|
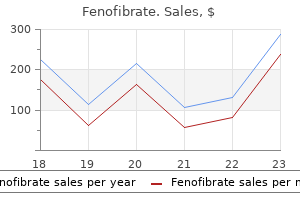
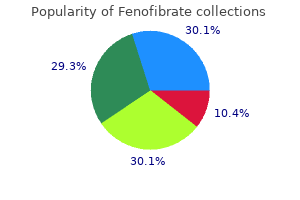
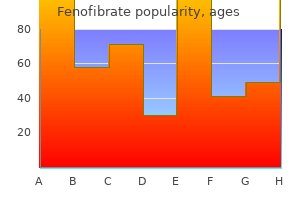
Fenofibrate dosages: 160 mg
Fenofibrate packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Fenofibrate 160mg on-lineThere is critical morbidity associated with open surgery, similar to laryngectomy, and minimally invasive endoscopic approaches have been recommended to scale back problems and morbidity whereas sustaining oncologic efficacy. Radiation and chemotherapy have, sadly, by no means been shown to have efficacy. Until now, mucosal melanoma has been excluded from immunotherapy treatments for the disease; nevertheless at a latest presentation at the European Cancer Congress in 2017, immunotherapy utilizing pembrolizumab was shown to be energetic towards mucosal melanoma tumors, suggesting that in the near future, mucosal melanoma patients must be supplied immunotherapy for the remedy of their disease. Patients with laryngeal melanoma often progress to widespread disseminated illness. In contrast to mucosal melanomas of other sites, laryngeal melanomas appear to have a considerably lower native recurrence price (32%). This could relate to total resectability of laryngeal tumors compared with other sites and to its pathologic stage. Histologically, one can see either mucosal melanocytes or melanin deposition inside basal epithelial cells. A relationship between laryngeal melanosis and primary melanoma has not been established, but a potential association between melanosis and upper aerodigestive tract squamous cell neoplasia is noted in literature. Extraosseus (extramedullary) plasmacytoma seems to be the commonest main hematolymphoid neoplasm of the larynx. The imply age of patients is 59 years (range, 34�78 years) with a male predominance of four:1. In three instances, there was additionally involvement of the adjoining ventricle, trachea, or base of the tongue. On gross examination, the tumor is usually red-brown, lobulated, and smooth or nodular and has a fleshy or rubbery consistency. Immunohistochemistry must be utilized in such instances to demonstrate plasma cell antigens. It has been advised that a proliferation index over 10% and a better grade may predict a extra aggressive course. None of the sufferers died of the disease, with follow-up ranging from three to 25 years (median, 5 years). The low incidence of laryngeal lymphomas has been attributed to a low lymphoid content in the larynx, when in comparison with different areas in the upper aerodigestive tract. Laryngeal lymphomas current clinically in a similar fashion to different tumors of the larynx, with symptoms, such as hoarseness, dyspnea, a international body sensation within the throat, or stridor. Uncommonly, they may current with acute airway obstruction requiring instant surgical intervention. These nonspecific signs may be confused with asthma and might trigger important diagnostic delay. Macroscopically, these tumors are generally polypoid and smooth, without ulceration of the overlying mucosa. Small lymphocytic lymphomas should be distinguished from atypical or reactive lymphoid infiltrates, similar to infectious mononucleosis. Immunophenotypic study shows a mix of B and T cells in reactive lesions, with a polyclonal sample of staining for immunoglobulin mild chains. When low-grade lymphoma is suspected, then molecular research for immunoglobulin heavy chain gene rearrangement could additionally be useful. Those limited to the primary web site or with regional lymphadenopathy could also be managed by radiation therapy. Most laryngeal lymphomas have a great preliminary response to radiation therapy, and the prognosis is mostly favorable. They are included in Group 1 in the lately revised classification of histiocytosis, primarily based on histology, scientific phenotype, molecular alterations, and imaging appearances. Unifocal disease occurs most frequently in older youngsters and young adults, whereas multifocal unisystem disease and multifocal multisystem illness generally affect younger youngsters and infants. Otitis media and/or destructive lesions of the temporal bone will be the preliminary presentation in as many as 60% of instances.
