. However, most sufferers with bilateral impartial interictal temporal discharges have unilateral seizures, normally arising the place spikes are extra frequent (5). Seizure control appears to be better the greater the diploma of lateralization of bilateral unbiased discharges (6,7). Ripples happen over the primary motor cortex and hippocampus, and are thought to be physiological occasions probably concerned in memory consolidation. On the contrary, quick ripples seem to be pathological, predominately occurring at the seizure onset zone each interictally and at seizure onset (10�13). Ictal-like interictal epileptiform discharges As seen in acute electrocorticographic recordings. RaT = proper anterior temporal; RpT = proper posterior temporal; LmT = left mid-temporal. Seizures can start with a run of focal quick exercise, sharp waves, spikes, or gradual waves lasting for a few seconds; such focal modifications are sometimes associated with extra widespread patterns, such as a diffuse attenuation of the background exercise (diffuse electrodecremental event). These sustained ictal adjustments are typically preceded by a single epileptiform discharge, which regularly exhibits a widespread or bilateral distribution, and is associated with a outstanding slow wave. The physiological and medical significance of those widespread modifications at seizure onset is unclear, and their presence is often disregarded in clinical practice. This confirms that the best marker of proximity to the epileptogenic zone is focal quick exercise. The procedure allows further tailoring of the surgical procedure on the time of surgery and, if carried out under native anaesthesia, practical mapping could be carried out. During the procedure beneath native anaesthesia, patients are usually sedated with propofol through the craniotomy, and thereafter, propofol is discontinued and the affected person is allowed to get up. Propofol has pharmacokinetic properties that let quick restoration of the patient on the working table, permitting useful mapping to (A) (C) (B). R = right; L = left; aT = anterior temporal; mT = mid temporal; aLes = anterior lesion; pLes = posterior lesion; asT = anterior subdural temporal; msT = mid subdural temporal; psT = posterior subdural temporal. C) Seizure onset displaying a 2-sec diffuse electrodecremental event preceded by a single epileptiform discharge (arrow) related to a distinguished slow wave. Electrical stimulation throughout functional mapping carries a big risk inducing a seizure. The procedure for intraoperative useful mapping is essentially similar to that described under for subacute recordings. For occasion, it has been described that propofol can suppress or induce spontaneous epileptiform activity during seizure surgery. Inhalational anaesthetics, corresponding to isoflurane or sevofluorane, have been reported to have dose-dependent results in suppressing spike (A) (C) (B). If few epileptiform discharges are seen within the baseline record, spike exercise may be activated, with progressive administration of thiopentane, methohexital, etomidate, or alfentanil. For occasion, through the progressive injection of thiopentane (25 mg each 20 s, as much as 250 mg in adults), an initial activation of a quantity of interictal foci, adopted by burst-suppression patterns at higher doses are expected. It is assumed that epileptogenic cortex is positioned where discharges disappear final and reappear first. Evaluation of interictal discharges It is unclear whether the resection must be guided by the extent, incidence, or amplitude of the epileptiform discharges. Primary discharges are associated with structural lesions and background abnormalities, they usually show sharp parts, (A) (C) (B). R = proper; L = left; F = frontal; T = temporal; A = anterior; L = lateral; M = medial; P = posterior. Excision of all discharging areas has not been thought-about necessary by the Montreal School.
Order 25 mg viagra super active overnight deliveryThese sufferers can reveal very slow ventricular charges at rest or during sleep and infrequently have long pauses. They can also conduct rapidly and develop symptoms attributable to tachycardia during train. In some cases, cardioversion results in a long sinus pause or junctional escape rhythm before the appearance of sinus rhythm. Lack of mechanical atrial contraction poses a excessive danger for thromboembolism in these sufferers. Although the resting heart price could be normal, these patients may be unable to increase their heart rate during train or could have unpredictable fluctuations within the heart price during activity. Some patients can initially experience a normal increase within the coronary heart fee with exercise, which then plateaus or decreases inappropriately. Irregular (and nonreproducible) will increase, and even decreases, in the sinus fee throughout train, can also occur but are uncommon. Sinus arrhythmia is current when the P wave morphology is normal and consistent and the P-P intervals differ by greater than a hundred and twenty milliseconds. The mechanism is unsure but may be related to the effects of the mechanical ventricular systole itself: ventricular contraction increases the blood provide to the sinus node, thereby transiently growing its firing price. Approximately 69% of sufferers with secondary pauses have medical evidence of sinoatrial exit block, and 92% of patients with sinoatrial exit block reveal marked secondary pauses. Sinoatrial exit block of variable period is the first mechanism of prolonged pauses, with a lesser element of melancholy of automaticity. However, secondary pauses could be a normal reflex following hypotension induced by pacing at fast rates or in response to pressure overshoot in the first recovery beat resulting from the prolonged filling time. Normal sinus node perform is assumed when the atrial musculature is depolarized at a standard price and in a normal temporal sequence-so-called regular sinus rhythm. Sinoatrial block is alleged to happen when the entire sinus node electrogram is seen in the absence of a propagated response to the atrium. Additionally, persistence of the sinus node electrogram following carotid sinus therapeutic massage, following induced pauses, or during pauses following overdrive suppression is an important technique for validation. The vary of A1-A 2 intervals at which reset of the sinus pacemaker occurs, resulting in a less than compensatory pause, defines the zone of reset. Data, however, counsel that conduction time into the sinus node is shorter than that out of the sinus node. To remove the results of sinus arrhythmia, a quantity of tests