|
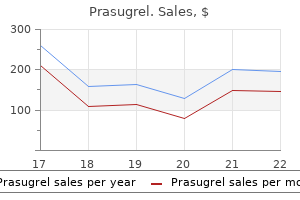
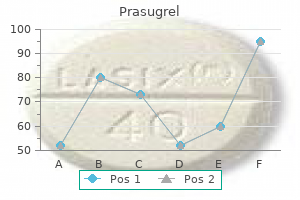
Prasugrel dosages: 10 mg
Prasugrel packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 360 pills

Purchase genuine prasugrel on lineBecause some important anatomic structures could also be obscured throughout airway administration, the anesthesiologist must be familiar with the interrelationship between totally different airway structures. The airway can be divided into the higher airway, which includes the nasal cavity, the oral cavity, the pharynx, and the larynx; and the lower airway, which consists of the tracheobronchial tree. The nasal cavity is split into the right and left nasal passages (or fossae) by the nasal septum, which forms the medial wall of each passage. The septum is shaped by the septal cartilage anteriorly and by two bones posteriorly- he ethmoid (superiorly) and the vomer (inferiorly). Nasal septal deviation is common within the adult population18; subsequently the more patent facet must be decided before passing instrumentation through the nasal passages. The inferior meatus, between the inferior turbinate and the ground of the nasal cavity, is the preferred pathway for passage of nasal airway devices19; improper placement of objects within the nose can end result in avulsion of a turbinate. This fragile structure, if fractured, may find yourself in communication between the nasal and intracranial cavities and a resultant leakage of cerebrospinal fluid. Because the mucosal lining of the nasal cavity is highly vascular, vasoconstrictor ought to be utilized, normally topically, before instrumentation of the nostril to decrease epistaxis. The posterior openings of the nasal passages are the choanae, which lead into the nasopharynx. The onerous palate, shaped by elements of the maxilla and the palatine bone, makes up the anterior two thirds of the roof of the mouth; the taste bud (velum palatinum), a fibromuscular fold of tissue hooked up to the hard palate, types the posterior one third of the roof of the mouth. The posterior wall of the pharynx is made up of the buccopharyngeal fascia, which separates the pharynx from the retropharyngeal space. Improper placement of a gastric or tracheal tube can result in laceration of this fascia and the formation of a retropharyngeal dissection. Along the superior and posterior partitions of the nasopharynx are the adenoid tonsils, which may cause chronic nasal obstruction and, when enlarged, may cause problem passaging airway gadgets. The nasopharynx ends on the soft palate; this area is termed the velopharynx and is a typical web site of airway obstruction in each awake and anesthetized patients. The base of the tongue lies within the anterior aspect of the oropharynx, linked to the epiglottis by the glossoepiglottic folds, which sure paired areas generally recognized as the valleculae (although these are frequently referred to as a single house referred to as the vallecula). The area between the vocal cords is termed the glottis; the portion of the laryngeal cavity above the glottis is named the vestibule, and the portion inferior to the vocal cords is named the subglottis. It consists of 16 to 20 C-shaped cartilaginous rings that open posteriorly and are joined by fibroelastic tissue; the trachealis muscle types the posterior wall of the trachea. No single check has been devised to predict a tough airway accurately one hundred pc of the time; however, an entire analysis of the airway and knowledge of the troublesome airway predictors can alert the anesthesiologist to the potential for problem and permit for applicable planning. The cartilaginous framework of the larynx is made up of nine separate cartilages: the thyroid and cricoid cartilages; the paired arytenoid, corniculate, and cuneiform cartilages; and the epiglottis. The thyroid cartilage is the largest of those cartilages and supports most of the gentle tissues of the larynx. The arytenoid cartilages articulate with the posterior cricoid and are the posterior attachments for the vocal cords. The space inferior to the laryngeal inlet all the method down to the inferior border of the cricoid cartilage is the laryngeal cavity. The ventricular folds (also referred to because the vestibular folds or false vocal cords) are the most superior construction inside the laryngeal cavity. In either case, the affected person interview ought to particularly tackle adjustments in weight, symptomatology, and pathologic situations for the reason that last induction of an anesthetic (if there was one), and attempts must be made at acquiring prior anesthetic records-they could yield useful info regarding airway administration. The presence of pathologic states that improve the danger of a tough airway must be elicited by performing a medical historical past. A centered review of systems can alert the anesthesiologist to other potential components which will predict troublesome airway administration; for example, a historical past of snoring has been shown to be predictive of difficult masks air flow. These embrace apparent facial deformities, neoplasms involving the face or neck, facial burns, a big goiter, a short or thick neck, or a receding mandible. The presence of a beard has been shown to be related to difficult ventilation attributable to the issue in acquiring a mask seal. An interincisor distance of less than 3 cm (or 2 fingerbreadths), as measured from the higher to the lower incisors with maximal mouth opening, can suggest the potential for difficult intubation7; some studies have used 4 or 4.