Cheap fenofibrate 160mg on-lineWarthin-Starry silver stain reveals bacterial rods within these histiocytes (inset). The differential diagnoses include atypical mycobacterial an infection, which also appears as a histiocytic infiltrate somewhat than a granulomatous response. Lepromatous leprosy additionally appears as a diffuse histiocytic infiltrate (Virchow cells) and should be dominated out by a Fite-Faraco stain. When a lymphoplasmacytic infiltrate dominates the histology, the analysis of syphilis also needs to be considered. Long-term (3�6 months) parenteral antibiotic remedy, such as with tetracycline, streptomycin, chloramphenicol, or ciprofloxacin (1 g/day) has been reported. The causative agent was named Actinomyces bovis (Actinomyces: strahlenpilz or ray fungus). It was originally thought to be associated with the habit, by both man and cow, of chewing straw. It is classed as a filamentous, gram-positive, nonacid quick anaerobic bacteria, quite than a fungus, as a outcome of it reproduces by fission quite than sporulation (as do excellent fungi) or filamentous budding (as do imperfect fungi) and it accommodates muramic acid in cell walls and absent mitochondria, each features of micro organism. Actinomycetae are part of the normal oral, gastrointestinal, and urogenital tract microbiota. They are of low pathogenicity and need mucosal barrier disruption to trigger illness. If the integrity of the mucosal barrier is compromised, for instance during dental manipulation, trauma, or surgical procedure, entry to the soft tissue and bone is gained. These organisms turn into pathogenic and might initiate a chronic continual inflammatory process, resulting in tissue destruction, formation of abscesses and sinus tracts, which can often be lengthy and communicating with the soft tissues of the again and chest, as properly as fistula, fibrosis and tumor-like plenty. The recognized danger elements include surgical procedure, trauma, diabetes mellitus, alcoholism, and treatment with bisphosphonates, chemotherapy, and irradiation. In the oral cavity, Actinomycetae could be found on mucosal surfaces and in the tonsillar crypts, in gingival sulci, periodontal pockets, and in carious lesions. It is, therefore, generally misdiagnosed as a end result of it could mimic other conditions, such as malignancy and tuberculosis. The pale yellow sulfur granules or grains (originally known as drusen) noticed clinically are microcolonies of bacilli. Microscopically, Actinomyces typically trigger suppurative irritation with colonies of filamentous bacteria, which appear as round or oval basophilic lots with a radiating arrangement of eosinophilic terminal "golf equipment," measuring 1 to 2 mm in diameter. Special stains are helpful to confirm the diagnosis, as Actinomyces stains with silver impregnation methods, and Brown and Brenn staining (gram positive). The distinction between these two filamentous micro organism is essential, as their sensitivities to antibiotics differ: penicillin is the drug of choice for Actinomyces, whereas Nocardia are unresponsive to penicillin and may be treated with sulfa drugs. It has been claimed that culture results in proper diagnosis in only 20% to 40% of instances, whereas the remaining cases are identified by biopsy. Biopsy is considered because the quickest and most delicate means of diagnosis actinomycosis. Actinomycosis is usually handled with prolonged high doses of antibiotics, normally penicillin G. Laryngeal candidiasis is often not seen in immunocompetent hosts, but could also be seen in those with diabetes or sufferers immunosuppressed due to steroid therapy, chemotherapy, or severe chronic illness. Laryngeal candidiasis can clinically present with a mass lesion, mimicking carcinoma. Small, oval, globose yeast cells result in a "spaghetti and meatballs" appearance. If disseminated disease is current, then systemic antifungal therapy (amphotericin B or flucytosine) is indicated. Laryngeal aspergillosis is mostly seen as secondary invasion from the lungs and tracheobronchial tree in immunocompromised hosts. Biopsy samples taken from laryngoscopy show each spores and broad septate hyphae, the majority of which exhibit acute angle branching on histopathological examination. Histopathologically, aspergillosis can show necrotizing, suppurative, granulomatous, or pseudomembranous irritation. The presence of septate hyphae with dichotomous branching is diagnostic for aspergillosis. In some instances, the removing of the vocal cord lesions throughout biopsy provides reduction of signs. Early analysis is essential to stop further dissemination from superficial to the deep type of the disease, where aspergillus can have hematogenous unfold.
