|
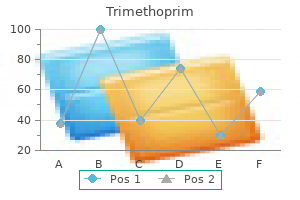
Trimethoprim dosages: 960 mg, 480 mg
Trimethoprim packs: 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Purchase 480mg trimethoprim overnight deliveryBiological implants in sphincter augmentation provide good brief term outcomes after a sphincter repair. Our understanding of the etiology of constipation has improved, resulting in an evolving definition. One generally used definition is based upon bowel frequency of fewer than three stools per week. This definition relies on interviews of factory workers within the United Kingdom that found that 99% of the working population reported frequency of bowel actions between three per day and three per week. The drawback with this definition is that it ignores the symptoms reported by most patients who contemplate themselves constipated. Although physicians and patients usually discuss with constipation as a single disorder, it must be seen as a symptom that means different things to completely different individuals. In 1987, Sandler and Drossman reported on the bowel habits of greater than a thousand adults. Because most constipation becomes a problem only when the affected person complains of it, and because signs of constipation may happen in the absence of any physiologic abnormalities. The standards are expert consensus tips for making the medical diagnosis of the various kinds of functional bowel problems, together with constipation. Must include two or more of the next: Straining 25% of defecations Lumpy or onerous stools 25% of defecations Sensation of incomplete evacuation 25% of defecations Sensation of anorectal obstruction/blockage 25% of defecations Manual maneuvers to facilitate 25% of defecations Less than three defecations per week 2. This pain is related to improvement after a bowel motion, change within the variety of bowel actions, or change in consistency of stools. During repeated makes an attempt to defecate, the affected person should have at least two of the following: a. In these patients, stool frequency could also be regular, however patients really feel constipated and will report problem with defecation, bloating, stomach ache, and hard stools. On testing, sufferers in this group may have elevated rectal compliance, reduced rectal sensation, or both (Ashraf et al. Patients with slow-transit constipation usually have decreased number of high-amplitude propagated contractions of the bowel. This might result from abnormalities of the myenteric plexus, decreased interstitial cells of Cajal which are required to generate smooth muscle electrical sluggish wave, diminished excitatory extrinsic nervous enter, or extrinsic inhibitory activity (He et al. Those with defecation disorders might have normal or barely slowed transit studies however have preferential storage of stool in the rectum. They also have larger defecatory sensation thresholds and may tolerate larger volumes in the rectum. Based on the Cleveland Clinic expertise, outlet-type symptoms of constipation appear to be the predominate subtype seen in patients with other pelvic floor disorders corresponding to pelvic organ prolapse and incontinence. Patients with dyssynergic defecation (the older time period for this is anismus) have paradoxical contraction or failure to chill out the pelvic ground muscular tissues during attempts to defecate. Physical examination could reveal a failure to relax the puborectalis or paradoxical contraction during an tried defecation, they usually have laboratory testing exhibiting evidence of inappropriate contraction or failure of rest of the pelvic floor during makes an attempt to defecate. Structural abnormalities are less frequent but include rectal prolapse and/or intussusception, rectocele, and extreme perineal descent. The premise behind these issues is that the symptoms of constipation result from motor and sensory disturbances, in the end resulting in delayed transit or physiologic disorders of the colon and pelvic floor. Studies of the pathophysiology of disorders of defecation have examined altered anorectal motor and sensory function. The data present proof that practical bowel issues could additionally be more intimately related to the neurologic system than is usually thought. Despite these advances, our information of neuroanatomy and its relationship to practical disorders of the bowel remains in its infancy. Epidemiology Constipation is a commonly encountered problem in medical practice and is predicted to enhance dramatically. Higgins and Johanson (2004), in a scientific evaluation of the epidemiology of constipation in North America, concluded that a conservative estimate of 15% of the North American population, or forty two million individuals in the United States alone, suffer from constipation. Worldwide estimates are comparable, with 12% of individuals reporting self-defined constipation (Wald et al. Higgins and Johanson (2004), in a large systematic evaluation, concluded that the prevalence of constipation stratified by gender confirmed constipation to be approximately 2.
Evening Primrose Oil. Trimethoprim. - Are there safety concerns?
- Is Evening Primrose Oil effective?
- Osteoporosis, when used in combination with calcium and fish oils.
- Attention deficit-hyperactivity disorder (ADHD).
- Hot flashes due to menopause.
- Are there any interactions with medications?
- Symptoms of premenstrual syndrome (PMS).
- Dosing considerations for Evening Primrose Oil.