Diseases - Stratton Parker syndrome
- Blepharonasofacial malformation syndrome
- Daish Hardman Lamont syndrome
- Myalgic encephalomyelitis
- Ornithinemia
- Rhizomelic pseudopolyarthritis
- Anemia, sideroblastic
- Exostoses, multiple, type 3
Buy 10 mg prasugrel otcArbous and coauthors reported a case-control study over 1 12 months within the Netherlands,176 in which they discovered that practice-level unbiased variables associated with a decreased risk for coma and death in 24 hours had been (1) anesthesia tools check performed with a checklist; (2) direct availability of an anesthesiologist by phone, beeper, or walkie-talkie during upkeep anesthesia; (3) no change of anesthesiologist in the course of the case; (4) presence of a full-time nurse anesthetist versus a part-time anesthetist during maintenance anesthesia; and (5) presence of two suppliers versus one particular person throughout emergence. This examine was one of only a few that tried to determine apply characteristics somewhat than particular medication or techniques that have an effect on anesthesia outcomes, and the results are putting, in spite of numerous points with data reporting and matching. The discovering that practitioner traits affect outcomes warrants further follow-up. Attention has recently turned to the influence of handoffs of anesthesia care on patient outcomes. In 2018, Jones and colleagues176a published a retrospective cohort examine evaluating outcomes together with all-cause mortality, hospital readmission, and major postoperative complications in 313,066 sufferers present process major surgery. The examine design was limited by the lack to management for the profession expertise of the alternative anesthesiologist and surgeon as well as by the only use of billing codes to decide exposure to a transition in anesthesia care. Several research have attempted to consider the complication rates and risks associated with numerous care provider models. Bechtoldt,177 as a member of the North Carolina Anesthesia Study Committee, evaluated 900 perioperative deaths that occurred in an estimated 2 million anesthesia procedures performed in North Carolina between 1969 and 1976. A examine by the Stanford Center for Health Care Research178 demonstrated similar outcomes: the investigators reported that dying plus severe morbidity was 11% larger than predicted in patients who obtained their care in a nurse anesthetist�only setting, 3% decrease than predicted for physician-only care, and 20% lower than predicted for an anesthesia care group surroundings. The influence of particular provider sorts could additionally be best specifically conditions: for example, sufferers with significant comorbid illnesses and individuals who maintain perioperative issues may profit from suppliers with particular ability units. One approach to examine such issues is to evaluate the rate of survival after problems. Silber and colleagues7 on the University of Pennsylvania studied the medical data of 5972 surgical sufferers randomly selected from 531 hospitals. They evaluated affected person and hospital traits, together with the number and kind of physicians, board certification status, and ratio of care providers. Improved perioperative survival was considerably related to the presence of an increased number of board-certified anesthesiologists. These findings had been corroborated in followup studies by the identical group,179,181 wherein analysis was again restricted by database traits. They found hospitals without anesthesiologists had results just like these services during which anesthesiologists offered or directed anesthesia care. More lately, work by Needleman and Minnick in contrast obstetric outcomes in facilities with different obstetric anesthesia staffing patterns. Ultimately, as concluded by Smith and associates186 in a evaluation of available revealed studies through 2004 on the affect of anesthesia providers, the relationship of affected person outcomes to the type of anesthesia provider has not yet been conclusively demonstrated. Nurse anesthetists and different nonphysician providers are important to the delivery of anesthesia care within the United States and elsewhere, and determining the optimum scope of practice for such providers stays an ongoing area of academic analysis and political debate. Improving Anesthesia Safety Over the previous a number of many years, major improvements to the security of anesthesia have been initiated. In 1984, Cooper, Kitz, and Pierce hosted a landmark International Symposium on Preventable Anesthesia Mortality and Morbidity in Boston. Approximately 50 anesthesiologists from around the world attended the assembly and, after much debate, established a series of definitions of outcome, morbidity, and mortality (Box 30. The Anesthesia Patient Safety Foundation at 25: a pioneering success in safety, twenty fifth anniversary provokes reflection, anticipation. Overall, these efforts have confused the potential for systems-level enhancements, standardization of care processes, human-factors engineering, and simulation-based coaching to restrict harms attributable to preventable adverse events and errors in crisis administration in the context of anesthesia care. Typically, a practice commonplace implies that a remedy or practice ought to be performed for sufferers with a selected situation. Standards are accredited provided that an evaluation of the possibilities and utilities of the group indicate that the choice to select the treatment or a method would be nearly unanimous. Depending on the affected person, setting, and