|
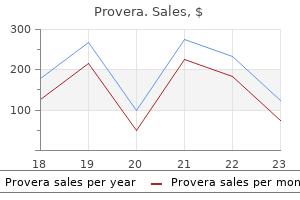
Provera dosages: 10 mg, 5 mg, 2.5 mg
Provera packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy provera torontoAssociated diseases It could also be related to affective disease (anxiety and depression) but this should not mislead the clinician into thinking that melancholy and anxiousness are the causes of the illness [3]. Investigations Investigations fail to show any trigeminal nerve or central neuropathy. Pathophysiology the pathophysiology is unknown, but in all probability includes dysfunction of the peripheral and/or central sensory nerve pathways which innervate the genital areas, or are liable for consciousness of genital sensation [4]. Vulovodynia, scrotodynia and penodynia Definition and nomenclature Vulvodynia and penoscrotodynia involve irregular sensations of the skin in sitespecific places. Chronic scalp pain Definition and nomenclature Scalp pain and tenderness with none scalp disease is another mucocutaneous pain syndrome. It follows the sample of different mucocutaneous ache syndromes in that sufferers complain of (usually) severe continual pain affecting the scalp and/or hair, which can be provoked by contact. Synonyms and inclusions � Trichodynia � Scalp allodynia Presentation There is usually little or no to see by the use of bodily indicators. The diagnosis is considered one of exclusion, although the clinical history and examination normally permit clinicians to make the analysis clinically [5]. Differential diagnosis the differential prognosis contains genital dermatoses which may usually be excluded clinically. Some sufferers have genital pain syndromes as a part of a more generalized ache syndrome disease. Complications and comorbidities Psychosexual and psychosocial comorbidities are frequent. Treatment is normally successful though it might take a while to obtain remission or symptom amelioration. Clinicians and sufferers might should search via trial and error for the remedy that most closely fits the person patient. Some authors indicate that the thalamus may be appearing dysfunctionally and that this will likely result in scalp allodynia amongst different cutaneous ache syndromes [1,2]. Management All sufferers have to be referred to a patient advocacy group, and given opportunities to be taught as much as they want about their disease. Clinical features Differential diagnosis the differential prognosis includes all scalp dermatoses. In the absence of scalp illness, the analysis trichodynia can be made clinically with an acceptable clinical historical past. Warn that this is also an antidepressant (although not normally used in antidepressant doses for genital ache syndromes). Synonyms and inclusions � Mitchell disease � Acromelalgia � Red neuralgia � Erythermalgia Differential diagnosis the differential diagnoses embody peripheral neuropathy, connective tissue diseases, Raynaud phenomenon, acrocyanosis and peripheral vascular illness [3]. Management Treatment of erythromelalgia is troublesome and usually achieved via trials of medication with the affected person. Third line brokers embrace intravenous brokers such as lidocaine, sodium nitroprusside or prostaglandins. For sufferers not aware of medical therapy, invasive procedures corresponding to sympathetic blockade, sympathectomy or dorsal cord stimulation may be thought of [4]. All sufferers ought to be educated to avoid frightening components, corresponding to warmth, dependent positioning, train and alcohol. Behaviours which will exacerbate the condition (such as utilizing ice packs) ought to be strongly discouraged. Some patients feel very wretched and may even consider suicide, so assessment of psychosocial comorbidities and risk is essential. Age Part 7: Psychological, sensory & neurological the typical age of presentation is 60 years, though diagnoses have been made in youngsters. Recently, nonetheless, many sufferers with erythromelalgia had been found to have a distal cutaneous smallfibre neuropathy that diminished sudomotor operate (sweating). It has been postulated that this neuropathy reduces the sympathetic vasoconstrictive response, which finally ends up in an elevated acral blood move. As a end result there could also be decreased oxygenation of the pores and skin and subcutaneous tissue, additional scary signs [2].
