|
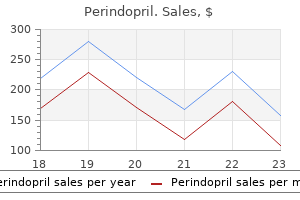
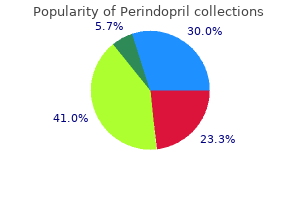
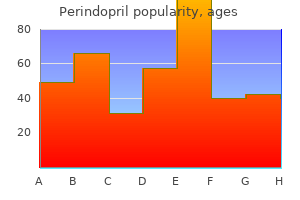
Perindopril dosages: 8 mg, 4 mg, 2 mg
Perindopril packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Order perindopril from indiaBlastoid options may also seem in a subsequent biopsy of a affected person with traditional mantle cell lymphoma, and vice versa. Mantle Cell Lymphoma Definition Mantle cell lymphoma is a B-cell lymphoma of mantle zone or major follicle lymphocytes. Clinical Features Mantle cell lymphoma typically occurs in middle-aged or older adults. It shows a striking male predominance, with the M/F ratio (up to 7: 1 in accordance with some series) being the best among the many commoner lymphoma sorts. Gastrointestinal tract involvement may or may not produce signs; some patients current with myriads of polyps in the ileocecal area (lymphomatous polyposis). Most patients have high-stage illness, and marrow involvement is very common (see Table 21A-11). Response to chemotherapy is poor (remission price solely approximately 50%); most responding sufferers relapse within 20 months. Scattered larger "naked" nuclei are current, representing follicular dendritic cells. This case reveals the traditional cytology of mantle cell lymphoma, with irregular nuclei, darkish chromatin, and scanty cytoplasm. B, Nodular progress pattern, which may lead to a misdiagnosis of follicular lymphoma. This is often an incidental finding in reactive lymph nodes-cyclin D1+ small lymphoid cells are confined to the inner mantle zones of the reactive follicles, with out coalescence or spillover into interfollicular regions. Distinction from reactive follicular hyperplasia is inconceivable with out recourse to immunohistochemistry. The solitary histiocytes dispersed among the lymphoma cells and the hyalinized venules present necessary clues that this small cell lymphoma is most likely a mantle cell lymphoma. Also because of the unknown outcome of patients identified with in situ mantle cell lymphoma, it has been instructed that the designation "mantle cell lymphoma�like B cells of undetermined significance" could also be more acceptable. Mantle cell lymphoma is unusual amongst B-cell lymphomas in that light chain is extra generally expressed than. They are unmutated in 70% to 80% of instances and show somatic hypermutation in 20% to 30% of instances. The most regularly noticed changes are lack of chromosomes thirteen and Y; deletions of 1p, 2p11, 6q, 8p, 11q2223, 13q14, 13q34, and 17p; gains at 3q26-29 and 11q; and trisomy 12. The blastoid/pleomorphic variant is related to a worse consequence in contrast with traditional mantle cell lymphoma. A excessive mitotic depend higher than 20/10 high-power fields or Ki67 index higher than 10% is related to a worse consequence. V(H)321 usage is related to an extended median survival, but the patients are inclined to be youthful at prognosis. Lymphoblastic lymphoma could mimic mantle cell lymphoma due to the irregular nuclear folding but may be distinguished from the latter by the extra delicate chromatin, greater mitotic rely, excessive likelihood of T-cell immunophenotype, and youthful age of the sufferers. The blastoid variant of mantle cell lymphoma is practically indistinguishable from lymphoblastic lymphoma, however is TdT-. Despite an excellent response to radiotherapy and/or chemotherapy, recurrence is nearly the rule. That is, follicular lymphoma is practically incurable with presently out there therapy, besides presumably stage I disease and follicular massive cell lymphoma. Special types of follicular lymphoma (pediatric, main intestinal, main cutaneous, and in situ) are discussed individually in subsequent sections. Pathology the nodal structure is effaced by neoplastic follicles, some of which may lengthen into the perinodal tissue. It is important to examine the histologic section beneath very low magnification with reduced illumination, which is able to facilitate appreciation of the follicular sample. In most instances, the follicles are organized in a back-to-back sample with barely any interfollicular tissue. A diagnosis of follicular lymphoma is tougher to make in these cases and requires consideration of other Follicular Lymphoma Definition Follicular lymphomas are tumors composed of follicular center B lymphocytes, which present a follicular organization. The patients often present with insidious painless enlargement of multiple lymph nodes, and there may be a historical past of waxing and waning of the nodes. The node is changed by carefully packed nodules with scarcely any interfollicular tissue.