- Breast pain.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96967
Discount trimethoprim 960 mg with mastercardSacrospinous ligament fixation with transvaginal needle suspension for superior pelvic organ prolapse and stress incontinence. Posthysterectomy vaginal vault prolapse with emphasis on administration by transabdominal sacral colpopexy. Abdominal sacral colpopexy with Mersilene mesh within the retroperitoneal position within the management of posthysterectomy vaginal vault prolapse and enterocele. A comparison of various pelvic reconstruction surgical procedures utilizing mesh for pelvic organ prolapse sufferers. Two-year outcomes after sacrocolpopexy with and with out Burch to forestall stress urinary incontinence. A randomized managed trial evaluating fascia lata and artificial mesh for sacral colpopexy. Massive genital and vaginal vault prolapse treated with abdominal-vaginal sacropexy with use of Marlex mesh: evaluate of the literature. Vaginal length and sexual function after colpopexy for complete uterovaginal eversion. Pelvic promontory fixation of the vaginal vault in sixty-two sufferers with prolapse after hysterectomy. Abdominal colposacropexy and sacrospinous ligament suspension for extreme uterovaginal prolapse: a comparison. Surgical help and suspension of genital prolapse, together with preservation of the uterus, utilizing Gore-Tex gentle tissue patch. Laparoscopic in contrast with robotic sacrocolpopexy for vaginal prolapse: a randomized managed trial. Abdominal sacrocolpopexy: anatomic outcomes and issues with Pelvicol, autologous and synthetic graft materials. A randomized controlled trial evaluating abdominal and vaginal prolapse surgical procedure: effects for urogenital operate. Robot-assisted sacrocolpopexy for pelvic organ prolapse: a systematic review and meta-analysis of comparative research. Symptomatic and anatomic 1-year outcomes after robotic and abdominal sacrocolpopexy. Abdominal-retroperitoneal sacral colpopexy for the correction of vaginal prolapse. Randomized trial of fascia lata and polypropylene mesh for stomach sacrocolpopexy: 5-year follow-up. Abdominal sacral colpopexy in 163 ladies with posthysterectomy vaginal vault prolapse and enterocele. Thumbtack use for management of presacral bleeding, with description of an instrument for thumbtack utility. Outcome of thirty sufferers who underwent restore of posthysterectomy prolapse of the vaginal vault with stomach sacral colpopexy. Effect of surgical volume on outcomes for laparoscopic hysterectomy for benign indications. It represents the third leading cause of hysterectomy for benign illness and is answerable for approximately 70,000 hysterectomies yearly in the United States. Traditionally, operations to treat uterine and uterovaginal prolapse embrace a hysterectomy to provoke the surgery even when no specific uterine illness is present. It stays unknown whether the addition of hysterectomy to prolapse surgical procedure is integral to the effective remedy of this situation and few randomized medical trials of hysterectomy versus no hysterectomy have been accomplished. The surgical remedy of uterovaginal prolapse utilizing uterine-sparing strategies dates back to the late 1800s and has developed from vaginal procedures utilizing native tissue to prepackaged mesh kits and laparoscopic and robotic procedures using polypropylene mesh. Although many of those operations use the same methods and rules as those used to treat vaginal vault prolapse, the outcome data are fewer and direct comparisons are missing. As the interest in uterine conservation amongst sufferers and physicians is rising worldwide, the target of this chapter is to review and summarize the medical literature describing the function of uterine preservation in the course of the surgical administration of uterovaginal prolapse. Chapter Outline Introduction Historical Perspective Considerations for Uterine Preservation Patient Interest Lack of Data Supporting Hysterectomy to Treat Prolapse Role of Hysterectomy in Menopause Timing and Sexual Function Unanticipated Uterine Pathology Vaginal Approach Transvaginal Uterosacral Ligament Suspension/ Plication-Techniques and Outcomes Sacrospinous Ligament Hysteropexy- Techniques and Outcomes Prolapse Mesh Kits Abdominal Approach Open Abdominal Sacrohysteropexy Laparoscopic Ventrosuspension Laparoscopic Uterosacral Ligament Uterine Suspension Laparoscopic Sacrohysteropexy Summary and Future Questions Historical Perspective the origins of the vaginal hysteropexy date back to the late 1800s when methods had been developed to treat uterine retroversion.