Purchase fenofibrate 160 mg with visaCan metastatic lymph node ratio be used as an independent prognostic consider carcinoma tongue Embryologically, the ear is fashioned by the intersection of three developmental embryonic layers "not causally related in growth but linked together solely via the medium of their definitive functioning" (Yntema cited by Van De Water and Rubin1). The external ear, together with the pinna or auricle, external auditory meatus, and canal to the squamous epithelial layer of the tympanum (eardrum), is formed by the ectoderm and mesoderm of the first branchial groove and adjoining first (mandibular) and second (hyoid) branchial arches. The middle ear epithelium, lining the auditory (eustachian) tube, middle ear, and mastoid cavities, is an endodermal derivative of the first pharyngeal pouch, with mesodermal contributions lining the mastoid and epitympanic and hypotympanic cavities. The tympanic membrane is derived from each external and center ear; the external squamous floor is contiguous with that of the exterior auditory canal, and an endodermally derived simple cuboidal, columnar, or flat epithelium lines the center ear. The center ear ossicles and supporting tissues are first and second branchial arch mesenchyme derivatives. The inside ear develops, by mesodermal and neural induction, from the ectodermal otic placode somewhat than from the branchial apparatus. An appreciation of the embryologic origins of the ear is useful in interpreting the origins of tumors, the potential of cells for metaplastic change, and discussions of choristoma and the origin of cholesteatoma. Ross and Sasaki2 review the surgical anatomy of the ear of their dialogue of radical temporal bone surgical procedure for malignant tumors. Analysis of tumors of the ear from main referral centers and community and university hospitals7,eight shows related frequencies of tumor types and placement (Table 12. However, as a result of they occur in the identical age groups and have related clinical presentations, biopsy pattern differentiation between irritation and neoplasia (benign or malignant) is important and infrequently tough. Lesions of the external ear are predominantly lumps and bumps of skin and cartilage origin in elderly individuals. Tumors of the external canal are often not seen and are manifested early by fullness and later by a mass, fluid drainage, or bloody discharge. Hearing loss and ache are symptoms of increasing measurement and invasion, and are scientific manifestations of malignancy. Ulceration and superimposed inflammation can lead to an misguided analysis of irritation, but, aside from otitis in diabetic patients, necrotic inflammatory masses are usually necrotic tumors. Evaluation of the location, dimension, and spread of neoplastic lesions with refined imaging techniques is obligatory. Middle ear lesions current with listening to loss, and, with an otoscope, a mass can be seen behind the normal or bulging eardrum. Chronic otitis media is a sequel of acute otitis media in youngsters, but in adults, continual otitis media is an indication of a systemic illness or neoplasm. Hearing loss happens early in the center of middle ear disease owing to encroachment on the conductive chain of ossicles. An enlarging lesion may cause the drum to bulge into the external canal or destroy the drum. Both neoplasms and an infection unfold from the center ear posteriorly into the mastoid, medially into the jugular fossa, and superiorly by way of the tegmen into the cranial cavity and laterally via the drum. Inner ear tumors are predominantly nerve sheath tumors, meningiomas, and uncommon lipomatous tumors of the eighth cranial nerve involving the internal auditory meatus. Aggressive papillary center ear tumors and endolymphatic sac tumors (associated with von Hippel-Lindau disease), remain rare and controversial lesions. Secondary tumors in the ear/temporal bone are invariably late manifestations of previously recognized tumors, either as metastases or direct native invasion. A and B, Polypoid lesion containing a subcutaneous bar of mature cartilage surrounded by normal pores and skin. Congenital Developmental Anomalies Congenital anomalies of the exterior ear embody the deformed pinna and chronic tracts, pits, cysts, duplications, and anomalous (hamartomatous) glandular tissues in and across the external and middle ear, exemplifying the complexities of embryologic branchial arch derivation. Gustave Davis, the most typical congenital lesion within the Bridgeport Pathology information (see Table 12. Accessory tragus most frequently happens sporadically however can be related to the congenital Goldenhar syndrome (oculoauriculovertebral dysplasia).