different elements, tips can and must be tailor-made to match particular person needs. In a similar vein, the World Health Organization has lately placed an emphasis on the potential for a simple preoperative guidelines, modeled on the processes used in different high-risk industries such as aviation, to scale back the charges of adverse events in the perioperative period. Ultimately, such efforts, combined with improved monitoring of antagonistic outcomes by way of massive outcomes databases and those now being assembled by the Multicenter Perioperative Outcomes Group and the Anesthesia Quality Institute, maintain potential to improve the protection of anesthesia care continually on both a national and a world stage. At the identical time, vigilance have to be continued to keep high standards of primary anesthesia care across each hospital- and nonhospital-based settings. Finally, anesthesia providers ought to play a task in systems-based thinking to enhance perioperative care and the short- and long-term outcomes of patients undergoing surgical procedure and anesthesia.
Order genuine prasugrel on lineManagement of hypercalcemia preoperatively should embody (even in pressing or emergency situations) treatment of the underlying trigger, a frequent technique in surgical sufferers with malignancy-associated hypercalcemia. Therapy preoperatively for each malignant and nonmalignant causes of hypercalcemia embrace aggressive volume repletion, with the addition of diuresis provided that quantity overload develops. Intravenous fluid infusion charges of 250 to 500 mL/h preoperatively are generally used to maintain urine output larger than 200 mL/h. In the setting of fluid overload, diuresis with furosemide could be warranted; however, proof for benefit is proscribed and primarily theoreteical. In emergency situations, vigorous growth of intravascular volume normally reduces serum calcium to a protected stage (<14 mg/dL). Phosphate must be given to appropriate hypophosphatemia as a end result of it decreases calcium uptake into bone, will increase calcium excretion, and stimulates breakdown of bone. Hydration, accompanied by electrolyte repletion mainly phosphate, suffices within the management of most hypercalcemic patients. With electrical systole extended, the ventricles might fail to reply to the next electrical impulse from the sinoatrial node, with second-degree heart block ensuing. Because coronary heart failure in sufferers with coexisting coronary heart illness is decreased in severity when calcium and magnesium ion levels are restored to regular, these levels may be normalized preoperatively in a affected person with impaired exercise tolerance or signs of cardiovascular dysfunction; normalization may be achieved intravenously over a 15-minute period if completely essential. Sudden decreases in blood ranges of ionized calcium (as with chelation therapy) may end up in severe hypotension. They could additionally be focal, petit mal, or grand mal in appearance, usually indistinguishable from such seizures within the absence of hypocalcemia. Patients may also have a type of seizure called cerebral tetany, which consists of generalized tetany adopted by tonic spasms. Therapy with commonplace anticonvulsants is ineffective and should even exacerbate these seizures (by an anti�vitamin D effect), calcium should be repleted for therapy. The commonest cause of acquired hypoparathyroidism is surgical procedure of the thyroid or parathyroid glands. Other causes embody autoimmune problems, therapy with iodine-131, hemosiderosis or hemochromatosis, neoplasia, and granulomatous disease. Idiopathic hypoparathyroidism has been divided into three classes: an isolated persistent neonatal type, branchial dysembryogenesis, and autoimmune candidiasis related to a number of endocrine deficiency. Their calcium, phosphate, and magnesium levels must be measured each preoperatively and postoperatively. Patients with symptomatic hypocalcemia could additionally be handled with intravenous calcium gluconate preoperatively. Initially, 10 to 20 mL of 10% calcium gluconate may be given at a price of 5 mL/min. The impact on serum calcium ranges is of short length, but a steady infusion with 10 mL/min of 10% calcium gluconate in 500 mL of answer over a interval of 6 hours helps keep serum calcium at sufficient levels. For extreme signs in emergent settings, 10 mL of 10% calcium chloride could also be given over 10 minutes, adopted by a 10% calcium gluconate infusion. Magnesium and phosphate ranges may also require normalization to normalize cardiovascular and nervous system function. The goal of therapy is to convey the signs beneath control earlier than the surgical process and anesthesia. For patients with persistent hypoparathyroidism, the objective is to keep the serum calcium stage in the lower half of the conventional vary. Changes within the calcium level might alter the period of muscle leisure; thus cautious monitoring and titration of muscle relaxation with a twitch monitor is critical. The intimate involvement of the parathyroid gland with the thyroid gland may find yourself in unintentional hypocalcemia during surgery for diseases of both organ. Because of the affinity of their bones for calcium, this relationship is crucial in sufferers with superior osteitis. Internal redistribution of magnesium, calcium, or each ions could happen (into "hungry bones") after parathyroidectomy and should trigger hypomagnesemia, hypocalcemia, or each. Because the tendency to tetany increases with alkalosis, hyperventilation ought to be prevented.