Purchase perindopril nowCancer Causes Control 21: 999-1007 Kapp D S, Merino M, LiVolsi V 1982 Adenocarcinoma of the vagina arising in endometriosis: long-term survival following radiation therapy. Gynecol Oncol 14: 271-278 Haskel S, Chen S S, Spiegel G 1989 Vaginal endometrioid adenocarcinoma arising in vaginal endometriosis: a case report and literature evaluation. Gynecol Oncol forty five: 62-65 Mudhar H S, Smith J H, Tidy J 2001 Primary vaginal adenocarcinoma of intestinal kind arising from an adenoma: case report and evaluation of the literature. Staats P N, Clement P B, Young R H 2007 Primary endometrioid adenocarcinoma of the vagina: a clinicopathologic study of 18 instances. Bague S, Rodriguez I M, Prat J 2004 Malignant mesonephric tumors of the feminine genital tract: a clinicopathologic research of 9 circumstances. Elliott G B, Reynolds H A, Fidler H K 1967 Pseudo-sarcoma botryoides of cervix and vagina in being pregnant. Miettinen M, Wahlstrom T, Vesterinen E, Saksela E 1983 Vaginal polyps with pseudosarcomatous features: a clinicopathologic research of seven circumstances. Maenpaa J, Soderstrom K O, Salmi T, Ekblad U 1988 Large atypical polyps of the vagina throughout pregnancy with concomitant human papilloma virus an infection. Ostor A G, Fortune D W, Riley C B 1988 Fibroepithelial polyps with atypical stromal cells (pseudosarcoma botryoides) of vulva and vagina: a report of 13 instances. Hartmann C A, Sperling M, Stein H 1990 So-called fibroepithelial polyps of the vagina exhibiting an uncommon however uniform antigen profile characterized by expression of desmin and steroid hormone receptors but no muscle-specific actin or macrophage markers. Nucci M R, Fletcher C D 1998 Fibroepithelial stromal polyps of vulvovaginal tissue: from the banal to the bizarre. Hanski W, Hagel-Lewicka E, Daniszewski K 1991 Rhabdomyomas of female genital tract: report on two instances. Guillou L, Gloor E, De Grandi P, Costa J 1989 Post-operative pseudosarcoma of the vagina: a case report. Proppe K H, Scully R E, Rosai J 1984 Postoperative spindle cell nodules of genitourinary tract resembling sarcomas: a report of eight cases. Young R H, Scully R E 1987 Pseudosarcomatous lesions of the urinary bladder, prostate gland, and urethra: a report of three cases and evaluation of the literature. Meenakshi M, McCluggage W G 2009 Myoepithelial neoplasms involving the vulva and vagina: report of four cases. Ulbright T M, Alexander R W, Kraus F T 1981 Intramural papilloma of the vagina: proof of M�llerian histogenesis. Luttges J E, Lubke M 1994 Recurrent benign M�llerian papilloma of the vagina: immunohistological findings and histogenesis. Dobbs S P, Shaw P A, Brown L J, Ireland D 1998 Borderline malignant change in recurrent m�llerian papilloma of the vagina. Abu J, Nunns D, Ireland D, Brown L 2003 Malignant development via borderline adjustments in recurrent Mullerian papilloma of the vagina. Branton P A, Tavassoli F A 1993 Spindle cell epithelioma, the so-called combined tumor of the vagina: a clinicopathologic, immunohistochemical, and ultrastructural evaluation of 28 instances. Skelton H, Smith K J 2001 Spindle cell epithelioma of the vagina exhibits immunohistochemical staining supporting its origin from a primitive/progenitor cell inhabitants. Murdoch F, Sharma R, Al-Nafussi A 2003 Benign combined tumor of the vagina: case report with expanded immunohistochemical profile. Gallardo A, Prat J 2009 M�llerian adenosarcoma: a clinicopathologic and immunohistochemical research of 55 cases difficult the existence of adenofibroma. Liu L, Davidson S, Singh M 2003 M�llerian adenosarcoma of vagina arising in persistent endometriosis: report of a case and evaluate of the literature. Neesham D, Kerdemelidis P, Scurry J 1998 Primary malignant blended M�llerian tumor of the vagina. Sebenik M, Yan Z, Khalbuss W E, Mittal K 2007 Malignant blended mullerian tumor of the vagina: case report with review of the literature, immunohistochemical examine, and analysis for human papilloma virus. Craddock K J, Bandarchi B, Khalifa M A 2007 Blue nevi of the M�llerian tract: case collection and evaluation of the literature. Weinstock M A 1994 Malignant melanoma of the vulva and vagina in the United States: patterns of incidence and populationbased estimates of survival. DeMatos P, Tyler D, Seigler H F 1998 Mucosal melanoma of the feminine genitalia: a clinicopathologic research of forty-three instances at Duke University Medical Center. Young R H, Scully R E 1984 Endodermal sinus tumor of the vagina: a report of nine instances and evaluation of the literature.