Cheap fenofibrate 160mg mastercardCellular atypia and mitotic figures, if current, are usually present in these areas. A, the majority of this tumor (>98%) was composed of sheets of clear cells with barely pleomorphic, eccentrically located nuclei and plentiful clear cytoplasm. A and B, the vast majority of this tumor was composed of sheets of poorly differentiated carcinoma with clear cell options. C and D, Very focally (<1% of tumor), small foci of cells with a microcystic pattern composed of uniform intercalated duct-type cuboidal cells have been seen. A, the vast majority of this tumor was composed of sheets of typical oncocytic cells, with bland nuclei and abundant eosinophilic cytoplasm. B, Focally, the tumor had slightly extra pleomorphic nuclei, cystic change, and, along with areas of eosinophilic cytoplasm, a grayish purple cytoplasmic granularity was famous. Electron microscopy (not shown) confirmed the presence of each numerous mitochondria and zymogen granules. Intercalated ductal- and acinar-type cells normally intermingle to varying degrees. Zymogen granules may be troublesome to show and are normally discovered at least focally after careful searching. Resembling intercalated duct cells of a nonneoplastic salivary gland, ductal cells are generally cuboidal, with restricted amphophilic or eosinophilic cytoplasm and distinct borders. Nuclei, as with acinar cells, are normally uniform and bland, but rarely may demonstrate delicate pleomorphism and atypia. Intercellular microcysts and vacuolated cells might contain mucicarmine-positive material that can occasionally be ample. The end stage of the former is a unilocular cyst, with attenuated and swollen neoplastic cells, accompanied by papillary excrescences. The follicular sample appears to be an exaggerated acinar-microcystic sample in which dilated acini are lined with a flattened epithelium and comprise watery or colloid-like material. The high-grade element lacks acinic cell differentiation and could additionally be very focal or can occupy >95% of the mass. Occasional cases have also included an undifferentiated spindle cell neoplasm1049 and a multiply recurrent tumor exhibiting myoepithelial differentiation. The lack of intercalated, striated, and excretory ducts and normal lobular structure,346 nonetheless, aids in recognizing the neoplastic nature. Attention must also be paid to the distribution of lymphocytes as a outcome of a symmetric and approximately equal distribution of lymphocytes, and tumor cells in a well-circumscribed tumor warrant a diagnosis of the well-differentiated variant, which has a greater prognosis. The follicular variant is a possible mimic of follicular carcinoma of the thyroid. For nearly all of parotid tumors, superficial lobectomy1024,1034,1044 is sufficient, though some have advocated complete parotidectomy. Twentyyear disease-free survival in patients with distant metastases is type of 22%. These tumors had a low mitotic index, and all 12 patients in their sequence remained nicely without evidence of illness with follow-up intervals averaging simply lower than 7 years (range, 19 months to 14 years). Whether this trend will continue will require further cases with longer follow-up. El-Naggar and colleagues1088 noted an association between aneuploidy and poor end result. In our experience, and as reported by others, 1004,1005,1023,1034, 1044,1085 scientific stage at presentation provides essentially the most prognostic information. Accordingly, metastases,1004,1005,1023,1044,1091 large size (>3 cm),1004,1034,1044,1091 deep lobe parotid involvement, 1004,1044 multinodularity,1034 age older than 45 years,1091 and being male,1091 have all been related to poor medical consequence. Occasionally, on reduce surface, cystic areas could also be seen, containing yellow-whitish fluid. The borders of the tumors are normally circumscribed however not encapsulated and broad-front invasion within the salivary gland is commonly current.