Purchase trimethoprim 960mg overnight deliveryDifferences in low-grade persistent irritation and insulin resistance in ladies with previous gestational diabetes mellitus and women with polycystic ovary syndrome. Villitis of unknown aetiology: its incidence and significance in placentae from a British inhabitants. H-2(s) congenic mice are relatively proof against both experimental autoimmune encephalomyelitis and kind I diabetes. Interferon alpha-a potential hyperlink in the pathogenesis of viral-induced sort 1 diabetes and autoimmunity. Obesity and inflammation: epidemiology, threat elements, and markers of irritation. Pregnancy hypertension, placental evidences of low uteroplacental blood move, and spontaneous premature supply. Maternal placental vasculopathy and an infection: two distinct subgroups amongst patients with preterm labor and preterm ruptured membranes. The very low delivery weight infants: maternal problems leading to preterm start, placental lesions and intrauterine progress. Plasma mobile fibronectin as a measure of endothelial involvement in preeclampsia and intrauterine development retardation. Dysfunction of the endothelial nitric oxide signaling pathway in diabetes and hyperglycaemia. Short-term exposure of high glucose concentration induces generation of reactive oxygen species in endothelial cells: implication for the oxidative stress associated with postprandial hyperglycemia. Inhibition of insulin sensitivity by free fatty acids requires activation of a number of serine kinases in 3T3-L1 adipocytes. First trimester placental quantity and three dimensional energy doppler ultrasonography in type I diabetic pregnancies. Adipose tissue irritation contributes to short-term high-fat diet-induced hepatic insulin resistance. Lipoprotein(a) deposition in the uteroplacental mattress and in basal plate uteroplacental arteries: implications for atherosclerosis-associated processes in regular and sophisticated pregnancies. Maternal diabetes mellitus is related to altered deposition of fibrin-type fibrinoid on the villous surface in time period placentae. Clinical associations with a placental diagnosis of delayed villous maturation: a retrospective study. Histomorphometric study of placental villi vascular quantity in toxemia and diabetes. Villous histomorphometry and placental mattress biopsy investigation in type I diabetic pregnancies. The branching pattern of villous capillaries and structural adjustments of placental terminal villi in kind 1 diabetes mellitus. Livebirths with placental hemorrhagic endovasculitis: interlesional relationships and perinatal outcomes. Fetal thrombotic vasculopathy in the placenta: cerebral thrombi and infarcts, coagulopathies, and cerebral palsy. Inferior vena cava thrombosis presenting as non-immune hydrops within the fetus of a lady with diabetes. Peripheral gangrene in a new child toddler associated with renal and adrenal vein thrombosis. The relationship between placental and other perinatal danger factors for neurologic impairment in very low delivery weight children. Placental lesions associated with neurologic impairment and cerebral palsy in very low-birth-weight infants. Perinatal correlates of cerebral palsy and different neurologic impairment among very low delivery weight kids. Placental lesions related to cerebral palsy and neurologic impairment following term start. High glucose-induced apoptosis in human coronary artery endothelial cells entails up-regulation of demise receptors.
Buy trimethoprim 960mg amexPelvic ground muscle coaching for prevention and therapy of urinary and faecal incontinence in antenatal and postnatal ladies. Pelvic floor muscle coaching for prevention and therapy of urinary and fecal incontinence in antenatal and postnatal women: a brief model Cochrane evaluation. The prevalence of anal sphincter defects in faecal incontinence: a potential endosonic examine. Total fecal incontinence � a brand new methodology of gluteus maximus transposition: preliminary outcomes and report of earlier experience with related procedures. Quality of life is markedly improved in patients with fecal incontinence after sacral nerve stimulation. Safety and effectiveness of temperature-controlled radio frequency energy supply to the anal canal (secca procedure) for the therapy of fecal incontinence. Efficacy of dextranomer in stabilised hyaluronic acid for remedy of faecal incontinence: a randomised, shamcontrolled trial. Radiofrequency vitality supply to the anal canal: is it a promising new approach to the treatment of fecal incontinence Sacral nerve stimulation in faecal incontinence: position assertion based on a collective expertise. Anal sphincter defects in fecal incontinence: correlation between endosonography and surgical procedure. Biofeedback and/or sphincter workout routines for the therapy of faecal incontinence in adults. Sacral versus pudendal nerve stimulation for voiding dysfunction: a prospective, single-blinded, randomized, crossover trial. Validation of a questionnaire to assess fecal incontinence and related risk components. Fecal incontinence high quality of life scale: high quality of life instrument for sufferers with fecal incontinence. Posterior Pelvic Floor Sling: A Minimally Invasive Procedure for Correction of Fecal Incontinence. Does the radiofrequency process for fecal incontinence improve high quality of life and incontinence at 1-year follow-up Quality of life and functional outcomes of submucosal injection therapy using dextranomer hyaluronic acid for fecal incontinence. Radio-frequency vitality supply to the anal canal for the remedy of fecal incontinence. Extended two-year outcomes of radio-frequency vitality supply for the therapy of fecal incontinence (the secca procedure). Secca process for the treatment of fecal incontinence: results of five-year follow-up. Injectable silicone biomaterial for fecal incontinence attributable to inner anal sphincter dysfunction is effective. Sacral nerve stimulation for fecal incontinence: outcomes of a 120-patient potential multicenter examine. Stimulated gracilis neosphincter operation: initial expertise, pitfalls, and complications. Infection rates in a big investigational trial of sacral nerve stimulation for fecal incontinence. Most of the studies that stratified by age found constant trends of increasing prevalence of constipation with age, with vital will increase after age 70 years. Interestingly, when Sandler and Drossman (1987) stratified by subtypes of constipation in girls by age, the prevalence of constipation really decreased as they obtained older. Most data suggest similar racial variations in the prevalence of constipation, with a mean prevalence of 1. Outlettype constipation was additionally more prevalent amongst nonwhites in the knowledge from Sandler and Drossman (1987). Because of the high prevalence, constipation consumes substantial well being care assets. Constipation is one the five most typical doctor diagnoses for gastrointestinal disorders.