Purchase discount perindopril onlineMenestrina F, Harris N L, Moller P 2004 Primary mediastinal massive B-cell lymphoma. Perrone T, Frizzera G, Rosai J 1986 Mediastinal diffuse largecell lymphoma with sclerosis. Chadburn A, Frizzera G 1999 Mediastinal massive B-cell lymphoma vs traditional Hodgkin lymphoma. Am J Surg Pathol 21: 242-248 Banerjee D, Silva E 1981 Mediastinal mass with acute leukemia. Arch Pathol Lab Med 105: 126-129 Kubonishi I, Ohtsuki Y, Machida K I 1984 Granulocytic sarcoma presenting as a mediastinal tumor. Report of a case and cytological and cytochemical research of tumor cells in vivo and in vitro. Histopathology 14: 465-470 Bramwell N H, Burns B F 1986 Histiocytosis X of the thymus in association with myasthenia gravis. Am J Clin Pathol 86: 224-227 Novak L, Castro C Y, Listinsky C M 2003 Multiple Langerhans cell nodules in an incidental thymectomy. Arch Pathol Lab Med 127: 218-220 Lee B H, George S, Kutok J L 2003 Langerhans cell histiocytosis involving the thymus. Arch Pathol Lab Med 127: e294-e297 Bove K E, Hurtubise P, Wong K Y 1985 Thymus in untreated systemic histiocytosis X. Jpn J Clin Oncol 24: 327-330 Perez-Ordonez B, Erlandson R A, Rosai J 1996 Follicular dendritic cell tumor: report of 13 extra instances of a distinctive entity. Clinicopathologic evaluation of 17 circumstances 1612 the Thymus suggesting a malignant potential larger than presently recognized. J Clin Pathol fifty five: 791-794 Patcher M R, Lattes R 1963 Mesenchymal tumors of the mediastinum: tumors of fibrous tissue, adipose tissue, easy muscle and striated muscle. Cancer 16: 74-94 Havlicek F, Rosai J 1984 A sarcoma of thymic stroma with options of liposarcoma. Am J Clin Pathol 82: 217-224 Hahn H P, Fletcher C D 2007 Primary mediastinal liposarcoma: clinicopathologic analysis of 24 instances. Radiology 193: 121-126 Moran C A, Rosado-de-Christenson M, Suster S 1995 Thymolipoma: clinicopathologic review of 33 circumstances. Am J Surg Pathol 14: 395-398 Argani P, de Chiocca I C, Rosai J 1998 Thymoma arising with a thymolipoma. Arch Pathol Lab Med 118: 281-282 Chan J K 1997 Solitary fibrous tumour-everywhere, and a diagnosis in vogue. Histopathology 31: 568-576 Witkin G B, Rosai J 1989 Solitary fibrous tumor of the mediastinum. Am J Surg Pathol thirteen: 547-557 Weidner N 1991 Solitary fibrous tumor of the mediastinum. Ultrastruct Pathol 15: 489-492 Witkin G B, Miettinen M, Rosai J 1989 A biphasic tumor of the mediastinum with options of synovial sarcoma. Am J Surg Pathol 13: 490-499 Suster S, Moran C A 2005 Primary synovial sarcomas of the mediastinum: a clinicopathologic, immunohistochemical, and ultrastructural research of 15 cases. Am J Surg Pathol 29: 569578 Brown L R, Reiman H M, Rosenow E C 1986 Intrathoracic lymphangioma. Mayo Clin Proc sixty one: 882-892 Patcher M R, Lattes R 1963 Mesenchymal tumors of the mediastinum: tumors of lymph vascular origin. Semin Diagn Pathol eight: 14-34 Patcher M R, Lattes R 1963 Mesenchymal tumors of the mediastinum: tumors of blood vascular origin. Cancer 16: 95-107 Moran C A, Suster S 1995 Mediastinal hemangiomas: a research of 18 circumstances with emphasis on the spectrum of morphological features. Suster S, Moran C A, Koss M N 1994 Epithelioid hemangioendothelioma of the anterior mediastinum. Ulbright T M, Clark S A, Einhorn L H 1985 Angiosarcoma related to germ cell tumors. Suster S, Moran C A, Koss M N 1994 Rhabdomyosarcomas of the anterior mediastinum: report of 4 circumstances unassociated with germ cell, teratomatous, or thymic carcinomatous components. Lindskog B I, Malm A 1965 Diagnostic and surgical considerations on mediastinal (intrathoracic) goiter.