Order provera overnightIn some circumstances nodules come up from normal pores and skin in sufferers genetically predisposed to keloid formation [220]. In a histological and ultrastructural analysis in a patient with nodular morphoea on a background of diffuse cutaneous systemic sclerosis, Moinzadeh et al. Deep morphoea can thus mimic lipoatrophy clinically and should be thought-about in patients presenting with asymptomatic atrophic lesions. Generalized type Generalized morphoea has been outlined in quite a lot of ways in the literature. Falanga instructed 5 or more lesions, bilateral lesions and proof of becoming a member of together of at least two individual patches [94]. Laxer and Zulian [6] defined generalized morphoea as induration of the pores and skin starting as four or extra individual plaques, larger than three cm, that become confluent and contain at least two out of seven anatomical websites (head�neck, right higher extremity, left higher extremity, right lower extremity, left lower extremity, anterior trunk, posterior trunk). Based on these definitions, the literature suggests that generalized morphoea accounts for 7�9% of childhood morphoea cases [8,22,30,35] and between 13% and 52% of adult circumstances [9,22,28,35]. Extracutaneous signs including myalgia, arthralgia and fatigue are common, dyspnoea and dysphagia might happen, and the next prevalence of concurrent and familial autoimmune illness are documented (see the sections on genetics and complications and comorbidities on this chapter). Plaques could happen in different phases of evolution and are most incessantly positioned on the trunk, thighs and lumbosacral space in adults. Multiple, isolated, usually symmetrically distributed plaques could also be present, or bigger, coalescent plaques might develop in an isomorphic sample due to minor trauma from clothing across the waistband, under the breasts and within the groins (see Predisposing factors in this chapter) [189,235]. The isomorphic distribution pattern appears notably frequent in middleaged females [189]. In the most important multicentre research in youngsters, coinvolvement of the trunk and limbs occurred in 63% and of the trunk, limbs and head in 19% of circumstances [8,19]. Both adults and kids initially presenting with limited plaque morphoea may, as a outcome of ongoing or recurrent disease activity, progress to fulfil the criteria for the disseminated plaque subtype of generalized morphoea. Pansclerotic morphoea has variably been included within either the generalized [7] or deep [5] subtypes or as a separate subtype of morphoea [6] in published classifications. The pores and skin is tethered to the underlying concerned deep tissues giving a puckered look and bounddown feeling. Although a majority of the circumstances they described had widespread, deep involvement, some had particular person plaques in line with a prognosis of restricted deep morphoea (synonym solitary morphoea profunda). The primary histopathological features are sclerosis and hyalinization of collagen, and a putting accumulation of inflammatory cells within the deep dermis as nicely as within the subcutaneous tissue, which is predominantly composed of plasma cells and T and B lymphocytes [230]. Increased numbers of eosinophils may be current within the skin and circulation [230,231]. Rarely, a plasma cell panniculitis has been described (synonym morphoea panniculitis) [232]. Occasionally, lesions present as noninflammatory, cupuliform, depressed plaques with no associated induration, pigmentation or texture Clinical features 57. It is principally referred to as disabling pansclerotic morphoea of childhood within the literature and is incessantly difficult by extreme joint contractures, chronic ulceration and the development of squamous cell carcinoma [238�241]. Whilst the previous descriptions of pansclerotic morphoea in childhood recommend deep tissue involvement, including subcutaneous tissue, muscle and bone [236,238], the definition and frequency of involvement past the dermis has been inconsistent [237,244�248]. Because of the relative ambiguity as regards depth of involvement, in the literature, this criterion was removed, and pansclerotic morphoea was defined because the presence of near complete body floor space involvement with sparing of the fingers and toes. A majority had onset of lesions on the trunk with fast centrifugal spread and abrupt cutoff at the metacarpo and metatarsophalangeal joints. However, patients with the pansclerotic subtype were more more doubtless to be male (46% versus 6% of generalized morphoea patients) and have a shorter time to analysis, higher charges of functional impairment (61% versus 16%) and better skin sclerosis and damage scores. Even though it was not a defining issue, a high frequency of deep involvement on tissue biopsy (61% versus 17%) was observed. Restrictive defects on pulmonary operate exams, dysphagia and/or hand oedema had been recognized in 4/13 sufferers and following investigation had been attributed to extreme, extensive pores and skin sclerosis quite than inside organ involvement per se [10]. There is important clinical overlap between pansclerotic morphoea as outlined above and the various forms of deep morphoea described within the literature. The time period subcutaneous morphoea was initially coined by Person and Su in 1979, who described sixteen circumstances with biopsyproven inflammatory sclerosis of the panniculus or facscia, thirteen of whom had extensive, illdefined, bounddown plaques with a speedy centrifugal development [229]. Three years later they added seven circumstances and reviewed the revealed literature describing patients with deep involvement [146]. On the premise that involvement of the deep dermis, subcutaneous fats, fascia or muscle can be present alone or in any mixture, they renamed the situation morphoea profunda, and included eosinophilic fasciitis within its spectrum [146].