Generic prasugrel 10 mg onlineThe thumb of the proper hand is pressed on the right lower molars in a caudad path while the index or third finger of the best hand presses on the right upper molars in a cephalad direction. The blade is superior along the bottom of the tongue till the epiglottis is visualized; the tip of the blade is then superior further and positioned in the vallecula. A properly oriented vector of pressure is achieved through the use of the anterior deltoid and triceps, not by radial flexion of the wrist. The epiglottis (1), vocal cords (2), cuneiform cartilage (3), and corniculate cartilage (4) are recognized. The line of sight over the molars is achieved by rotating the pinnacle to the left and shifting the heel of the laryngoscope to the best. The tip of the blade is positioned beneath the epiglottis and a 45-degree lifting force utilized to expose the glottic aperture. The left hand of the laryngoscopist, which holds the laryngoscope handle, is omitted. The laryngoscope is inserted lateral to the tongue and carefully advanced along the paraglossal gutter between the tongue and tonsil. Application of continued reasonable lifting drive to the laryngoscope deal with helps maintain lateral displacement of the tongue and reduces contact with the maxillary teeth. As the laryngoscope is advanced, the epiglottis comes into view and the tip of the laryngoscope is handed posterior to the epiglottis. The path of force applied to the handle is identical as when using the Macintosh blade. Predictors for difficult laryngoscopy that can be identified in the course of the preoperative airway evaluation are listed in Box forty four. Cormack and Lehane developed a grading scale in 1984 to describe laryngoscopic views. This scale has been shown to have a better interobserver reliability than the Cormack-Lehane scoring system and is doubtlessly extra helpful for research studies in direct and indirect laryngoscopy. Unexpected troublesome laryngoscopy: a potential survey in routine common surgery. Nasotracheal Intubation Technique Before nasotracheal intubation, the more patent nostril should be chosen. Hypoxemia, elevated airway pressures, asymmetric chest expansion, and the absence of breath sounds over one lung, usually the left, are indicative of endobronchial intubation; pneumothorax also can produce this picture. Flexible bronchoscopy or chest radiography can be used if the clinical picture is unclear. Because no direct line of sight is needed, visualization of the larynx can occur without tissue distortion; consequently, these strategies can be readily used with topical anesthesia in an awake patient. Indirect laryngoscopy entails the indirect visualization of the glottis by means of optical aids, similar to fiberoptic bundles, video cameras, mirrors, prisms, or lenses. Several forms of intubating oral airways can be found, every with distinctive design variations, and include the Ovassapian, Berman, and Williams airways. A disadvantage of these gadgets is that they place strain on the base of the tongue, probably causing gagging in awake sufferers. This traction could be simply achieved by hand with the help of 4- � 4-inch gauze pads for traction or with Magill forceps. The trachea is well identifiable by the presence of the cartilaginous tracheal rings. Provides confirmation of tube placement, avoiding esophageal and endobronchial intubation. Is well-tolerated in awake patients; leads to less tachycardia and hypertension. While weighing the advantages and downsides, the clinician should decide which strategy is best-suited for the scientific state of affairs. Rigid Indirect Laryngoscopes the primary indirect laryngoscopes for intubation had been based mostly on modifications of the usual direct laryngoscope and used mirrors or prisms to project a picture at an angle from the horizontal, facilitating visualization of the larynx. It can be used for a wide range of purposes, including the identified or predicted troublesome airway, in addition to for awake intubation. A substantial physique of evidence supports the use of these optical stylets in sufferers with limited neck mobility,215 small mouth opening,216 irregular airway anatomy,217 or anticipated tough laryngoscopy.