Cheap 2mg perindopril overnight deliveryPapillary development is usually present no much less than focally and is incessantly the predominant progress pattern. The tumor cells often pile as much as kind tufts that project above the surfaces of the papillae. A micropapillary pattern in which lengthy, skinny tufts of tumor cells grow into cystic spaces can be frequent. Tumor cells line glands and cystic spaces, diffusely infiltrate fibrotic stroma, or kind strong nests and sheets. Elongated slit-like glands inside foci of stable development are a attribute finding in high-grade serous carcinoma. Foci of microcystic growth, typically with admixed signet ring cells, are famous occasionally. Some authors take a restrictive approach and think that a diagnosis of high-grade serous carcinoma is acceptable just for predominantly papillary tumors with minor glandular or solid areas. Others have adopted a more inclusive classification scheme and consider most high-grade carcinomas with some features of serous differentiation as types of high-grade serous carcinoma, together with tumors with in depth strong areas, tumors with high-grade glandular areas with out squamous differentiation, and some tumors with clear cell or transitional cell areas. Low-grade serous carcinoma has been proven to have a different molecular foundation than high-grade serous carcinoma. Crowded glands, simple or complex micropapillae, and stable or cribriform nests of tumor cells infiltrate a fibrous stroma. Zones of invasive carcinoma may be combined with zones of serous borderline tumor, often of the micropapillary kind. Micropapillary fronds, many surrounded by clear areas, infiltrate the ovarian stroma. They are often present in serous tumors, particularly serous carcinomas, and are occasionally numerous. Rarely, psammoma bodies are so quite a few in a low-grade serous carcinoma that they obscure the epithelial components of the tumor. Such carcinomas, termed serous psammocarcinomas, have a extremely favorable prognosis when they are often excised utterly. Although psammoma bodies are suggestive of a serous tumor, in addition they could be present in association with other forms of tumors and such nonneoplastic circumstances as epithelial inclusion cysts and endosalpingiosis. Grading of Serous Carcinoma Grading of ovarian carcinomas has not been standardized. Silverberg and colleagues141 proposed a "universal" grading system they thought could possibly be used for all types of ovarian carcinomas. With this method, the grade of a carcinoma is set by the degree of nuclear atypia, the frequency of mitotic figures, and the extent to which the tumor cells type papillae or glands (Table 13A-5). More just lately, a binary grading system, in which low-grade serous carcinoma almost at all times falls into grade 1 of the universal grading system, has gained larger acceptance than the universal grading system because it higher displays the present thinking that highgrade and low-grade serous carcinomas symbolize two completely different tumor types rather than two different grades of the same type of tumor. In the binary system, lowgrade serous carcinoma is a tumor that displays gentle to reasonable nuclear atypia and 12 or fewer mitotic figures per 10 hpf. Mitotic exercise is excessive, with a median of 38 mitotic figures per 10 hpf in one research. Architectural score Predominantly glandular Predominantly papillary Predominantly strong 2. Tumor grade 3-5 points 6, 7 factors 8, 9 factors hpf, High-powered fields; mf, mitotic figures. The postchemotherapy immunophenotype is similar to that of untreated serous carcinoma. Staining is noticed in roughly 20% of mesotheliomas, however usually in a weak and focal pattern, meaning that this antibody also can be used with caution for differentiating between serous carcinoma and mesothelioma. This multilocular cystic neoplasm is lined by a single layer of columnar mucinous cells. Borderline and malignant mucinous tumors are less numerous than their serous counterparts, and borderline mucinous tumors greatly outnumber mucinous carcinomas. The cut floor reveals unilocular or multilocular mucin-filled cysts of varying dimension. Mucinous adenofibroma is a predominantly stable, white or tan, fibrous tumor that incorporates small mucin-filled cysts. Mucinous cystadenofibroma is a cystic tumor that has solid fibrous areas much like a mucinous adenofibroma.
Generic perindopril 4mg visaThey are typically aged, with a imply age of sixty nine years,211 and their symptoms are just like those of other sufferers with bladder most cancers; gross hematuria is the most typical criticism. Hypercalcemia has been current in at least one case217 and ectopic adrenocorticotropic hormone manufacturing in one other. The prognosis is mostly poor,214 but occasionally radical cystectomy and aggressive adjuvant chemotherapy have resulted in long-term survival. The tumors could include small rosette-like structures or, much less commonly, malignant large cells. Cases having options just like those of huge cell neuroendocrine carcinoma of the lung are additionally seen (see later discussion). Other types of carcinoma, normally either in situ or invasive urothelial carcinoma, however often squamous cell carcinoma or adenocarcinoma, are present in roughly half of the circumstances. Immunohistochemical stains for lymphoid and epithelial markers could also be useful in these