Buy cheap trimethoprim 480 mg lineA handful of small nonrandomized research report outcomes with failure rates of 0% to 20%. At a mean follow-up of 12 months, 81% had no prolapse symptoms, whereas 79% had no goal proof of recurrence. There were no important differences in preoperative examination, age, body mass index, or parity between profitable and failed circumstances. A smaller prospective study offered related findings in 10 patients with stage 2 symptomatic pelvic organ prolapse (Uccella et al. At a median follow-up of 21 months, 80% of patients were objectively cured, defined as stage 1 prolapse, with solely two sufferers requiring reoperation for recurrent prolapse. All vaginal hysterectomy patients underwent a concomitant vault suspension including a McCall culdoplasty, a sacrospinous ligament suspension, or a laparoscopic uterosacral ligament suspension. The uterine preservation group additionally had fewer reoperations for failures (1 versus 3). The authors are the primary to examine laparoscopic uterine suspension to the traditional standard of hysterectomy with vault suspension. However, their conclusions are limited by the research size, retrospective design, and quick, variable follow-up intervals between the 2 groups. These studies also assist that laparoscopic uterosacral ligament suspension is safe. When in comparison with vaginal hysterectomy with vault suspension, laparoscopic uterosacral ligament suspension resulted in less blood loss (P < zero. Complications reported are few and embrace a uterine artery laceration resulting in a broad ligament hematoma that necessitated laparotomy and transfusion and two cases involving ureteral kinking remedied by a peritoneal ureteral releasing incision. One printed method mimics creation of recent uterosacral ligaments by attaching two 5 mm mersilene tapes from the cervix and bilateral uterosacral ligaments to the sacral promontory, whereas another research describes inserting a suture via the posterior cervix, operating it along the uterosacral ligament, then attaching it to the anterior longitudinal ligament. Other authors describe a method just like sacrocolpopexy, with a polypropylene mesh attached to the cervix and vagina distally and the anterior longitudinal ligament proximally. This may be carried out with a posterior mesh alone or with the addition of two anterior arms passing through the broad ligament to the anterior cervix and vagina. Although the subjective and objective success noticed on this study is encouraging, the study had poor follow-up, a small sample measurement, and lack of a comparability group. Robotic-assisted laparoscopic sacrohysteropexy has been described in a small case collection by Vitobello et al. The cohort study included 50 women and reported that at as a lot as 29 months, girls present process robotic-assisted laparoscopic sacrohysteropexy had important enchancment in high quality of life. Multiple case reports of a single port laparoscopic sacrohysteropexies have been published documenting the feasibility of this method, certainly one of which indicated the affected person had no subjective prolapse at 18 months postoperatively. Although minimally invasive sacrohysteropexy might lead to lower blood loss than an open procedure, it requires superior surgical expertise and may complicate future hysterectomy ought to it become needed. Few data about intraoperative problems exist, although reported postoperative problems embody a small bowel obstruction that required a bowel resection and reanastomosis. A extra critical complication involving an unrecognized rectal harm necessitating a proximal proctectomy, mesh elimination, small bowel resection, left colectomy, and temporary colostomy demonstrates that severe issues can happen with any of those strategies. Summary and Future Questions For the treatment of uterovaginal prolapse, most long-term studies describe vaginal vault suspension with hysterectomy. However, uterine-sparing procedures to treat uterovaginal prolapse have a protracted history and are becoming more popular worldwide. Several strategies with vaginal, open Laparoscopic Sacrohysteropexy Limited data exist on the outcomes and complications of laparoscopic sacrohysteropexy. Unfortunately, the majority of studies describing all approaches to hysteropexy are flawed with bias, quick follow-up, and lack of sufficient control teams. Data support its long-term cure of prolapse, with newer research demonstrating favorable results in comparability to sacrospinous ligament vaginal vault suspension. Quality of life and sexual perform outcomes appear good after sacrospinous hysteropexy.
