|
Zebeta dosages: 10 mg, 5 mg
Zebeta packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

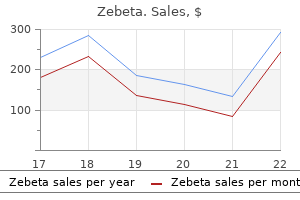
Buy generic zebeta canadaThe range o blood strain in time period in ants during the rst ew hours o li e is 65 to ninety five mm Hg systolic and 30 to 60 mm Hg diastolic, with a median mean blood pressure o 50 to fifty five mm Hg. The blood strain worth will steadily increase from delivery over the transitional interval. This have to be an ongoing course of, as a end result of high-risk sufferers may be recognized on the first prenatal go to, during follow-up prenatal visits, or not until the intrapartum and postpartum periods. R eview o the perinatal historical past is important in figuring out signi cant actors or neonatal well being management. Identification of an at-risk maternal situation is crucial to plan and organize take care of an at-risk neonate. R eview of the perinatal historical past consists of antepartum and intrapartum events (see Chapter 2) and early neonatal events, both in the delivery room and during transition. Initial newborn evaluation consists of the ollowing: � Assessment of gestational age and fetal progress � Newborn classification and neonatal mortality and morbidity threat � Physical and neurologic examination � Assessment of neurobiologic improvement Assessment o Gestational Age and Fetal Growth. Optimal management of the pregnant girl and her fetus is completely dependent on an correct knowledge of the age of the fetus. An assessment o gestational age should be done on all newborns to establish maturity and pattern o etal progress at birth. With the utilization of anthropometetal row ric measurements, including weight, size, and head circumference, along with gestational age, fetal growth standards have been decided for various reference populations from various areas. This variation is expounded to numerous factors, together with sex, race, socioeconomic class, and even altitude. The graphic display o this relationship provides a use ul and simple technique or figuring out the appropriateness o growth with respect to gestational age. Early antenatal ultrasonography appears to have 95% confidence intervals of less than 7 days. This way of figuring out maturity could have already been carried out by the point the new child reaches the nursery. Pediatric strategies o figuring out gestational age are based on physical characteristics and neurologic examination. W ithin 2 hours a ter start, each newborn should have an evaluation o gestational age by bodily characteristics. Neurologic criteria contain the assessment of posture, passive and lively tone, reflexes, and righting response. Gestational age could be assessed most accurately by combining the bodily criteria and the neurologic assessment. The Ballard incorporates physical maturity (six characteristics) and neuromuscular maturity (six criteria) on an equal basis, and includes assessment or extremely premature in ants. The score for the neuromuscular and bodily maturity is added and famous underneath the maturity rating column. This scoring system is simple to per orm, accurate, and extensively utilized in most nurseries. Foot length o appropriate- or-gestational age preterm in ants has been correlated with gestational age (Table 5-4). In early gestation, the pores and skin o the etus is very To use these charts precisely, the examiner must assess the following physical characteristics75,113: Vernix. Vernix is excessive in fat content material and protects the pores and skin from the aqueous amniotic fluid and micro organism. At 36 weeks, the white, cheeselike material begins to lower and disappears by 41 weeks. In a postterm toddler, desquamation might be outstanding at the ankles, wrists, and presumably palms and soles. As gestation progresses, the loss of vernix and subcutaneous tissue causes wrinkling. Note skin turgor, shade, texture, and the prominence o vessels, especially on the abdomen. Note the distribution o lanugo, rst on the ace and anterior trunk and then on the remaining o the body. At term, the hair lies flat on the pinnacle, it feels silky, and single strands are identifiable. An toddler with intrauterine growth restriction and early lack of vernix might have extra sole creases than expected. By 12 hours a ter birth, the pores and skin has dried to a point that sole creases are not a legitimate indicator o gestational age.