instances. Primary small cell carcinoma of the bladder should be distinguished from a metastasis. Direct extension from prostatic small cell carcinoma additionally needs to be thought-about; this most often occurs within the setting of recognized prostatic adenocarcinoma and often has an adenocarcinoma component. Prostatic small cell carcinoma is way less frequent than such urinary bladder tumors. Large Cell Neuroendocrine Carcinoma A few examples of main massive cell neuroendocrine carcinoma have been reported. Mixed histology is usually current with urothelial carcinoma, squamous cell carcinoma, or adenocarcinoma. Distinction from a high-grade urothelial carcinoma requires demonstration of neuroendocrine differentiation. Most are cured by transurethral resection, however local recurrence and metastases have occurred. The nice rarity of carcinoid of the bladder signifies that the prognosis ought to be made solely after other tumors that may simulate carcinoid have been excluded. Small cell carcinoma can have carcinoid-like areas but should be reported as small cell carcinoma. Some urothelial carcinomas grow in the form of nests that superficially resemble these of a carcinoid. Differences within the cytologic features of urothelial carcinoma and carcinoid and the efficiency of silver stains, immunohistochemistry, or electron microscopy should set up the prognosis. Given the limited expertise with these tumors, most authors favor making a diagnosis of leiomyosarcoma in tumors with reasonable nuclear atypia, even a number of mitotic figures, or an infiltrative growth sample. MalignantMesenchymalTumors Primary sarcomas of the urinary bladder are additionally unusual. A distinct age distribution is seen with rhabdomyosarcoma occurring in youngsters and leiomyosarcoma being most typical in adults. In addition, virtually all other forms of sarcoma including fibrosarcoma,263 unclassified pleomorphic sarcoma (socalled malignant fibrous histiocytoma),264 osteosarcoma,265 chondrosarcoma,266 angiosarcoma,239 so-called hemangiopericytoma,267 liposarcoma,268 and perivascular epithelioid cell tumor269 happen not often in the bladder. All of those must be identified solely after sarcomatoid carcinoma has been excluded fastidiously. Leiomyosarcoma Leiomyosarcoma is the most common sarcoma of the urinary bladder in adults,258,259,270 accounting for 57% of all main sarcomas (excluding rhabdomyosarcoma). This age distribution contrasts with that of vesical rhabdomyosarcoma, which happens mainly in kids. Treatment is primarily surgical with survival being related to stage and histologic grade. The differential diagnosis of leiomyosarcoma and sarcomatoid urothelial carcinoma has been mentioned earlier. Another necessary distinction is between leiomyosarcoma and nonneoplastic myofibroblastic proliferations.
Actaea racemosa (Black Cohosh). Perindopril. - What is Black Cohosh?
- Are there safety concerns?
- Premenstrual syndrome (PMS), osteoporosis, painful menstruation, labor induction, upset stomach, muscle pain, fever, sore throat, cough, repelling insects, acne, mole and wart removal, and other conditions.
- What other names is Black Cohosh known by?
- Menopausal symptoms such as hot flashes.
- Is Black Cohosh effective?
- Are there any interactions with medications?
- Dosing considerations for Black Cohosh.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96830
Safe 8 mg perindoprilFalk S, Takeshita M, Stutte H J 1988 Epithelioid granulomatosis with preliminary and predominant manifestation in spleen. Suster S, Moran C A, Blanco M 1994 Mycobacterial spindle-cell pseudotumor of the spleen. Horny H P, Kaiserling E 1988 Lymphoid cells and tissue mast cells of bone marrow lesions in systemic mastocytosis: a histological and immunohistological study. Parwaresch M R, Horny H P, Lennert K 1985 Tissue mast cells in well being and illness. Ryan R J, Akin C, Castells M 2012 Mast cell sarcoma: a rare and potentially under-recognized diagnostic entity with specific therapeutic implications. Rywlin A M 1982 Mastocytic eosinophilic fibrohistiocytic lesion of the bone marrow. Pardanani A, Akin C, Valent P 2006 Pathogenesis, medical features, and treatment advances in mastocytosis. Blood 99: 1741-1744 21 Tumors of the Lymphoreticular System, Including Spleen and Thymus 1555 198. Husni E A 1961 the clinical course of splenic hemangioma, with emphasis on spontaneous rupture. A case report with enzymehistochemical, immunohistochemical, and electron-microscopic findings. Tarazov P G, Polysalov V N, Ryzhkov V K 1990 Hemangiomatosis of the liver and spleen: profitable treatment with embolization and splenectomy. Arber D A, Strickler J G, Weiss L M 1997 Splenic mesothelial cysts mimicking lymphangiomas. Buckner J W 3rd, Porterfield G, Williams G R 1990 Spontaneous splenic rupture secondary to angiosarcoma. Chen K T, Bolles J C, Gilbert E F 1979 Angiosarcoma of the spleen: a report of two instances and review of the literature. Rosso R, Gianelli U, Chan J K 1996 Further evidence supporting the sinus lining cell nature of splenic littoral cell angiosarcoma. Morphologic, immunohistochemical findings and consideration of histogenesis of a uncommon splenic tumor. Budke H L, Breitfeld P P, Neiman R S 1995 Functional hyposplenism due to a main epithelioid hemangioendothelioma of the spleen. Yoda Y, Ohashi M 2012 A case of composite hemangioendothelioma arising from the spleen. Yu L, Yang S J 2011 