must be performed at every coupling interval. If the A3-A4 interval is longer than the A1-A1 interval, melancholy of sinus node automaticity is recommended. This zone is defined as the range of A1-A2 intervals at which the A2-A3 interval is less than the A1-A1 interval and the A1-A3 interval is lower than twice the A1-A1 interval. In this case, A3 represents delay of A1 exiting the sinus node, which has not been affected. In this case, (A1-A2) + (A2-A3) = A1-A1, and sinus node entrance block is alleged to exist. This zone is defined because the range of A1-A2 intervals at which the A2-A3 interval is less than the A1-A1 interval and (A1-A2) + (A2-A3) is less than A1-A1, and the atrial activation sequence and P wave morphology are equivalent to sinus beats. Instead of atrial untimely stimulation, atrial pacing at a rate slightly quicker (10 beats/min or more) than the sinus price is used as A2. It is assumed that such atrial pacing will depolarize the sinus node without important overdrive suppression. The ensuing intrinsic heart rate represents sinus node fee without autonomic influences. The normal intrinsic heart rate is age-dependent and could be calculated utilizing the next equation: intrinsic coronary heart fee (beats/min) = 118. The regular sinus node responses to atropine are an acceleration of coronary heart price to more than ninety beats/min and a rise over the baseline price by 20% to 50%.
Order 25mg viagra super activeGrades in-between the 2 ends of the spectrum correspond to progressive increment of the delta/theta ratio, decrement of the general voltage and lack of reactivity, and the looks of specific features, such as generalized periodic patterns, or intermittent durations of diffuse suppression, but are much less correct in predicting end result. Recovery has been sporadically reported only when the pattern is current early and transiently (usually for twenty-four h) after resuscitation. Relative contraindications embrace bleeding or high danger of bleeding, similar to post-surgery or post-trauma, but most sufferers are eligible and must remain closely sedated and probably on neuromuscular blockade (to stop breakthrough of shivering), intubated and mechanically ventilated (38). At excessive doses, a burst-suppression sample happens, followed by electrocerebral inactivity. To decrease the risk, the higher restrict of 4mg/kg/h has been advised in the sedation of critically sick patients for longer than forty eight h, and slightly higher infusion rates have been safely used for shorter periods (85). Irrespective of this, propofol is taken into account the best preliminary selection as its major benefits include quick seizure management and quick recovery from anaesthesia, both due to its pharmacokinetic properties. Even within the latest literature, the time period appears to embrace, past the above described pattern, a continuum of any bilateral, synchronous and symmetric sample of temporary, often sharp, complex discharge that repeats itself at quasi-regular intervals, including also triphasic waves as they seem in severe metabolic derangements (97). As coma deepens, scientific responsiveness could diminish or disappear, even to noxious, but electrographic cerebral responses might persist. Demonstrating reactivity is an important task for the physiologist and the electroencephalographer, however requires meticulous testing and cautious interpretation. A normal response is a reproducible change to a pattern that displays larger vigilance, i. Therefore, the recording has to be long enough to allow identification of attainable different patterns that will replicate cyclical changes and stimulations ought to be carefully planned and executed in a timely fashion. Auditory stimuli (calling sufferers by their name for instance) may be more practical when given by a member of the family, similar to a parent or partner (see additionally cognitive potentials below). Stimuli should be intense and extended (for instance nail mattress strain across the proximal fringe of the finger or toe nail sustained for a quantity of seconds) to guarantee temporal summation. Central stimulation (sternal rub or supraorbital pressure) and at last endotracheal suctioning should comply with, particularly when auditory or peripheral tactile stimuli fail to show clear and reproducible responses. Ideally, physiologists ought to work in pairs, or a nurse can stimulate the patient underneath the directions of the physiologist. The sample is ongoing 1 (B) and 4 min (C) after onset and in fact lasted for more than 15 min. Note the amplitude reduction of the plethysmogram that reflects increased sympathetic tone and therefore corroborates higher vigilance. Burst-suppression patterns after 24 h had been also associated with poor neurological outcome, but not inevitably so. The sensitivity and specificity of absent somatosensory evoked potential responses in the course of the first 24 h have been 24 and 100%, respectively (115). Long latency (cognitive) evoked responses rely upon the psychological connotations of the stimuli and are thought to mirror more advanced activation of subcortical areas and thalamus, main cortex and associative areas. Passive paradigms (such as mismatched negativity) use oddball acoustic-are used to assess residual cognition whereas active paradigms could identify acutely aware responses. The major concern is fake positive prediction of a poor outcome which will affect choice about continuation of therapy or withdrawal of life assist. Liaising with the responsible for the affected person intensivist(s) should be actively pursued to plan further diagnostic methods. Bedside medical evaluation of consciousness in the unresponsive sufferers following coma defines short-term management and guides prediction of useful end result, however is particularly difficult (120) and susceptible to errors (121). Evidence of neurotoxicity of ecstasy: sustained results on electroencephalographic activity in polydrug users. Electroencephalography of encephalopathy in patients with endocrine and metabolic issues. Nonconvulsive standing epilepticus in adults: electroclinical variations between correct and comatose forms. Frequency and predictors of nonconvulsive seizures during continuous electroencephalographic monitoring in critically ill youngsters. Frequency and timing of nonconvulsive standing epilepticus in comatose post-cardiac arrest topics handled with hypothermia. Adverse events and their relation to mortality in out-ofhospital cardiac arrest sufferers treated with therapeutic hypothermia. Electroencephalographic monitoring during hypothermia after pediatric cardiac arrest.