Order trimethoprim with a mastercardThis is corroborated by direct measurements of cardiac output and progressive decreases in amniotic fluid volume after long-standing redistribution. In addition, elevated ranges of endothelin, arginine, vasopressin, norepinephrine, epinephrine, vasoactive intestinal peptide, and atrial natriuretic peptide lead to enhanced vascular reactivity that may irritate the scientific status and increase the complication price during cordocentesis. Forward blood move within the venous system is decided by cardiac compliance, contractility, and afterload, and is characterized by a triphasic circulate pattern. The sudden enhance in right atrial strain with atrial contraction in late diastole causes a variable quantity of reverse move, producing a second trough after the D wave (a-wave). The magnitude of forward circulate during atrial systole varies significantly in individual veins. Abnormal venous move is characterised by decreasing forward velocities in the course of the a-wave and, to a lesser extent, in the course of the D wave. Multiple venous Doppler indices have been described to characterize this complicated waveform without any clear benefit of particular person indices. If the failure to accommodate preload is progressive, umbilical venous pulsations could also be noticed and are the last word reflection of elevated central venous stress. Abnormal terminal villi and stem arteries result in elevated placental vascular resistance and a proportional lower in the umbilical artery end-diastolic velocity. Associated placental perfusion defects are answerable for impaired feto-maternal fuel and nutrient exchange. Hind limb reflex: Diversion of blood circulate away from the carcass on the expense of the lower physique. Achieved by way of increase in proper ventricular afterload proximal to the umbilical arteries as nicely as elevated blood flow resistance distally. In addition to centralization (see below), descending aortic blood move can additionally be preferentially distributed to the placenta. Centralization: A measurable shift within the relationship between the right and left ventricular afterload, which ends up in redistribution of cardiac output in favor of the left ventricle. This may be passively mediated purely by a rise in the placental blood move resistance and due to this fact right ventricular afterload. Doppler Finding Uterine artery notching Decreased, absent, or reversed umbilical artery end-diastolic velocity Elevation of blood circulate resistance in the thoracic aorta and iliac artery 1. Measured dilation of the ductus venosus with elevated Doppler index accompanied by decreased hepatic artery Doppler index. During perceived hypoxemia and/or redistribution of cardiac output blood flow to the intestine as a nonessential organ in utero is compromised. Splenic artery vasodilatation enhances perfusion of this essential hematopoietic organ possibly facilitating a rise in pink cell mass. There may be a mirrored image of blood move augmentation within the hepatic and splenic arteries, that are the principle branches of this axis. As nonessential organs in fetal life, lung perfusion may be additional compromised by increased vascular resistance in the pulmonary circulation ensuring that a greater proportion of right ventricular output bypasses the lungs to attain the placenta. Redistribution and elevated renal vascular tone will be the mediators of oliguria and oligohydramnios observed with continual and/or progressive hypoxemia. Liver sparing: Preferential arterial blood provide to the fetal liver invoked when elevated diversion of umbilical venous blood by way of the ductus venosus jeopardizes hepatic perfusion. Adrenal sparing: Enhanced adrenal perfusion is triggered as part of the fetal stress response to continual or acute-on-chronic malnutrition. With superior cardiovascular deterioration, brain autoregulation may become abnormal. Probably in affiliation with a lower in cardiac function the interval between systolic and diastolic velocities widens resulting in an increase (thus normalization) of the Doppler index. With the maturation of the vasomotor heart, reticular activating system, central connections, and growing processing of peripheral sensory inputs, the characteristics of the fetal heart fee change with advancing gestation. Variations of the heart price and episodic accelerations coupled to fetal movement every indicate normal functioning of those connections. Under regular circumstances, successive achievement of behavioral milestones progresses from the initiation of gross body movements and fetal respiration to coupling of fetal behavior. Once organized behavioral states are established, the diurnal and responsive cyclicity. Because variations of fetal habits may be due to several components including maturational state, behavioral state, and oxygen tension, statement of a number of variables over a sufficient time period is important to separate physiologic from irregular variation. In the second trimester, amniotic fluid manufacturing is primarily associated to fetal urine manufacturing and due to this fact to renal perfusion.