Kaposiform hemangioendothelioma of the spleen in an adult: an initial case report. Krishnan J, Frizzera G 2003 Two splenic lesions in need of clarification: hamartoma and inflammatory pseudotumor. Kraus M D, Dehner L P 1999 Benign vascular neoplasms of the spleen with myoid and angioendotheliomatous features. Hulbert J C, Graf R 1983 Involvement of the spleen by renal angiomyolipoma: metastasis or multicentricity Mallipudi B V, Chawdhery M Z, Jeffery P J 1998 Primary malignant fibrous histiocytoma of spleen. Sheahan K, Wolf B C, Neiman R S 1988 Inflammatory pseudotumor of the spleen: a clinicopathology examine of three circumstances. Seijo L, Unger P D, Strauchen J A 1996 Inflammatory pseudotumor of the spleen, a case report and evaluate of the literature. Darden J W, Teeslink R, Parrish A 1975 Hamartoma of the spleen: a manifestation of tuberous sclerosis. Am J Surg Pathol 29: 109-114 21 Tumors of the Lymphoreticular System, Including Spleen and Thymus 1557 300. Morinaga S, Ohyama R, Koizumi J 1992 Low-grade mucinous cystadenocarcinoma in the spleen. Jorgensen L N, Chrintz H 1988 Solitary metastatic endometrial carcinoma of the spleen. Gilks C B, Acker B D, Clement P B 1989 Recurrent endometrial adenocarcinoma: presentation as a splenic mass mimicking malignant lymphoma. Abrams H L, Spiro R, Goldstein N 1950 Metastases in carcinoma, evaluation of 1000 autopsied circumstances.
Syndromes - Transfusion reaction
- Weakened immune system
- Some pregnant women with fibroids may deliver a premature baby because there is not enough room in the womb.
- Systemic sclerosis
- Acute renal failure
- Exposure to contaminated or untreated drinking water
- Dizziness
- Acamprosate is a drug that has been shown to lower relapse rates in those who are alcohol dependent.
Perindopril 2 mg amexThis could additionally be accompanied by a desmoplastic reaction or inflammatory reaction together with granuloma formation. The medical significance of microscopic metastasis comprising single or small clusters of cells, revealed solely on immunohistochemical staining but not on morphologic evaluation, continues to be controversial. A panel of antibodies ought to be used, ideally together with at least antibodies to cytokeratin, lymphoid markers, and S100 protein. Prediction of the Primary Site for Metastatic Carcinoma About 3% to 4% of carcinomas present with metastases from an occult primary neoplasm. For example, a breast or lung main has to be significantly thought-about for axillary lymph nodes, and a breast, lung, or genital organ origin has to be thought of for supraclavicular nodes. Morphologic assessment can provide important diagnostic clues and assist in the choice of special studies. Undifferentiated carcinoma of the nasopharynx can often be suspected on the premise of the presence of sheets of cells with indistinct mobile outlines, crowded vesicular nuclei, and prominent nucleoli. Immunohistochemical research are significantly helpful in chosen conditions, as listed in Table 21A-21. The tumor is well circumscribed, with compressed lymph node tissue on the periphery. It consists of intersecting fascicles of bland-looking spindle cells that are in all probability myofibroblasts. The interfollicular infiltration and intermingling of tumor cells with lymphocytes could prompt a prognosis of lymphoma. The epithelial nature of this tumor is typically recommended by the presence of obscure cellular groupings, similar to in the proper area. In nasopharyngeal carcinoma, the cell borders are usually vague and the nuclei are vesicular. Hemorrhagic spindle cell tumor with amianthoid fibers (palisaded myofibroblastoma) 2. Nevus cell aggregates and blue nevus formation of stellate collagen nodules (amianthoid fibers). Interstitial hemorrhage is usually distinguished, and a hemorrhagic zone could also be present within the periphery. Angiomyomatous Hamartoma this lesion occurs almost solely in inguinal lymph nodes and could also be accompanied by ipsilateral lymphedema. Proliferation of thick-walled blood vessels within the nodal hilum extends into the nodal parenchyma in the form of haphazardly disposed smooth muscle cells in a sclerotic stroma. Sometimes, the lesion happens as an incidental discovering in pelvic lymph nodes (nodal lymphangiomyoma). That is, these lesions belong to the household of perivascular epithelioid cell tumors. Lymph node can additionally be very not often involved by angiomyolipoma, often in affiliation with a renal tumor. Deciduosis of Lymph Node In pregnant ladies, compact masses of decidual cells could additionally be present in intra-abdominal lymph nodes. The absence of desmoplastic reaction, mitotic figures, and keratinization distinguishes this lesion from metastatic squamous cell carcinoma. Short fascicles of spindle cells are interspersed with slender, branching vascular spaces. Kaposi Sarcoma of Lymph Node Clinical Features and Epidemiology Kaposi sarcoma is a particular vascular tumor of lymphatic origin, incessantly showing multicentric progress (see Chapter 3). It occurs in several scientific settings, associated with different prognosis1,1703-1711: 1. Cutaneous lesions occurring in younger adults; the disease can be indolent or progressive. Lymphadenopathic type, occurring primarily in kids; the illness is rapidly progressive. The illness is usually fulminant and disseminated, involving mucocutaneous websites, lymph nodes, and visceral organs.