Buy viagra super active 100mg without a prescriptionThe report should also be written in a transparent and simple way, avoiding extreme technical terms particularly when addressed to a non-epilepsy specialist. For instance, a spike wave discharge that happens in all scalp electrodes, however has a regional onset could be interpreted, either as focal with fast generalization or as generalized with an incomplete initial phase. Similarly, a spike wave discharge that occupies several adjoining (but not all) scalp electrodes can be interpreted as both (diffusing) focal or (incompletely/abortive) generalized. Record previously unrecognized (or new) seizures/triggers in patients who failed initial remedy. Topographical analysis of the centrotemporal discharges in benign rolandic epilepsy of childhood. American Electroencephalographic Society Guidelines for Standard Electrode Position Nomenclature. Comparison of sphenoidal, foramen ovale and anterior temporal placements for detecting interictal epileptiform discharges in presurgical assessment for temporal lobe epilepsy. Contribute to refinement of the prognosis at various ranges: � Classify the sort of epilepsy. Simultaneous recording of absence seizures with video tape and electroencephalography. Idiopathic generalised epilepsy in adults manifested with phantom absences, generalised tonic-clonic seizures and frequently absence standing. Negative myoclonus induced by cortical electrical stimulation in epileptic sufferers. Juvenile myoclonic epilepsy and idiopathic photosensitive occipital lobe epilepsy: is there overlap Commission on Classification and Terminology of the International League Against Epilepsy. Clinical and electroencephalographic classification of epileptic seizures Epilepsia, 10(Suppl. Interictal temporal delta activity in temporal lobe epilepsy: correlations with pathology and consequence. Familial mesial temporal lobe epilepsy: a benign epilepsy syndrome showing complicated inheritance. Modulation of generalized spike-and-wave discharges during sleep by cyclic alternating sample. Epileptic discharges and phasic sleep phenomena in patients with juvenile myoclonic epilepsy. Sleep deprivation prompts epileptiform discharges independent of the activating results of sleep. Effect of sleep deprivation on spike-wave discharges in idiopathic generalised 34. Assessment with intracranial electrodes can be used in patients the place outcomes from non-invasive checks are contradictory or unrevealing (see Chapter 32 and Box 12. Before implantation of electrodes, there ought to be a hypothesis to explain any non-convergence of proof from totally different checks. This speculation must be testable by the implantation of intracranial electrodes. They offer larger spatial sampling at the price of recording from fewer regions, because the number of implanted electrodes is necessarily limited. For continual recordings, after recovering from electrode implantation, video-telemetry is obtained with implanted intracranial electrodes. Video-telemetry not only goals to localize epileptogenic cortex, but in addition mapping operate in order to keep away from neurological deficits after surgical procedure. Types of intracranial electrodes Intracranial electrodes normally come as bundles of several electrodes assembled in a variety of shapes, every with its own advantages and disadvantages. Subdural electrodes Subdural electrodes are bundles of electrodes assembled as both mats (grids) or strips, which could be placed under the dura in contact with the cortical floor. Mats are two-dimensional arrays of electrodes, whereas strips are arranged as single rows of electrodes. Subdural electrodes are normally made with stainless steel or platinum/iridium embedded in Silastic or Teflon sheets. Each contact typically has 5 mm diameter and contact centres are positioned 1 cm aside, however new models with excessive density grids with smaller diameter electrodes are available. Mats are introduced by way of a craniotomy and can be placed over the cerebral convexity.
|