Gnaphalium italicum (Sandy Everlasting). Prasugrel. - Liver disorders, gall bladder disease, fluid retention, bronchitis, asthma, whooping cough, psoriasis, burns, rheumatism, headache, migraine, allergies, stomach upset, and other conditions.
- What is Sandy Everlasting?
- How does Sandy Everlasting work?
- Dosing considerations for Sandy Everlasting.
- Are there safety concerns?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96511
Buy 10mg prasugrel with amexIf these brokers are used, the neuromuscular transmission must be closely monitored with a nerve stimulator as each resistance and sensitivity to these brokers have been reported. Great care should be taken to keep circulatory stability, together with enough cardiac preload and afterload. Regional anesthesia is employed by some practitioners252 but its use stays controversial because it has been reported to trigger worsening of neurological signs. Although the etiology is unknown, in lots of instances a well timed affiliation with a viral (influenza-like) or bacterial an infection and even lymphomatous disease may be demonstrated. Mild variants can current with ataxia, ophthalmoplegia, or hyporeflexia with out vital appendicular weakness. Fulminant instances can present with severe ascending weakness leading to full tetraplegia, and paralysis of cranial nerves and phrenic and intercostal nerves with facial and respiratory muscle weak point necessitating tracheostomy and ventilatory support. Management is primarily supportive and includes nutritional help, respiratory help, and measures to stop aspiration. Early plasma exchange, usually five exchanges with 5% albumin repletion, could mitigate the course but is contraindicated in setting of hemodynamic instability, marked dysautonomia, and lively bleeding. Particular attention must be made to defend peripheral nerves, particularly the ulnar and peroneal nerves, during positioning of these sufferers 2. Steroids have been implicated in the pathophysiology of the disease and will subsequently be avoided 4. It impacts the lower extremities to a larger extent than higher extremities, and distal muscle groups more severely than the proximal. Conversely, a sensory nerve action potential is commonly regular in important illness myopathy however compound muscle action potentials are diminished and electromyography is according to myopathy. No particular remedies are presently out there, and administration is supportive with aggressive and early rehabilitation. Hereditary motor-sensory neuropathies have been categorised into seven varieties and a number of subtypes based on the age at onset, mode of inheritance, predominately concerned muscle teams, and genotypes. Damage to sensory axons can also result in sensory loss leading to frequent tripping and falls. Major considerations embrace the use of hypnotic agents, muscle relaxants, unstable brokers, and neuraxial methods. The defect is situated on the quick arm of the X chromosome at the Xp21 region, which accommodates the gene for the big protein Dp427, also identified as dystrophin. It also seems that there are "scorching spots" throughout the first 20 exons and in the central area of the gene (exons 45-55) where deletion and duplication are prone to happen. Dystrophin is responsible for maintenance of muscle membrane integrity although it accounts for under roughly zero. Consequently, scientific pseudohypertrophy of the muscle occurs when the useless muscle shells are changed by fibrofatty infiltrates. The initial scientific findings embody a waddling gait, frequent falling, and issue climbing stairs because of proximal muscle weak spot within the pelvic girdle. The basic Gower maneuver describes rising from a sitting to a standing place with the help of both arms. Patients may also show weak spot in the shoulder girdle and trunk erectors that results in thoracolumbar scoliosis. The earlier the onset of disease, the more speedy the illness will take its course. Proximal deep tendon reflexes in the upper extremities and patella may disappear despite the dearth of denervation. Sixty percent of sufferers could have pseudohypertrophy of the calves, and thirty percent will have macroglossia. The mental impairment that can be related to the illness was thought to be associated to limitation of academic opportunities. Cardiac degeneration is due to substitute of myocardium by connective tissue or fat, which leads to dilated cardiomyopathy.