Syndromes - Numbness in any part of the body
- Fingers or toes turn black or the skin breaks
- Complete blood count (CBC)
- Complete blood count (CBC)
- Death
- Drugs used to treat schizophrenia or psychosis
Purchase trimethoprim with visaFew stories have addressed the results of the newer era sulfonylureas (glibenclamide, glipizide, and gliclazide) or repaglinide on the fetus. Coetzee and Jackson have reported on the use of glibenclamide (combined with metformin) during being pregnant each for gestational diabetes and type 2 diabetes. They managed over 600 women between 1974 and 1983, and located decreased perinatal morbidity compared with the control group and no instances of great neonatal hypoglycemia. This is a reassuring finding concerning the safety of glibenclamide in gestational diabetes. There are several possible mechanisms for the absence of glibenclamide within the umbilical cord blood of the infants whose mothers had taken the drug. Data from a number of research recommend that drug transporters could play an essential function. Glibenclamide has been shown to be a substrate for P-glycoprotein and P-glycoprotein induction by rifampicin77 has been proposed as the reason for the decreased half-life and space under the plasma concentration-time curve of glibenclamide with extended administration of rifampicin. P-glycoprotein has been found in the human placenta78 and its exercise as an extruding drug pump has been proposed to influence the passage of several drugs. Other reasons for the poor placental transfer of glibenclamide could also be its very excessive protein binding (99. An necessary concern with the utilization of glibenclamide is the potential for drug interactions. As talked about earlier, P-glyocprotein inhibition produces pharmacokinetic adjustments in disposition. Glibenclamide has been shown to each inhibit and be a substrate of P-glycoprotein81,82 which could probably lead to many alternative drug interactions in both the mom and the fetus. The single cotyledon perfusion study has proved to be a priceless tool in the preclinical evaluation of medication that could be of use in being pregnant. Still, higher prognostic strategies and algorithms are wanted to be able to predict with larger confidence which drugs may not cross the placenta. The use of oral brokers in women with kind 2 diabetes could be of nice benefit, since these sufferers are probably to be of lower socioeconomic status and have a tendency to belong to immigrant populations in developed countries. The excessive cost of insulin and syringes might preclude using insulin in many populations, especially these where kind 2 diabetes has a high incidence (native populations, immigrants and in developing countries). Given the chance to use oral agents, compliance may enhance, leading to better glycemic management and lower perinatal morbidity. There appears to be a widespread notion that finding out medicine in pregnant ladies carries the unacceptable threat of unpredictable and deleterious adverse effects in the fetus. Systematic clinical research of appropriate drugs must be performed, with the dangers being fastidiously assessed and measured as a substitute of officially denying the treatment to a population and then unofficially using the drug "as needed. The mostly pharmaceuticals fall into the therapeutic classes of antibiotics, analgesics, antiemetics, and narcotics. Clinicians would typically shudder on the thought of conducting a scientific study of an oral hypoglycemic drug throughout being pregnant, but still would use it in "particular circumstances," as proven by a wealth of case stories and sequence. This paradox leads to a waste of very useful knowledge and to a distorted notion of risks. This in turn leads to misuse of important drugs, either denying them to a inhabitants that could acquire great profit from them, or using them in a probably harmful means, exposing that very same population to extreme and infrequently unperceived dangers. In order to be ready to begin clinical research of a sure drug, each effort have to be made to collect meaningful pharmacokinetic and pharmacodynamic knowledge from previous use of the drug in different populations and in animals, and derive predictions from these parameters as nicely as precautions regarding antagonistic results observed. More common use of in vitro testing of placental transfer of medication ought to be included as a routine stage of drug growth. Glycemic control, nevertheless, has also been implicated as an etiological issue for congenital malformation in ladies with diabetes. Poor glycemic control is known to be related to an increased number of malformations in people with insulin-dependent diabetes in a dose-dependent style. The key phrases being pregnant, diabetes; diabetes mellitus; non-insulin dependent; and polycystic ovary syndrome have been used to search for studies on the disease. As nicely, the keywords abnormalities; drug-induced, pregnancy issues; neonatal diseases and abnormalities; infant mortality; and hypoglycemia were used to seek for research on the outcome. Other potential confounding variables abstracted were maternal age, weight, race, comorbidities.
Order trimethoprim online nowIn situations where the cul-de-sac may be very deep and broad, internal McCall-type sutures can be positioned, plicating the distal remnants of the uterosacral ligaments across the midline. Cystoscopy after intravenous injection of indigo carmine is recommended to doc bilateral ureteral patency. The sacrospinous ligaments lengthen from the ischial spines on both sides to the lower portion of the sacrum and coccyx. A, probably the most outstanding portion of the prolapsed vaginal vault is grasped with Allis clamps. The retractor lifts the sponges up out of the decrease pelvis, thus completely exposing the cul-de-sac. When appropriate downward traction is applied on the uterosacral ligaments with an Allis clamp, the uterosacral ligaments are easily palpated bilaterally. D, Delayed absorbable sutures are passed through the uppermost portion of the uterosacral ligaments on all sides and are individually tagged. E, Each finish of the previously handed sutures is brought out by way of the posterior peritoneum and the posterior vaginal wall. A free needle is used to cross each ends of those delayed absorbable sutures by way of the full thickness of the vaginal wall. F, the anterior colporrhaphy is begun by initiating a dissection between the prolapsed bladder and the anterior vaginal wall. The fibromuscular coccygeus is attached directly to the underlying sacrotuberous ligament. Also, an plentiful vascular provide that features inferior gluteal vessels and hypogastric venous plexus lies superiorly. The sacrospinous ligament colpopexy is finished for average to extreme apical prolapse after hysterectomy; it may also be done with simultaneous vaginal hysterectomy and even as a hysteropexy (see Chapter 26). H, the vagina has been appropriately trimmed and closed with interrupted or steady delayed absorbable sutures. After closing the vagina, the delayed absorbable sutures that had been previously brought out by way of the full thickness of the posterior vaginal wall are tied, thereby elevating the prolapsed vaginal vault excessive up into the hollow of the sacrum. A, the uterosacral