Purchase fenofibrate cheapNecrotizing sialometaplasia happens commonly within the hard or soft palate, however can be found within the parotid gland. Unlike dermoid cysts, skin appendages, such as hair follicles and sebaceous glands are absent in keratocystoma. The six instances printed to date with follow-up data have behaved in a totally benign method, with no recurrence after excision or subtotal parotidectomy. It not often could come up in different websites, including the parotid space, lips, breast, and vulva. Six arose in numerous areas of the tongue, three within the flooring of the mouth and one in the nasopharynx and clivus. Mills and coauthors postulated that the microcystic carcinomas doubtless arose from the minor salivary glands or from a multipotential stem cell. Tumor cells usually invade into adjoining soft tissues and skeletal muscle and are composed of bland, minimally atypical, cuboidal cells focally surrounded by an attenuated myoepithelial layer. Nuclei normally have uniformly dispersed chromatin and occasional nucleoli; rare mitoses may be noted. Surgical margins from this tumor must be examined very rigorously, possibly using a number of step sections, as its paucicellular nature and plentiful stroma may lead to missed margin involvement. Most of these differential diagnoses may be eradicated by cautious histologic evaluation. There are quite a few, scattered infiltrating carcinoma cells in a collagenized/desmoplastic stroma (A). Tumor cells are organized in nests, tubules, and epithelial strands, in a markedly desmoplastic stroma (B). Treatment consists of wide surgical excision with adjuvant radiation therapy for optimistic surgical margins. Five of the nine instances handled with surgery had follow-up data, ranging from 10 to 60 months. One tumor was treated with radiation, solely with no change in tumor size at 21 months. Striated Duct Adenoma Striated duct adenomas are unilayered ductal tumors that recapitulate normal striated ducts, that are lined by a single layer, with patchy or absent basal or myoepithelial cells, unlike intercalated or excretory ducts. Prominent cell membranes, harking again to "striations" of normal striated ducts were seen. Only isolated cells in three tumors have been optimistic with p63, which was a pattern similar to the traditional striated ducts. In contrast, striated duct adenoma occurs in main or minor glands, and comprises discrete ducts, with little or no intervening stroma. They share morphologic and immunophenotypic options with normal intercalated ducts. Patients in a latest series of 32 patients with 34 lesions, ranged in age from 19 to eighty years (mean fifty three. The hybrid pattern contains areas of both intercalated duct hyperplasia and intercalated duct adenoma. A and B, the tumor has a fragile capsule and consists of variably sized back-to-back ducts with virtually no stroma. A nodule on the proper is strong, whereas the left two-thirds has a "thyroidized" development sample (A). C, Immunohistochemical stains reveal robust diffuse cytoplasmic positivity with S-100 protein (left), sturdy diffuse cytoplasmic and nuclear staining with cytokeratin 7 (middle,) and really occasional, patchy staining of myoepithelial cells by smooth muscle actin (right). Correlation with the scientific impression, cytodiagnosis, and radiographic imaging can then begin to guide the surgeon alongside remedy pathways. It can be utilized each as a diagnostic take a look at and a screening device to triage patients into different remedy groups, similar to surgical versus medical administration versus following without intervention. It ought to be used to make an intraoperative therapeutic determination: � What is the illness process Is it a primary lymph node course of or is the mass involving the salivary gland parenchyma When contemplating all head and neck neoplasia, the accuracy of frozen-section diagnoses of salivary gland lesions is the most controversial.
Buy fenofibrate without prescriptionClinical and pathologic characterization of mucosa-associated lymphoid tissue lymphoma of the pinnacle and neck. Is clonality equal to malignancy: specifically, is immunoglobulin gene rearrangement diagnostic of malignant lymphoma Targeting Bruton tyrosine kinase with ibrutinib in relapsed/refractory marginal zone lymphoma. Localization of Epstein-Barr viral genomes in angiocentric immunoproliferative lesions. Sequential karyotyping in Burkitt lymphoma reveals a linear clonal evolution with improve in karyotype complexity and a excessive frequency of recurrent secondary aberrations. Impact of oncogene rearrangement patterns on outcomes in patients with double-hit non-Hodgkin lymphoma. Impact of induction regimen and stem cell transplantation on outcomes in double-hit lymphoma: a multicenter retrospective analysis. Plasmablastic lymphomas of the oral cavity: a new entity related to the human immunodeficiency virus an infection. Primary extramedullary plasmacytoma and multiple myeloma: phenotypic variations revealed by immunohistochemical evaluation. Clinical findings in 25 sufferers with sinonasal or nasopharyngeal extramedullary plasmacytoma in a four-decade singlecentre series. Solitary extramedullary plasmacytoma of the pinnacle and neck � long-term consequence analysis of 68 circumstances. Clinicopathological options of myeloid sarcoma: Report of 39 instances and literature evaluation. An immunohistochemical examine of 29 cases using routinely mounted and processed paraffinembedded tissue sections. Detection of prognostically relevant mutations and translocations in myeloid sarcoma by next era sequencing. Blastic plasmacytoid dendritic cell neoplasm: from origin of the cell to targeted therapies. Accordingly, a consideration of pores and skin tumors on this area of the physique should be rather