Buy zebeta with paypalSelect an uncuffed, uniform-diameter endotracheal tube of the right dimension (Table 4-4). O rotracheal intubation is pre erable to nasotracheal intubation throughout acute resuscitation as a result of it may be per ormed rapidly and without extra gear. Per orm the ollowing steps: � Shorten the chosen endotracheal tube to thirteen cm (or the length appropriate for the fixation methodology used), and put together the laryngoscope, tape, suction, oxygen, bag, and masks. If solely the tongue is seen, advance the blade further till it enters the vallecula or passes under the epiglottis. Pressure may be applied with the little finger of the hand holding the laryngoscope or by an assistant. Complications of intubation embody hypoxia caused by extended intubation attempts or lack of supplemental oxygen; tube malposition; apnea or bradycardia brought on by hypoxia or vagal stimulation; and trauma to the oropharynx, trachea, vocal cords, or esophagus (see Table 4-3). To forestall issues, provide free-flow oxygen during intubation, use mild approach, and limit every intubation attempt to 30 seconds. Follow the sequence of (A) airway, (B) respiration, and (C) circulation in offering resuscitative support. Even i the guts price is less than 60 beats/ min shortly a ter supply, the airway must be cleared and positive-pressure ventilation ought to be given or 30 seconds be ore starting chest compressions. Position: Lower third of sternum47,seventy four Rate: 90 times/ min Depth: One third of the anterior-posterior diameter of the chest Support: Encircling fingers or hand under back � Provide ninety compressions/ min and interpose 30 breaths/ min with a 3:1 ratio o compressions to breaths (120 events/ min). When response to positive-pressure air flow and chest compressions is poor, reevaluate or technical problems and situations inter ering with air flow. Confirm that oxygen is related correctly and that oxygen has been elevated to 100% (see Table 4-3). To ensure a patent airway, place an endotracheal tube and make sure correct position. Ventilate with pressures to increase the chest and breaths interposed between compressions. Evaluate the infant for pneumothorax, diaphragmatic hernia, or hypovolemia (see Delivery R oom Emergencies later in this chapter). Complications of chest compressions embrace liver laceration, rib fractures, and pneumothorax. To prevent problems, examine the position of compressions, maintain contact with the chest in the course of the release portion of the compression cycle, and avoid extreme force during compressions. Perhaps extra necessary during resuscitation is its action as a peripheral vasoconstrictor, directing cardiac output to the central circulation and rising coronary perfusion strain. Providing chest com pressions romthe head o the mattress acilitates em ergency U Cplacem (F V ent. Expansion of plasma and blood quantity may be essential to preserve cardiac output, blood strain, and peripheral perfusion. Normal saline is the pre erred solution or quantity enlargement in a dose o 10 ml/ kg by umbilical venous catheter. Complications of drug administration embrace extravasation with intravascular administration, hepatic harm with low umbilical venous catheters, and unpredictable absorption with endotracheal administration. Epinephrine, administered in excessive doses, will increase the risk for significant hypertension and a hyperadrenergic state, which can end in germinal matrix hemorrhage or myocardial harm. R apid volume enlargement, resulting in acute elevation of systolic blood strain, has been related to intraventricular hemorrhage. Increased cerebral blood circulate and elevated systolic pressures could also be answerable for intraventricular hemorrhage within the presence of a capillary bed insulted by acidosis and hypoxia. The exception to this rule is the infant who has experienced acute perinatal hemorrhage with hypovolemia. These infants ought to have the circulatory fluid volume restored as quickly as possible. Complications of medicine administration can be prevented by choosing the right dose, price, and route of administration and positioning umbilical traces fastidiously. The toddler must be evaluated for opposed effects and response to fluid quantity after each medication/ volume dose. Sodium bicarbonate is now not really helpful or use during resuscitation immediately a ter delivery.