Buy prasugrel 10mg lineBecause of the impaired margin of safety at the neuromuscular junction, a risky anesthetic often offers sufficient muscular paralysis to allow most surgical procedures to be performed without the necessity for a neuromuscular blocking agent. The syndrome is regularly part of a paraneoplastic phenomenon, often combined with small cell lung carcinoma. Improvement of muscle operate with exercise is due to the buildup of presynaptic calcium and subsequent improved release of acetylcholine. Pulmonary perform tests could also be indicated to decide the need for mechanical air flow postoperatively. As a basic rule, patients ought to hold taking their anticholinesterase medicine and be told about the potential of postoperative ventilator assist. Most anesthesiologists used to dose nondepolarizing muscle relaxants in small increments similar to zero. Periodic Paralysis (Hyperkalemic, Hypokalemic, and Normokalemic) the periodic paralyses are a group of problems which are characterized by alterations of operate in voltage-gated ion channels; hence these ailments are generally termed "skeletal muscle channelopathies. In addition, a chilly surroundings, emotional stress, fasting, glucocorticoids, and being pregnant can provoke or worsen the assaults. Mutant channels exhibit sustained sodium currents that result in extended membrane depolarization, which can then cause myotonia followed by membrane desensitization (or inactivation) and will finally end in paralysis. Behavioral modification, similar to avoiding potassium containing meals, strenuous train, fasting, and publicity to chilly are also important. The illness is as a result of of lack of function of one of many two completely different ion channel sorts: CaV1. It has a robust male predominance, and is rather more frequent in patients of oriental descent. Preventive measures similar to maintaining normal body temperature and low serum potassium ranges and avoiding hypoglycemia are useful in limiting such paralysis. General anesthesia, postoperative stress, glucose-containing intravenous solutions, and long-acting neuromuscular blockers are related to postoperative paralytic occasions. Diagnosis rests on acute consciousness of the indicators and signs of this syndrome, of which hyperthermia is a late sign. Specific remedy contains administration of dantrolene to lower muscle Ca2+ ranges, and symptomatic remedy consists of reversal of the acid-base and temperature adjustments. Acknowledgment this text is a consolidation of two chapters in the eighth version, Chapter forty two, Neuromuscular Disorders and different Genetic Disorders and Chapter 43, Malignant Hyperthermia and Muscle-Related Disorders. The editors, publisher, and the returning authors, would like to thank the next authors: Aranya Bagchi, Richa Saxena, and Diptiman Bose for their contributions to the prior edition of this work. Skeletal muscle acutely and unexpectedly increases its sarcoplasmic Ca2+ focus, thereby resulting in increased oxygen consumption and lactate manufacturing, and resulting in higher heat manufacturing, respiratory and metabolic acidosis, muscle rigidity, sympathetic stimulation, and increased cellular permeability. It is a homozygous, single point mutation of RyR1 in swine and a heterozygous dysfunction in humans, in whom there can also be a modification of RyR1 protein perform by interacting buildings, 35 � Neuromuscular Disorders Including Malignant Hyperthermia and Other Genetic Disorders 30. De Novo Reconstitution Reveals the Proteins Required for Skeletal Muscle Voltage-Induced Ca(2+) Release. In Engel A, Franzini-Armstrong C, eds: Myology, third ed, New York: McGrawHill; 20041845. Respiratory Function as a Measure of Muscle Strength in Young Boys with Duchenne Muscular Dystrophy. Glucose-6-phosphatase deficiency (glycogen storage illness I, von Gierke disease). Perioperative administration of the paediatric affected person with coexisting neuromuscular illness. Prevalence of malignant hyperthermia and relationship with anesthetics in Japan: knowledge from the analysis procedure mixture database. Prevention and therapy of malignant hyperthermia in licensed coaching hospitals in Japan: a questionnaire. Presence of two totally different genetic traits in malignant hyperthermia families: implication for genetic evaluation, analysis, and incidence of malignant hyperthermia susceptibility. Prevalence of malignant hyperthermia due to anesthesia in New York State, 2001-2005. Etiological standing and related research of pale, gentle, exudative porcine musculature.