Purchase perindopril 4 mg without a prescriptionKato H, Suzuki M, Mukai M, Aizawa S 1999 Clinicopathological study of pheochromocytoma of the urinary bladder: immunohistochemical, circulate cytometric and ultrastructural findings with evaluate of the literature. Zhou M, Epstein J I, Young R H 2004 Paraganglioma of the urinary bladder: a lesion that could be misdiagnosed as urothelial carcinoma in transurethral resection specimens. Khan O, Williams G, Chisholm G D, Welbourn R B 1982 Phaeochromocytomas of the bladder. Usuda H, Emura I 2005 Composite paraganglioma-ganglioneuroma of the urinary bladder. Tainio H M, Kylmala T M, Haapasalo H K 1999 Primary malignant melanoma of the urinary bladder associated with widespread metastases. Khalbuss W E, Hossain M, Elhosseiny A 2001 Primary malignant melanoma of the urinary bladder diagnosed by urine cytology: a case report. Talmon G, Khan A, Koerber R, Johansson S 2010 Simple melanosis of the bladder: a uncommon entity. Kuyumcuoglu U, Kale A 2008 Unusual presentation of a dermoid cyst that derived from the bladder dome presenting as subserosal leiomyoma uteri. Jain S K, Kaza R C, Vindal A, Bains L 2010 Vesical dermoid: an unusual presentation. Bates A W, Baithun S I 2000 Secondary neoplasms of the bladder are histological mimics of nontransitional cell major tumours: clinicopathological and histological options of 282 instances. Silverstein L I, Plaine L, Davis J E, Kabakow B 1987 Breast carcinoma metastatic to bladder. Marshall F C, Uson A C, Melicow M M 1960 Neoplasma and caruncles of the female urethra. Kaneko G, Nishimoto K, Ogata K, Uchida A 2011 A case of intraepithelial squamous cell carcinoma arising from urethral caruncle. Omar A, Thomas A, Thompson I 2007 Primary urethral transitional cell carcinoma presenting as a urethral caruncle. Bruijnes E, de Wall J G, Scholtmeijer R J, den Hollander J C 1985 Congenital polyp of the prostatic urethra in childhood. Isaac J, Snow B, Lowichik A 2006 Fibroepithelial polyp of the prostatic urethra in an adolescent J Pediatr Surg forty one: e29-e31 347. Dalbagni G, Zhang Z F, Lacombe L, Herr H W 1998 Female urethral carcinoma: an evaluation of treatment consequence and a plea for a standardized management strategy. Dalbagni G, Zhang Z F, Lacombe L, Herr H W 1999 Male urethral carcinoma: analysis of therapy outcome. Colapinto V, Evans D H 1977 Primary carcinoma of the male urethra developing after urethroplasty for stricture. Trabulsi E J, Hoffman-Censits J 2010 Chemotherapy for penile and urethral carcinoma. Begin L R, Deschenes J, Mitmaker B 1991 Pagetoid carcinomatous involvement of the penile urethra in affiliation with highgrade transitional cell carcinoma of the urinary bladder. Grussendorf-Conen E I, Deutz F J, de Villiers E M 1987 Detection of human papillomavirus-6 in major carcinoma of the urethra in men. Diaz-Cano S J, Rios J J, Rivera-Hueto F, Galera-Davidson H 1992 Mixed cloacogenic carcinoma of male urethra. Salehi M, Falahatkar S, Neiroomand H, Akbarpour M 2009 Fibroepithelial congenital polyp of prostatic urethra in an adult man. Debenedictis T J, Marmar M L, Praiss D E 1977 Intraurethral condylomas acuminata: administration and evaluate of the literature. Bissada N K, Cole A T, Fried F A 1974 Extensive condylomas acuminata of the complete male urethra and the bladder. Huvos A G, Grabstald H 1973 Urethral meatal and parameatal tumors in young males: a clinicopathologic and electron microscopic examine. Maung R, Kelly J K, Grace D A 1988 Intestinal metaplasia and dysplasia of prostatic urethra secondary to stricture. Powell I, Cartwright H, Jano F 1981 Villous adenoma and adenocarcinoma of feminine urethra. Samaratunga H, Letizia B 2007 Prostatic ductal adenocarcinoma presenting as a urethral polyp: a clinicopathological examine of eight instances of a lesion with the potential to be misdiagnosed as a benign prostatic urethral polyp.