Order zebeta 5 mg without a prescriptionChapter Summary Citric Acid Cycle Mitochondria Function Acetyl (CoA) is completely oxidized to carbon dioxide. During a myocardial infarction, the oxygen supply to an area of the heart is dramatically lowered, forcing the cardiac myocytes to switch to anaerobic metabolism. Succinate dehydrogenase Phosphofructokinase-1 Glucokinase Pyruvate dehydrogenase Lactate dehydrogenase Items 2 and three A 40-year-old African American man is seen within the emergency room for a severe headache. Which of the following enzymes is affected most instantly by the lively metabolite of this drug Which complex associated with electron transport or oxidative phosphorylation is most sensitive to the poisonous byproduct that will accumulate with high doses of nitroprusside A affected person has been uncovered to a toxic compound that will increase the permeability of mitochondrial membranes for protons. Acetyl-CoA, which is produced within the mitochondria, is delivered to these pathways using the citrate shuttle. Oxaloacetate, produced from pyruvate, exits the mitochondrion after conversion to malate. Glycogen synthesis and degradation happen primarily in liver and skeletal muscle, although other tissues, including cardiac muscle and the kidney, retailer smaller quantities. Glycogen is saved in the cytoplasm as either single granules (skeletal muscle) or as clusters of granules (liver). Glycogen granules composed completely of linear chains have the highest density of glucose close to the core. If the chains are branched, the glucose density is highest at the periphery of the granule, permitting more speedy launch of glucose on demand. Glycogen stored within the liver is a supply of glucose mobilized during hypoglycemia. In white (fast-twitch) muscle fibers, the glucose is transformed primarily to lactate, whereas in red (slow-twitch) muscle fibers, the glucose is completely oxidized. Glycogen Metabolism Glycogen Synthase Glycogen synthase varieties the 1,4 glycosidic bond discovered in the linear glucose chains of the granule. Comparison of Glycogen Synthase in Liver and Muscle Glycogen Synthase Activated by Inhibited by Liver Insulin Glucagon Epinephrine Skeletal Muscle Insulin Epinephrine 200 Chapter 14 Glycogen, Gluconeogenesis, and the Hexose Monophosphate Shunt Branching Enzyme (Glycosyl 1,4:1,6 Transferase) 1,four bond Core 1. Transfers the oligoglucose unit and attaches it with an 1,6 bond to create a department. Branching Enzyme Branching enzyme is responsible for introducing 1,6-linked branches into the granule as it grows. Glycogen Phosphorylase Glycogen phosphorylase breaks 1,four glycosidic bonds, releasing glucose 1-phosphate from the periphery of the granule. Glycogen phosphorylase releases glucose 1-P from the periphery of the granule till it encounters the first branch points. Debranching Enzyme 202 Chapter 14 Glycogen, Gluconeogenesis, and the Hexose Monophosphate Shunt Debranching Enzyme (Glucosyl 1,4: 1,4 Transferase and 1,6 Glucosidase) Debranching enzyme deconstructs the branches in glycogen which were uncovered by glycogen phosphorylase. Debranching enzyme: Breaks an 1,4 bond adjacent to the department point and strikes the small oligoglucose chain released to the uncovered finish of the other chain Forms a model new 1,four bond Hydrolyzes the 1,6 bond, releasing the single residue at the branch point as free glucose. Additional symptoms embody: Glycogen deposits in the liver (glucose 6-P stimulates glycogen synthesis, and glycogenolysis is inhibited) Hyperuricemia predisposing to gout. Myophosphorylase Deficiency (McArdle Disease) Myophosphorylase is another name for the muscle glycogen phosphorylase. Symptoms of myophosphorylase deficiency embrace: Exercise intolerance through the preliminary part of high-intensity exercise Muscle cramping Possible myoglobinuria Recovery or "second wind" after 10�15 minutes of exercise A 25-year-old woman had a lifelong historical past of train intolerance that was usually accompanied by episodes of cramping. The episodes have been considerably ameliorated by drinking sucrose-rich delicate drinks immediately before train. The newest episode occurred during her first spin class (stationary bicycling with a resistance load) at her local bicycle store. She initially had excessive weakness in both legs and muscle cramps and later excreted redbrown urine. In subsequent sessions, in addition to the high-sucrose drink, she decreased the load on the bicycle and was better capable of tolerate the initial phase of exercise. After 10�15 minutes, she experienced a "second wind" and was able to continue her train successfully. This woman has myophosphorylase deficiency and is unable to correctly break down glycogen to glucose 6-phosphate in her muscular tissues.