Cheap prasugrel online mastercardAssessment of fluid responsiveness in mechanically ventilated cardiac surgical patients. Fluid responsiveness in spontaneously respiratory sufferers: a review of indexes used in intensive care. Catheterization of the guts in man with use of a flow-directed balloon-tipped catheter. Evaluation of right-heart catheterization within the critically sick patient without acute myocardial infarction. A simple methodology to pass a pulmonary artery flotation catheter rapidly into the pulmonary artery in anaesthetized sufferers. Transthoracic echocardiography assists applicable pulmonary artery catheter placement: an observational study. Complications associated with pulmonary artery catheters: a comprehensive medical evaluate. An up to date report by the American Society of Anesthesiologists Task Force on Pulmonary Artery Catheterization. A prospective analysis of 1400 pulmonary artery catheterizations in sufferers undergoing cardiac surgery. A evaluate of pulmonary artery catheterization in 5,306 consecutive patients undergoing cardiac surgical procedure. Pulmonary artery occlusion stress estimation: how assured are anesthesiologists Failure of a brief academic program to enhance interpretation of pulmonary artery occlusion stress tracings. Ventricular pacing can induce hemodynamically significant mitral valve regurgitation. Transatrial access for left atrial strain monitoring in cardiac surgery sufferers. Frequency of technical problems encountered in the measurement of pulmonary artery wedge pressure. Increased regional myocardial stiffness of the left ventricle throughout pacing-induced angina in man. Silent ischemia throughout coronary occlusion produced by balloon inflation: relation to regional myocardial dysfunction. Do adjustments in pulmonary capillary wedge stress adequately replicate myocardial ischemia throughout anesthesia: a correlative preoperative hemodynamic, electrocardiographic, and transesophageal echocardiographic examine. Right ventricular ischemia recognized by an esophageal electrocardiogram and proper atrial strain tracing. Interpretation of cardiac pathophysiology from stress waveform evaluation: pericardial compressive hemodynamics, half I. Accurate, automated, continuously displayed pulmonary artery pressure measurement. The impact of air flow on the accuracy of pulmonary artery and wedge pressure measurements. Relationship of the pulmonary artery enddiastolic pressure to the left ventricular end-diastolic and mean filling pressures in patients with and with out left ventricular dysfunction. Relationship between pulmonary artery end-diastolic stress and left ventricular filling pressure in patients in shock. Cardiac filling volumes versus pressures for predicting fluid responsiveness after cardiovascular surgical procedure: the position of systolic cardiac function. The Swan-Ganz catheter remains a critically essential component of monitoring in cardiovascular important care. Effectiveness of pulmonary artery catheters in aortic surgery: a randomized trial. Pulmonary-artery versus central venous catheter to information therapy of acute lung harm. Pulmonary artery catheter use is related to lowered mortality in severely injured sufferers: a National Trauma Data Bank evaluation of fifty three,312 patients. Severity of illness and risk of demise associated with pulmonary artery catheter use. Hemodynamic monitoring in the aged undergoing elective colon resection for most cancers. National tendencies in use and outcomes of pulmonary artery catheters among medicare beneficiaries, 1999-2013.
Generic 10 mg prasugrel fast deliveryAlthough a patient who takes steroids on a long-term basis might become hypotensive perioperatively; glucocorticoid or mineralocorticoid deficiency is seldom the cause. Longer duration and better residence steroid dose enhance the likelihood of deficiency. Giving these patients steroid protection equal to one hundred mg of hydrocortisone perioperatively has little risk. The animals were then randomly allocated to teams that obtained subphysiologic (one-tenth of the traditional cortisol production), physiologic, or supraphysiologic (10 instances the traditional cortisol production) doses of cortisol for four days previous abdominal surgical procedure (cholecystectomy). The group given subphysiologic doses of steroid perioperatively had a major enhance in postoperative mortality. Death in the subphysiologic alternative group was related to extreme hypotension associated with a significant decrease in systemic vascular resistance and a lowered left ventricular stroke work index. Filling pressures of the heart were unchanged compared with these in control animals. All these responses are appropriate with the previously documented interplay of glucocorticoids and catecholamines, and thus suggest that glucocorticoids mediate catecholamine-induced will increase in cardiac contractility and maintenance of vascular tone. The investigators used a sensitive measure of wound therapeutic involving accumulation of hydroxyproline. All therapy teams, including the group given supraphysiologic doses of glucocorticoids, had the identical capacity for wound therapeutic. Furthermore, perioperative administration of supraphysiologic doses of corticosteroids produced no opposed metabolic penalties. This study confirmed long-standing intuitive impressions concerning patients who had inadequate adrenal operate because of either underlying illness or administration of exogenous steroids-inadequate substitute of corticosteroids can lead to addisonian crisis and increased mortality, whereas the administration of supraphysiologic doses of steroids for a brief time perioperatively can be safe. Yong and colleagues reviewed the randomized controlled trials for a Cochrane Systemic Review and reported only two trials involving 37 sufferers that met the inclusion standards. The authors concluded that they were unable to help or refute using supplemental perioperative steroids for patients with adrenal insufficiency throughout surgical procedure. Because the danger is low and the benefit is high, physicians should consider offering supplementation for any patient who has obtained steroids within a 12 months. If the plasma cortisol focus is measured throughout acute stress, a worth of greater than 25 g/dL assuredly (and a worth >15 g/dL probably) signifies regular pituitary-adrenal responsiveness. In another test of pituitary-adrenal sufficiency, the baseline plasma cortisol degree is set. A lesser response often indicates pituitary-adrenal insufficiency, presumably requiring perioperative supplementation with steroids. Good correlation exists between the severity and length of the operation and the response of the adrenal gland. In a research of 20 patients during major surgery, the imply maximal concentration of cortisol in plasma was forty seven g/dL (range, 22-75 g/dL). During minor surgical procedure, the imply maximal concentration of cortisol in plasma was 28 g/dL (range, 10-44 g/dL). Although the precise amount required has not been established, we usually intravenously administer the maximum amount of glucocorticoid that the body manufactures in response to maximal stress. Unless infection or another perioperative complication develops, we decrease this dose by roughly 50%/day till the standard residence dose is resumed. For major surgical procedures, we normally give 50 mg every 6 hours to 100 mg every eight hours. Again except a complication develops, this is decreased 50%/day until the usual house dose is resumed. Rare complications of perioperative steroid supplementation embrace aggravation of hypertension, fluid retention, inducement of stress ulcers, and psychiatric disturbances. Two potential issues of short-term perioperative supplementation with glucocorticoids are irregular wound therapeutic and an increased rate of infections. This proof is inconclusive, nevertheless, as a outcome of it pertains to short-term glucocorticoid administration and not to long-term administration of glucocorticoids with increased doses at instances of stress.