expansive. However, there are some dermatological lesions which may be so uncommon (or unknown) in otorhinolaryngological follow that a dialogue of their attributes shall be understandably omitted. The following chapter addresses these neoplastic pores and skin lesions of the face, neck, and scalp that might be encountered by the pathologist with any regularity no matter. By force of spatial constraint, the morphological features of these proliferations are the principal focus of this evaluation; attendant medical and epidemiological particulars are largely left to the contents of other monographs. These mainly are few in quantity and could be considered underneath the rubric of epidermal nevi. Verrucae and verruca-like nevi reveal common papillomatosis with a "spiky" surface side; acanthosis; regional parakeratosis; and variable levels of nuclear atypia. A notably necessary form of verruciform nevus is the nevus sebaceus, which is found on the scalp and neck. Conversely, hair follicles are either lacking or embryonic in appearance within nevi sebaceus. True verrucae differ from verruciform epidermal nevi in additionally demonstrating multifocal koilocytosis, coarse clumping of keratohyaline cytoplasmic materials, and regional "floor glass" homogenization of nuclear chromatin. These include syringocystadenoma papilliferum, basal cell carcinoma, squamous cell carcinoma, trichoblastoma, trichilemmoma, and apocrine adenocarcinoma. Warty dyskeratoma is one other benign epidermal tumor with a distinctive histological appearance. Keratinous particles might extrude from the latter structure, or the lesion could also be pruritic. Under the microscope, one sees localized acanthosis of the infundibular portion of adjacent hair follicles, with acantholysis of the overlying epithelium and follicular keratin plugs. The acantholytic keratinocytes may show focal cytoplasmic hypereosinophilia and the formation of "corps ronds" as seen in Darier disease (a potentially systemic genodermatosis). Actinic keratosis is a premalignant alteration within the epidermis that clearly is expounded to actinic skin harm.

Purchase fenofibrate 160 mg without a prescriptionInvolvement of the thyroid gland is less widespread, resulting in Riedel thyroiditis, which might cause hypothyroidism and symptoms related to airway obstruction because of enlargement and complete sclerosis of the gland. Early stage of illness could show primarily lymphoplasmacytic infiltration, however fibrosis is extra evident because the disease progresses. A prognosis is highly suggested when the ratio of IgG4-positive to IgGpositive plasma cells is greater than 50% and 30 IgG4-positive cells per high-power area are noted. Lack of monotypic plasma cells and absence of atypia argue against a malignant process. Burkitt lymphoma of endemic (African) type normally impacts the maxilla and mandible. Hodgkin lymphoma, against this, entails lymph nodes in the head and neck, most commonly cervical lymph nodes, and barely occurs in extranodal sites. Extranodal lymphomas, being relatively distinctive in the head and neck, are the main focus. These tumors characterize 15% to 20% of all lymphomas and roughly 50% of extranodal lymphomas of the pinnacle and neck. Affected patients are usually adults over 50 years of age and men are extra regularly affected. The most common presenting signs are airway obstruction, altered listening to, and pain. The tonsils are the most typical site of involvement, representing over 50% of all tumors, followed in frequency by the nasopharynx and base of the tongue. Large noncleaved cells (centroblasts) have vesicular chromatin with two or three nucleoli, often one central and two apposed to the nuclear membrane. Each tumor is classed based on the stage of cell differentiation, cell lineage, postulated cell origin, and the underlying molecular mechanisms. The three major categories are B-cell and T-cell non-Hodgkin lymphoma and Hodgkin lymphoma. The precursor B- and T-cell lymphoblastic lymphomas are further separated from the mature B- and T-cell lymphomas. Malignant lymphomas characterize 5% of all malignant neoplasms of the top and neck area. Approximately 25% to 50% of non-Hodgkin lymphomas within the head and neck region involve extranodal websites ranking second solely to the gastrointestinal tract. Slow to progress but easy to relapse Morphologic Features Immunophenotype Prognostic Factors Reed-Sternberg cells, or Hodgkin cells in a mixed inflammatory background. The lymphoma may have a follicular, follicular and diffuse, or diffuse growth sample. Patients with infectious mononucleosis have tonsillar enlargement that might be pronounced. In most circumstances, the enlargement is bilateral and it is a useful distinguishing characteristic from patients with lymphoma. A, At low power, reactive lymphoid follicles with germinal facilities are surrounded by pale areas. In the pale areas, the neoplastic cell inhabitants is heterogeneous and composed of small lymphocytes, plasmacytoid lymphocytes, plasma cells, and scattered massive cells. Some cells with Russell bodies (eosinophilic intracytoplasmic inclusions of immunoglobulin-related products) are seen. Immunohistochemistry for keratin is extremely helpful for supporting the diagnosis of carcinoma. Indolent T-lymphoblastic proliferation is a really rare nonneoplastic entity that may mimic T-lymphoblastic lymphoma and incessantly entails the tonsils. The importance of indolent T-lymphoblastic proliferation is its recognition as being benign and never requiring remedy. Ocular Adnexal Structures the ocular adnexal structures included on this section are primarily the orbit and conjunctiva. Lymphomas of the eyelid are intently associated to cutaneous lymphomas and the lacrimal gland is extra closely associated to the salivary glands.