Buy zebeta overnightYorifuji J, Yorifuji T, Nagai S, et al: Craniotabes in normal newborns: the earliest sign of subclinical vitamin D deficiency, J Clin Endocrinol Metab 93:1784, 2008. National Perinatal Association: Multidisciplinary pointers for care of late-preterm infants, 2012. Resource Materials for Parents American Academy of Pediatrics: Parent Education Materials: Care of the uncircumcised penis- truth sheet. Prime amongst these is the lodging to a new thermal setting that represents a definite "chilly challenge. At birth, the body temperature of the newborn infant will approximate or barely exceed that of the mother. Within minutes of birth, nonetheless, core temperature begins to fall precipitously, significantly in infants with delivery weights lower than 1500 g. These in ants have a diminished capacity or metabolic warmth manufacturing, a high sur ace area to volume ratio, and immature epidermal barrier leading to terribly high evaporative warmth losses. This chapter discusses the present information of the physiology and pathophysiology of neonatal thermoregulation and methods used not solely to forestall heat loss but also to handle warmth steadiness. Stephane Tarnier, Chairman of Obstetrics of the University of Paris, first applied the principle of graded incubation (commonly utilized in chick embryos) in creating a covered incubator chamber that has been widely known as the primary try to systematically provide a warmed surroundings for premature infants. Petersburg, R ussia, introduced an incubator described as a double-walled box that circulated warmed water within the interspace. The care of newborns was delegated to Madame Henry, Midwife-in-Chief, who oversaw the building of a pavilion particularly for the care of these weakling newborns. These had been spectacular first steps in attempting to control the delicate heat balance of weak preterm infants. Budin, continued this essential early follow of neonatology, focusing on the home care of those high-risk babies. Alexandre Lion improved the design of incubators and charged spectators a payment to see them in motion, which led to a very popular show on the Berlin Exposition of 1896. An associate of Lion, Martin Couney, introduced the incubator reveals to the United States, the place Dr. Joseph DeLee adopted the know-how and opened an "incubator station" in 1900 on the Chicago Lying-in Hospital. These infants were lined up underneath heaters in incubators, they usually breathed filtered air. At least 8000 infants handed by way of these incubators, and at least 6000 were saved. Servocontrolled radiant warmth in incubators was initially reported by Agate and Silverman in 1963. R adiant energy as the sole source of heat from an overhead panel was described in 1969 by Due and Oliver. As intensive care grew to become extra available, easy accessibility to the infants became increasingly necessary and the open hotter became more readily used. These new beds permit the caregiver to rotate the mattress 360 degrees for simple affected person entry and supply an inbed scale. In latest years, new approaches to thermal care of the new child preterm baby have been extensively studied, including* occlusive wrapping, inserting on heated mattresses, and skin-to-skin * R eferences three, 8, 17, 27, 31, forty one, 49, seventy six. Humans, as homeotherms, preserve a "regular" physique temperature by balancing the amount o warmth lost rom the body with the amount o warmth generated rom within the physique. Our capacity to deal with changing thermal environments improves physically and physiologically with age. Neutral Thermal Environment Physiologic responses to a chilly setting include metabolic reactions that devour substrate and oxygen and end in warmth production. Minimal metabolic activity is feasible within a slim vary of temperatures, so temperatures which are too excessive or too low add stress and improve metabolic rate. Extreme deviations from this vary overwhelm the thermoregulatory mechanisms, resulting in physique temperature imbalances and potentially death. Shaded areas showaverage neutral tem perature vary or healthy in ant w eighing 1 kg (dark) or 2 kg (light) at delivery. O al tem ptim perature most likely approxim to low lim o impartial range as de ned ates er it here. Information from these varied sensors is processed (probably in the posterior hypothalamus), together with common temperature, fee of temperature change, and size of the stimulated area.
Discount zebeta 2.5 mg fast deliveryFractures of the humeral shaft have attribute displacement, which is dictated by the extent of the fracture in relation to the insertion of deltoid. Distal to deltoid insertion, the proximal fragment is abducted by deltoid, while the distal fragment is medialized and shortened by the muscular tissues of the anterior and posterior compartments. Posterior: this allows wonderful repeat the evaluation of neurovascular standing publicity of the distal humerus and is and procure repeat radiographs. Anterolateral: this is an extension of the deltopectoral method described above. In the center and distal thirds of the humerus, the bone is covered by brachioradialis, and the internervous aircraft is between the lateral third (radial nerve) and medial two-thirds (musculocutaneous nerve) of the muscle. Outpatientfollow-up � Mid-shaft humerus fractures are reviewed within the fracture clinic within per week. Patientinstructions � Those sufferers with a U-slab ought to be warned of the potential of plaster complications. Acceptable limits will � clearly rely upon the practical necessities of the patient, however as a rule of thumb, up to 30� of angulation in any course and three cm of