ligament at about the stage of the ischial backbone is grasped with an Allis clamp. B, Three sutures are positioned via the ipsilateral uterosacral ligament after which by way of the vaginal apex. This operation normally requires simultaneous correction of the anterior and posterior vaginal partitions and an enterocele repair. Placing the prolapsed vaginal apex to the sacrospinous ligament to see whether the vagina is long sufficient to full the repair and whether the anterior and posterior vaginal wall prolapse disappear helps to decide whether cystocele and rectocele repairs are wanted. If the uterus is current, a vaginal hysterectomy is done and the peritoneum is closed, as beforehand described. Sacrospinous cervicopexy or hysteropexy may be accomplished utilizing related technique, if desired (see Chapter 26). The apex of the vagina is grasped with two Allis clamps, and downward traction is used to decide the extent of the vaginal prolapse and related vaginal help defects. The vaginal apex then is decreased to the sacrospinous ligament meant to be used. In the posterior method a midline posterior vaginal wall incision is made just short of the apex of the vagina, leaving a small vaginal bridge approximately 3 or 4 cm broad. The perirectal house or the area alongside the peritoneum near the apex then is entered by breaking by way of the fibroareolar tissue just lateral to the enterocele sac at the degree of the ischial spine. This can often be achieved with blunt dissection after mobilizing the rectum medially. At instances, however, using gauze on the index finger or a tonsil clamp is necessary to break into this area. The surgeon should take nice care to be certain that the rectum is adequately retracted medially. At this time, we suggest performing a rectal examination to ensure that no inadvertent rectal injury has occurred. Several strategies are used for the precise passage of sutures through the ligament.
Buy trimethoprim without a prescriptionExercise results in useful alterations in body composition and biochemical, physiological, and morphological changes in skeletal muscular tissues. Exercise in an overweight lady leads to weight loss and the share of type 1 muscle fibers will increase, resulting in elevated muscle oxidative capacity. In addition to these components, train could relieve stress, scale back anxiety, and depression, and improve self-confidence and, in doing so, limit "emotional eating" that contributes to weight gain and insulin resistance. Increased bodily activity typically leads to enhancements in self-image and other components that, in turn, support healthy life style. After an exercise session, glucose tolerance is improved for variable durations depending on the mass of the muscle activated, duration, depth, and insulin response. Essential to this course of that results in improved insulin sensitivity and glucose uptake is the activation of notably giant muscles such as the quadriceps. There has lengthy been concern that train throughout being pregnant may increase the chance of preterm delivery, fetal growth restriction, or fetal misery as a end result of a decrease within the uterine blood move throughout train that could affect the fetus and end in an abnormal fetal heart fee and other physiologic responses that might be dangerous to the fetus and even end in fetal demise. In the nonpregnant woman, target coronary heart charges have been incessantly used to prescribe train. In regard to prescribing exercise intensity, nonetheless, it should be acknowledged that in being pregnant maximal maternal coronary heart price reserve decreases and resting coronary heart price increases. There are few studies in pregnancy combining food regimen and train; however, proof is emerging that each exercise and weight restrictions are safe interventions in obese and obese pregnant women. A triad of pregravid weight problems, excessive gestational weight achieve, and diabetes in being pregnant are often discovered in combination. Each of these factors independently will increase the chance of fetal overgrowth and, in turn, childhood obesity. In our expertise, minimally to no weight acquire in overweight girls has no deleterious impression on the fetus and is beneficial to the mother in regard to her long-term three. Hypoglycemia may also end result when a pregnant lady workouts and her glucose stage is depressed secondary to fasting or medicine. The risk of hypoglycemia is best in early being pregnant, previous to the autumn in insulin-mediated glucose disposal that happens over the course of the second and third trimesters. Over the previous 30 years, our laboratory has carried out research examining the impact of being pregnant on maternal and fetal responses to exercise, on the regulation of glucose homeostasis by glucagon, insulin, and catecholamines and other. After 45 minutes, glucose concentration declined additional, suggesting that at this point the potential threat of hypoglycemia with moderate-intensity continuous train could rise. Preexisting and pregnancyinduced low-back ache and joint pain are additionally common issues. Pregnant women with these limitations could additionally be extra tolerant of nonweight-bearing exercise. Many of the person trials which have investigated the impression of bodily exercise on gestational weight gain have been restricted by their small size and poor participant compliance. Recognition of those limitations have prompted a 2011 meta-analysis of 12 bodily exercise intervention trials that collectively enrolled over a thousand ladies. The analysis uncovered a modest however statistically vital discount in gestational weight achieve amongst those uncovered to various bodily activity interventions. That meta-analysis included five prospective cohort, two retrospective case-control, and two cross-sectional studies. This means that an exercise program, although useful to all is more practical in preventing gestational diabetes in overweight or obese ladies, rather than in regular weight girls. The other five trials have been initiated earlier in pregnancy but the majority if not all the varied interventions were carried out within the second and third trimesters, and the facility of the trials was restricted by their small measurement, ranging from a total of 41 to 142 individuals. Only one of the research included on this 2013 meta-analysis restricted enrollment to overweight pregnant ladies. The intervention concerned twice weekly 60-minute aerobic and strength train classes that started around 15 weeks of gestation. That danger is essentially as a outcome of decreased hypoglycemic awareness and counter-regulatory diversifications which may be altered by pregnancy-related augmentation of catecholamine and glucagon responses. The widespread use of insulin pump units and growing reputation of steady glucose sensors might facilitate and enhance the safety of exercise for pregnant women with type 1 diabetes. Nonetheless, we recommend that these patients have interaction in reasonable exercise limited to 30 minutes per session. Although the risk of hypoglycemia with gestational and kind 2 diabetes is considerably decrease, these girls typically enter pregnancy obese and deconditioned and because of this are at higher threat of exercise-related musculoskeletal injuries.