Discount fenofibrate 160 mg on lineInflammatory cells, notably mucin-laden macrophages with vacuolated cytoplasm, are current inside the peripheral granulation tissue and pooled mucus. Adjacent intact minor salivary glands, if present, can exhibit infiltration by inflammatory cells and mucin might encompass acini. Rarely, mucoceles could additionally be located so superficially that they simulate subepithelial blistering illness. A, A cystic area is lined focally with residual excretory duct epithelium and granulation tissue. C and D, There is a submucosal pool of extravasated mucin containing a couple of inflammatory cells. Treatment frequently is excision of the mucocele and the encompassing minor salivary glands. Other modes of remedy in the literature embrace cryotherapy, laser ablation, marsupialization, and injection of a sclerosing agent. The mucus retention cyst, also identified as a salivary duct cyst or sialocyst, although intently associated to a mucocele, is much much less frequent. The cause of obstruction is usually not detectable, although sometimes a microlith or inspissated secretion could additionally be seen. Patients are usually older than these affected by mucocele; the typical age was forty five years in one study. In basic unicystic, lesions might hardly ever be multicystic or present ectasia of the adjoining ducts. The epithelial basement membrane of the cyst may appear thickened, and the encircling stroma might seem loose and edematous. Less generally, oncocytoid change and proliferative papillary changes of the epithelium are encountered, and, when current, these cysts have been referred to as reactive oncocytoid cysts and mucopapillary cysts. Sialadenoma papilliferum and inverted ductal papillomas are both related to greater levels of epithelial proliferation than one sometimes finds in a mucus retention cyst, and, in addition, the former is associated with a floor papillary component, whereas in the latter the epithelial proliferation is growing down right into a dilated duct. Etiologies of cystic disease are numerous, and for classification, these may be divided broadly into major and secondary forms. Salivary duct cysts, or sialocysts, within the major salivary glands, often arise within the parotid gland; nonetheless, they could not often be related to ectopic salivary tissue. Although these cysts develop as a consequence of duct obstruction, the cause of obstruction is usually not detectable. Patients most commonly current within the fifth decade of life with a slowly enlarging, painless, mass-like lesion. In general, unilocular lesions not often could additionally be multicystic or show ectasia of the adjoining ducts. Metaplasia of the epithelial lining is widespread; cuboidal or columnar, squamous, mucous (goblet), and clear cells may be seen. B, the submucosal cyst is lined with a skinny uniform cuboidal to columnar epithelium (right). Distinguishing between the primary two entities has already been discussed (see "Mucus Retention Cyst" section). The absence of lymphoid infiltrates, along with medical features, serves to distinguish salivary duct cysts, with or with out proliferative changes, from a Warthin tumor and branchial cleft or lymphoepithelial cysts. Other strategies of therapy are additionally efficient, together with microwave ablation,231 absolute ethanol injection,232 and marsupilization. Ranula (meaning "frog-like" in Latin) is a scientific variant of a mucocele that presents as a large swelling within the flooring of the mouth. Contrasting mucoceles, ranulas symbolize a mucus extravasation phenomenon of main salivary gland origin. Occurring principally from the sublingual gland, they come up from excretory duct disruption. A minority of lesions may prolong through the geniohyoglossus (mylohyoid) muscle and deeper delicate tissue to produce a submental or lateral neck swelling termed plunging or cervical ranula. Clinically, cervical ranulas may simulate bursae, angiomas (cystic hygroma), and other potential midline submental neck lesions, similar to a dermoid cyst, lymphadenopathy, and hematoma. If an associated intraoral ranula is lacking, the diagnostic issue of cervical ranula is significantly elevated. Microscopically, the appearance is similar to mucocele, although foamy histiocytes are probably to be notably prominent in the pseudocyst wall and inflammatory cells could also be inconspicuous.
|