shortening are acceptable. Antegrade nailing: this might be most popular in the proximal finish of the nail to be buried to forestall subacromial impingement and cuff segmental fractures (which would otherwise irritation. Shoulder pain from cuff irritation require an extensive exposure and soft is the principal complication of this techtissue dissection) and in pathological fracnique. Surgery is carried out in the beachclose proximity to the axillary nerve, the chair position. A small incision is made just distal screws to the median nerve and bralateral to the acromion. Retrograde nailing: this method aims to cartilage with fluoroscopic assistance. A decrease the insult to the shoulder and sequence of drills and reamers is used to rotator cuff by employing an entry point disprepare the canal earlier than implantation of the tally on the olecranon fossa. After sharp dissection through the subcutaneous tissue, the triceps fascia is introduced into view. Identify the interval between the long and lateral heads of triceps and dissect bluntly between the two. The radial nerve is recognized and protected because it programs with the profundus artery within the spiral groove. Sharp dissection is used to complete the separation of the long and lateral heads distally. Postoperativerestrictions Movement: Free motion of the shoulder and elbow are initiated early. An evolving nerve palsy, or one that arises after surgical procedure, should often be explored. Most radial nerve palsies are lesions in continuity (neurapraxia or axonotmesis; p. The degenerate long head of these could additionally be required to exclude a bony biceps has usually been a source of ache prior harm. Inpatientreferral EmergencyDepartment management Clinicalfeatures � There might be prominence of the biceps belly, � � the affected person should be referred to Orthopaedics for consideration of repair of the damage, as approximately half of the supination power and one-third of elbow flexion power are misplaced. The procedure is carried out There will be tenderness just above the beneath common anaesthesia. A transverse incielbow crease and a tender fullness over the sion is made at the antecubital fossa. Start with the uninjured facet and, tendon end is retrieved and secured with whipwith the elbow flexed, press your fingertip stitches. A drill gap (or holes) is (are) positioned into the medial facet of the antecubital on the tuberosity and the tendon is secured fossa; slide it laterally, feeling for the well- with a suture button system, suture anchor or defined edge of the biceps tendon. The condyles bear the articular surfaces of the humerus, which project distally and anteriorly at 45�, and are barely angled to give round 6� of physiological valgus at the elbow.
Buy cheap zebeta on-lineThe deltoid arises from components (corresponding to the four developmental the scapula and clavicle and inserts into the ossification centres), which are important in deltoid tuberosity. This relationship is essential in avoiding inadvertent neurovascular injury during surgical procedure, because the surgeon ought to always keep lateral to the coracoid course of. The plexus offers off a number of nerves that journey in close approximation to the shoulder skeleton. The axillary nerve is weak to injury in shoulder dislocations or fractures, and in the middle of a deltoidsplitting approach. The anatomical head bears the articular surface of the proximal humerus, which articulates with the glenoid. Lateral to the anatomical head are the greater and lesser tuberosities, that are separated by the bicipital groove. The larger tuberosity is on the lateral aspect of the top, and is the location of insertion of three of the four rotator cuff muscles: supraspinatus, infraspinatus and teres minor. The lesser tuberosity is positioned extra anteriorly and is the positioning of insertion of the remaining rotator cuff muscle, subscapularis. The 4 rotator cuff muscle tissue are principally responsible for sustaining stability of the glenohumeral joint. When the tuberosities fracture, they have an inclination to displace with retraction and defunctioning of their hooked up rotator cuff muscles. In impact, a displaced tuberosity fracture is equivalent to an enormous rotator cuff tear. The anatomical head and the tuberosities make up the surgical head of the humerus. The anterior artery � and in particular its ascending (arcuate) branch, which runs in the bicipital groove � has long been held to be most necessary, although latest research have instructed the posterior artery (which runs with the axillary nerve) is predominant. Additional vascular provide arises from the tendon insertions into the 2 tuberosities and the periosteum, notably on the calcar of the medial neck. Avascular necrosis might comply with a displaced proximal humeral fracture, and affects the anatomical head significantly in displaced four-part fractures where it loses all vascularized attachments. It is effectively cylindrical in shape in the mid-shaft, progressively flattening and flaring out into the supracondylar ridges just above the elbow distally. It crosses the shoulder joint and passes distally to cross Arcuate artery the elbow joint as well, before inserting into the bicipital tuberosity of the radius. It acts to supiAxillary artery nate the forearm and flex the elbow, thus both driving in the corkscrew and pulling out the Posterior circumflex humeral artery cork. Lying deep to biceps is the rather bigger brachialis muscle, which has a broad origin Anterior circumflex over the anterior humerus and inserts into humeral artery the coronoid process of the ulna. The lateral head arises from the dorsal floor of the humerus, lateral