Purchase trimethoprim 960mg without a prescriptionSurgical handle ment of meshrelated issues after prior pelvic ground reconstructive surgical procedure with mesh. Suprapubic telescopy: extraperitoneal intra operative approach to demonstrate ureteral patency. However, problems from each traditional and mesh-augmented prolapse repairs and from placement of artificial slings occur; this chapter discusses these various complications and how best to handle them. Population-based research report an 11% to 19% lifetime threat of ladies undergoing surgery for certainly one of these conditions, with a recurrence of symptoms frequent in both teams. Of the women who bear a pelvic ground repair, 6% to 29% have additional surgical procedure for recurrent prolapse, stress incontinence, or related problems (Olsen et al. The success initially noticed with the utilization of surgical mesh in general surgical procedure mixed with the perceived high failure rates for traditional native tissue suture repairs for prolapse initially led gynecologic surgeons to implement surgical approaches that use prosthetic supplies. Medical system manufacturers have estimated that, in 2006 and 2007, approximately 30% of pelvic organ prolapse restore procedures and 80% of anti-incontinence procedures used reconstructive prosthetic materials. However, considerations raised across the security of transvaginal mesh and artificial slings are because of a wide range of concerns related to mesh erosion, ache, vaginal constriction, and other issues. Although similar types of problems have occurred with native tissue sutured repairs, the notion is that graftrelated issues have been more severe and difficult to handle. Stanley Birnbaum described a novel method for treatment of vaginal prolapse in which fixation of the vaginal vault with a Teflon mesh bridge anchored the vagina to the hole of the sacrum. A follow-up article 6 years later famous that 20 of 21 sufferers handled with this system maintained good support and vaginal operate. Over the final 15 years there has been a significant refinement and improvement in surgical mesh supplies (see also Chapter 28). Early on, there were problems with some surgical meshes that had been associated with increased erosion and an infection charges. In most circumstances, these meshes had been microporous multi-filament supplies, which normally require complete explantation for symptom improvement (Occhino et al. They can further be divided by weight (heavy, mid- or light-weight) (Sanders and Kingsnorth 2012; Amid 1997). Synthetic mesh utilized for prolapse repairs may be placed abdominally (abdominal sacral colpopexy) or transvaginally. All of the meshes used for these procedures at the current time are macroporous polypropylene with fairly low complication charges. Many of the complications mentioned in this chapter are specific to mesh placement, though some can even occur with native tissue suture restore. The first portion of this chapter will focus on these issues particularly related to meshes, and the latter portion will talk about iatrogenic vaginal complications related to native tissue prolapse repairs. The commonest complications reported have been mesh erosion, infection, pain, and urinary signs. Physicians should search specialised training for procedures involving using mesh, and be alert and acknowledge issues early. Physicians should inform sufferers on the permanent nature of surgical mesh, and that some complications related to implanted vaginal mesh might require subsequent surgery that may or could not appropriate the complication. Physicians ought to inform sufferers in regards to the potential for serious complications and the effect on quality of life, including pain throughout intercourse, scarring, and narrowing of the vagina after prolapse repairs. It was also acknowledged that mesh placed abdominally for the remedy of pelvic organ prolapse through sacrocolpopexy had a decrease rate of mesh complications when in comparability with vaginally-placed mesh. Finally, mesh used to treat stress incontinence was to stay beneath continued investigation, with updates to come at a later date. Thus a 510(k) process based on a predicate gadget (synthetic mid-urethral sling) was the approval process, even though mesh used for prolapse repairs involves considerably elevated volumes of mesh and involves a different house in which the mesh is placed. Currently-approved artificial mid-urethral slings had been permitted by the same process based upon a prior product, the "Protegen sling," which is now not on the market because of a poor safety profile. If this occurred, then a major financial funding can be required to deliver new mesh kits to market. These mandated studies are ongoing and, in the end, will more than likely determine the long-term fate of these units.
|