Purchase prasugrel 10mg without a prescriptionNote that the polarity of peaks is displayed opposite to standard conference (see text). The instance reveals a recording of posterior tibial somatosensory-evoked potentials. Each tracing is reproduced twice because reproducibility of a waveform helps distinguish sign from artefact. Left and proper posterior tibial nerves are stimulated at 0 and ninety ms, respectively. As a far-field potential, the potential looks similar for right- and left-sided stimulation. The primary cortical responses are recorded from the contralateral hemisphere (labeled P35 and N40). More responses need to be averaged to document far-field potentials (several thousand) than nearfield potentials (50�100). Subcortical responses could arise from many alternative structures depending on the sort of response, including peripheral nerves, spinal wire, brainstem, thalamus, cranial nerves, and others. Subcortical evoked responses additionally may be recorded as far-field potentials from scalp electrodes or, as applicable, from electrodes placed over the spinal column or peripheral nerve. Latency is outlined as the time measured from the application of the stimulus to the onset or peak (depending on convention used) of the response. According to convention, deflections below the baseline are labeled "positive (P)," and deflections above the baseline are labeled "negative (N). The surgical incision and the need for sterility might necessitate nonstandard electrode placements. Recording electrodes may be positioned over the spinal column, peripheral nerve, and (most commonly) innervated muscle. These main corticalevoked responses, which are recordable with most anesthetic methods, outcome from the earliest electric exercise generated by the cortical neurons and are thought to come up from the postcentral sulcus parietal neurons. The longerlatency secondary cortical waves are thought to come up within the association cortex. These responses have a lot larger variability in an awake affected person,42 habituate rapidly on repetitive stimulation,41 and are only poorly reproducible throughout common anesthesia. After synapsing in nucleus Z at the spinomedullary junction, the pathway crosses and tasks onto the ventral posterolateral thalamic nucleus. This point overlies the brachial plexus, and alerts recorded right here assure the clinician that the stimulus is definitely being delivered correctly to the affected person. The subsequent electrode is positioned midline posteriorly over the neck at level of the second cervical vertebra, comparatively close to the dorsal column nuclei. Signals recorded here guarantee proper transmission of the response from the peripheral nervous system into the spinal cord and rostral alongside the spinal cord to the lower medulla. Cervical backbone and scalp recording electrodes are positioned in an identical way as described beforehand, though totally different areas could also be used as required by the surgical incision. More invasive recording methods, similar to epidural electrodes, also may be used intraoperatively. In these instances, attribution of a selected generator to a given wave on the tracing could also be fairly troublesome. After decrease limb stimulation, absolute latencies are increased because of the higher distance the response to stimulation should journey alongside the peripheral sensory nerve and spinal wire. The capacity to establish each of the labeled peaks shown in the tracing from the awake patient is compromised by the anesthetic state and use of various recording electrode places (A�C). The duration of the click is approximately one hundred s, and the stimulus is given normally 10 to 15 occasions per second. Clicks are delivered utilizing completely different "polarities"-that is, the click may trigger preliminary motion of the tympanic membrane away from the transducer (rarefaction) or towards the transducer (condensation). Use of these two completely different methods generally produces very totally different waveforms, amplitudes, and latencies in individual patients, and the tactic that produces the biggest reproducible response is chosen.
|