and proximal to the groove of the radial nerve. The medial head is deep to the lateral and lengthy heads, and arises distal to the spiral groove, from the posterior side of the humerus and from the medial and lateral intermuscular septa. The triceps muscle is innervated by the radial nerve, which arises from the posterior cord of the brachial plexus and passes by way of the triangular area of the axilla into the posterior aspect of the arm. Here it travels with the profunda brachii artery within the spiral groove, descending and passing medially to laterally till it passes via the lateral intermuscular septum and into the anterior compartment, the place it travels between brachialis and brachioradialis into the forearm. The radial nerve is susceptible to harm at two sites in particular: on the posterior shaft of the humerus and on the elbow. At the elbow, the nerve is at risk throughout an anterior method to the distal humerus. The internervous airplane is inside brachialis whereas dissection lateral to this muscle exposes the radial nerve, which is concealed between brachialis and brachioradialis. In the posterior method to the humerus, dissection through triceps is an anatomical exercise in finding and protecting the nerve. Move Formal testing of shoulder or elbow motion will show painful while offering limited information. Hand and wrist actions to assess neurological operate are enough within the acute setting. A high-energy mechanism of damage, corresponding to a motorized vehicle the most common neurological abnormality in collision or fall from a top, suggests the mid-shaft humeral fractures is a radial nerve possibility of other related injuries and a palsy, occurring in 10% of circumstances.
Buy zebeta 2.5mg cheapFrom a medical viewpoint, cyanosis happens very late in paediatric respiratory misery. A decubitus view could also be helpful in young children, where normally the dependent lung deflates. A Cincinnati (high-kilovoltage filter) view enhances the tracheal air column while deemphasizing the bony cervical backbone to reveal the most important airways. Policy for suspected epiglottitis differs between centres; nonetheless, the result of the x-ray might not influence administration and may be related to vital risk to the kid. Videofluoroscopy is a superb way of demonstrating tracheomalacia and could be mixed with a contrast swallow to exclude vascular compression, tracheoesophageal fistula or aspiration. It may demonstrate diaphragmatic immobility on the aspect of a overseas body airway obstruction. Bronchograms using safe nonionic contrast media are useful for outlining the luminal surface of the decrease airway, demonstrating tracheobronchial stenosis and malacia. Opening pressures of the collapsed bronchi and decrease trachea can additionally be measured, to determine the level of airway support needed. They are helpful in demonstrating vascular anomalies and extrinsic compression of the airway. Virtual endoscopy makes use of radiological knowledge to create pc simulations which could be considered as one would conventional endoscopy. There is also a lack of detail, with airway pathology similar to glottic webs being poorly demonstrated. Airway obstruction that worsens throughout sleep is often a feature of pharyngeal obstruction, corresponding to adenotonsillar obstruction or craniofacial anomaly. Laryngo-tracheal pathology at any stage, together with laryngo-malacia, may, nonetheless, sometimes worsen throughout sleep, thus requiring sleep study investigation. Stridor is usually associated with reflux, and tests for reflux such as double-probe pH studies, distinction studies, milk scan or oesophagoscopy must be thought of. An inadequate analysis will need to be repeated and referral to an experienced centre ought to be made as required, to ensure a single complete and definitive analysis. This is normally thought-about a screening procedure, as the view of the larynx could additionally be suboptimal. Rigid endoscopy of the airway is superior in analyzing the airway for structural abnormalities. Flexible endoscopy could be very helpful in assessing the dynamic airway for vocal twine motion or options of laryngomalacia. A systematic method should be adopted, Endoscopy / Endoscopy technique 563 observing first the nasal cavity followed by the postnasal house, oropharynx, supraglottis and glottis throughout dynamic respiration and phonation. This is solely a diagnostic process, with no opportunity for therapeutic procedures, in distinction to a rigid laryngo-tracheobronchoscopy. Flexible endoscopy underneath sedation in an endoscopy suite is extensively practised by paediatricians and pulmonologists and can be utilized by otolaryngologists as an adjunct to inflexible endoscopy. It allows a radical evaluation to be carried out while the airway is maintained and permits findings to be visually recorded for future reference. It additionally could incorporate therapeutic procedures, including international body removal or the endoscopic administration of airway pathology. It requires an experienced team expert in airway evaluation, including the surgeon, anaesthetist and nursing assistant, who work carefully to ensure an optimal and safe examination. The use of a video is essential to facilitate training and allows the anaesthetist and nurse to comply with the process and standing of the airway on the monitor. It is vital that accurate data are stored in a standardized form within a department. Digital prints present a valid record of static conditions, whilst video clips report dynamic findings. This supplies a useful supply of data for sequential medical comparisons, instructing and medicolegal purposes.