8 mg perindopril with mastercardConsistent abnormalities are discovered within the -catenin gene, and the irregular immunohistochemical nuclear localization of -catenin (and downstream components corresponding to cyclin D1) staining has been proposed as a diagnostic aid. Interestingly, one case was proven to have a particular unbalanced translocation between chromosomes thirteen and 17. Solid pseudopapillary neoplasms histologically just like these in the pancreas have been rarely described outside the pancreas,a hundred and fifteen significantly within the ovary. In distinction to the more commonly occurring tumors of epithelial origin, nonepithelial tumors of the pancreas are very rare. Most frequent are leiomyosarcoma129 and malignant peripheral nerve sheath tumor, adopted by liposarcomas and unclassified pleomorphic sarcomas (so-called malignant fibrous histiocytomas). Malignant lymphomas and leukemic infiltrates might occasionally be seen in the pancreas. Metastases involving the pancreas are unusual and include metastases from renal cell carcinoma, breast carcinoma, small cell lung carcinoma, and melanoma. Among the strong nonneoplastic lesions are the "inflammatory pseudotumors" and the hamartomas32,140,141; among the many cystic lesions are the pseudocysts; lymphoepithelial cysts; and congenital, retention, and parasitic cysts. Patients usually have serum elevation of immunoglobulin IgG4, a discovering that will assist distinguish the lesion clinically from that of pancreatic ductal adenocarcinoma. In addition to pancreatoblastoma (see earlier discussion), acinar cell carcinomas (see earlier discussion), well-differentiated neuroendocrine tumors (see Chapter 20), and solid pseudopapillary neoplasms (see earlier discussion) can happen, whereas ductal adenocarcinoma is just about absent. This infiltrate first appears around medium-sized ducts and later additionally spreads to the acinar lobuli. The extension of the infiltrate to the acinar lobules is related to the event of intense fibrosis that may virtually substitute the acinar tissue and is usually related to quite a few myofibroblasts organized in a storiform pattern. If the latter change prevails, autoimmune pancreatitis resembles inflammatory myofibroblastic tumor (formerly referred to as inflammatory pseudotumor). The disease may happen at all ages however is commonest between 50 and 60 years of age. Successful therapy with steroids may be achieved if the prognosis is acknowledged before surgery, however the radiographic resemblance of autoimmune pancreatitis to pancreatic carcinoma can result in radical surgery for a presumed malignant diagnosis. Immunohistochemical staining for IgG4 could be helpful to help a analysis of autoimmune pancreatitis if a diffuse, dense IgG4positive plasma cell infiltrate exists. A second variant of autoimmune pancreatitis (type 2, in distinction to the classic or kind 1 autoimmune pancreatitis described earlier) shares the periductal lymphoplasmacytic infiltrate but additionally exhibits a neutrophilic infiltrate within the ductal epithelium ("granulocytic epithelial lesions") and has much less dense fibrosis, much less developed obliterative venulitis, and more edema within the lobules. The second type of continual pancreatitis which might be clinically mistaken for pancreatic cancer is paraduodenal pancreatitis (synonyms: cystic dystrophy of the duodenal wall, para-ampullary duodenal wall cyst, and groove pancreatitis). Typically cystic and/or pseudocystic adjustments are seen in affiliation with mobile fibrotic tissue that normally extends by way of the duodenal wall into the close by pancreatic tissue around the bile duct. As a sine qua non they need to arise in the middle of pancreatitis, usually of alcoholic, hardly ever of hereditary origin. In: Hamilton S R, Aaltonen L A (eds) Pathology and genetics of tumours of the digestive system. Makhlouf H R, Almeida J L, Sobin L H 1999 Carcinoma in jejunal pancreatic heterotopia. Andea A, Sarkar F, Adsay N V 2003 Clinicopathological correlates of pancreatic intraepithelial neoplasia: a comparative analysis of 82 circumstances with and 152 cases without pancreatic ductal adenocarcinoma. Cubilla A L, Fitzgerald P J 1976 Morphological lesions associated with human primary invasive nonendocrine pancreas cancer. In: Dom�nguez-Mu�oz J E (ed) Clinical pancreatology for practising gastroenterologists and surgeons. Kloppel G, Adsay N V 2009 Chronic pancreatitis and the differential analysis versus pancreatic most cancers. Recommendations for the reporting of pancreatic specimens containing malignant tumors. L�ttges J, Zamboni G, Kl�ppel G 1999 Recommendation for the examination of pancreaticoduodenectomy specimens faraway from patients with carcinoma of the exocrine pancreas. A proposal for a standardized pathological staging of pancreaticoduodenectomy specimens including a checklist. Schlitter A M, Esposito I 2010 Definition of microscopic tumor clearance (r0) in pancreatic resections. Conlon K C, Klimstra D S, Brennan M F 1996 Long-term survival after healing resection for pancreatic ductal adenocarcinoma. Adsay N V 2002 Intraductal papillary mucinous neoplasms of the pancreas: pathology and molecular genetics.
|