Generic zebeta 5mg overnight deliveryAcetyl-CoA Citrate Malonyl-CoA Malate Oxaloacetate When adipose tissue shops triglyceride arriving from the liver or intestine, glycolysis must also happen in the adipocyte. Which of the next products or intermediates of glycolysis is required for fat storage Glycerol Glucose 6-phosphate Pyruvate Acetyl-CoA Dihydroxyacetone phosphate Items 3 and 4 Abetalipoproteinemia is a genetic dysfunction characterized by malabsorption of dietary lipid, steatorrhea (fatty stools), accumulation of intestinal triglyceride, and hypolipoproteinemia. A deficiency within the manufacturing of which apoprotein would more than likely account for this medical presentation This uncommon purple cell morphology would most likely end result from malabsorption of A. A affected person with a history of recurring attacks of pancreatitis, eruptive xanthomas, and elevated plasma triglyceride levels (2,000 mg/dL) associated with chylomicrons, most probably has a deficiency in A. He is given directions for dietary modifications and a prescription for simvastatin. The scientific findings noted in this patient are most probably caused by poor manufacturing of A. From a Lineweaver-Burk plot, the Km and Vmax of this rate-limiting enzyme were calculated to be four 10-3 M and 8 102 mmol/h, respectively. If the above experiment is repeated in the presence of simvastatin, which of the next values would be obtained A 20-year-old man is taken to the university clinic to decide the cause of recurring hyperlipidemia, proteinuria, and anemia. Fasting blood exams reveal barely elevated concentrations of unesterified cholesterol and phosphatidylcholine. The patient is given a a hundred gram chocolate bar and blood lipid ranges are monitored hourly. Results reveal considerably elevated levels of unesterified cholesterol and phosphatidylcholine for extended durations. A deficiency of which of the following proteins is most probably to be related to the observations in this patient To reform triglycerides from the incoming fatty acids, glycerol 3-P have to be out there. ApoB-48 is required for intestinal absorption of dietary fat within the type of chylomicrons. ApoB-100 formation can additionally be impaired in these sufferers, but this may not clarify the clinical symptoms described. The genetic defect would lead to malabsorption of the three fatty acids listed, but solely linoleate is strictly important in the food regimen. These are the scientific options of lipoprotein lipase deficiency (type I lipoproteinemia). The findings are indicative of heterozygous kind lla familial hypercholesterolemia, an autosomal dominant disease. With a competitive inhibitor, there will be a rise in Km with no change in Vmax. Deficiencies of apoprotein B100 and apoprotein B48 (choices D and C) end in abetalipoproteinemia characterized by decreased blood triglycerides and ldl cholesterol. Free fatty acids are transported by way of the blood in association with serum albumin. Neither erythrocytes nor mind can use fatty acids and so proceed to rely on glucose throughout regular durations of fasting. Short-chain fatty acids (2�4 carbons) and medium-chain fatty acids (6�12 carbons) diffuse freely into mitochondria to be oxidized. Very long-chain fatty acids (>20 carbons) enter peroxisomes by way of an unknown mechanism for oxidation. Fatty acyl- CoA synthetase, on the outer mitochondrial membrane, prompts the fatty acids by attaching CoA. The fatty acyl portion is then transferred onto carnitine by carnitine acyltransferase-1 for transport into the mitochondria.
[newline]Carnitine acyltransferase-1 transfers the fatty acyl group to carnitine (outer mitochondrial membrane). Carnitine acyltransferase-2 transfers the fatty acyl group back to a CoA (mitochondrial matrix). Carnitine acyltransferase-1 is inhibited by malonyl-CoA from fatty acid synthesis and thereby prevents newly synthesized fatty acids from entering the mitochondria. Insulin indirectly inhibits -oxidation by activating acetyl-CoA carboxylase (fatty acid synthesis) and rising the malonyl-CoA focus in the cytoplasm.
|