Discount provera 10 mg lineThere has been a current international effort, not only to better understand the impression that morphoea can have on sufferers, but also to develop and validate scientific outcome measures and consensus therapy tips [25,26,27]. Peterson discovered that general, plaque morphea was the most typical subtype (56% of cases), followed so as of frequency by linear (20%), generalized (13%) and deep (11%) subtypes [28]. Linear morphoea was again the most frequent childhood subtype (65%), followed by plaque morphea (26%), generalized morphea (7%) and deep morphea (2%) [8]. These knowledge are corroborated by two additional large North American research collectively overlaying 381 kids. Linear morphoea occurred in 42�54%, followed by plaque in 15�28% and generalized types in 7�11% [9,30]. In these research 15�23% of youngsters had a mixed subtype, and linear� plaque was probably the most frequent combination (60�85%) [8,9,30]). In adults, plaque morphoea is the most typical subtype (28�44% of cases), adopted by generalized (24%) and linear (15%) forms [9,22,31]. There are fewer data concerning the frequency of mixed subtypes in adults, though one examine recognized them in 4% of a hundred and twenty grownup cases [9]. They could also be seen more commonly in patients with childhood onset rather than grownup onset of disease. Very uncommon circumstances of linear morphoea and atrophoderma of Pasini�Pierini presenting at birth have been described [32,33]. In general, 75% of plaque illness happens between the ages of 40 and 50 years, whereas 75% of linear illness occurs between the ages or 2 and 14 years. Sex Most studies suggest that morphoea is commoner in women, with feminine to male ratios of between 7: 1 and a pair of. Disorders reported to happen concomitantly with morphoea in case stories embody psoriasis, vitiligo, alopecia areata, autoimmune hepatitis, main biliary cirrhosis, inflammatory bowel disease, type 1 diabetes, autoimmune thyroid illness, polyglandular autoimmune disease sort 2, M�ni�re illness, coeliac illness, multiple sclerosis, systemic lupus erythematosus, rheumatoid arthritis, Sj�gren syndrome, antiphospholipid syndrome, Still disease and mixed connective tissue illness [38�40] (reviewed in [9,19]). In a bid to perceive which of these are true associations, some larger research have been undertaken in latest years. Amongst 123 adults and 122 youngsters from Texas, concomitant rheumatic or other autoimmune issues had been identified in 18% of patients, and were a lot commoner in adults (30%) than kids (5%) [9]. This association was most marked amongst adults and youngsters with generalized morphoea, occurring in 46% of this group versus 9% within the different subtypes mixed. In this study the prevalence of psoriasis, systemic lupus erythematosus, a quantity of sclerosis and vitiligo appeared significantly larger in sufferers with morphoea than within the background inhabitants. In a multicentre worldwide study of 750 children, concomitant autoimmune illness was identified in 1. In a retrospective German study of 472 patients (381 adults), essentially the most incessantly related autoimmune illnesses were Hashimoto thyroiditis, rheumatoid arthritis, alopecia areata and kind 1 diabetes [41]. Interestingly, the offspring of oldsters with morphoea appear at higher threat of creating rheumatoid arthritis [42]. Lichen sclerosus�morphoea overlap Cases of lichen sclerosus (also see Chapters 111 and 112) occurring in conjunction with morphoea are actually properly documented [46]. In earlier printed instances many of the coexistent lichen sclerosus was extragenital, but more lately, bigger studies have recognized increasing numbers of patients with genital disease, which can current concurrently or several years after the onset of morphoea [41,47,48]. In a retrospective research of 472 morphoea sufferers from Germany (381 adults, with a mean age of forty six years), lichen sclerosus was identified and histopathologically confirmed in 5. There was an increased prevalence of lichen sclerosus amongst sufferers with morphoea compared with the final inhabitants (1: 300�1: 1000), with an odds ratio of over 18 [41]. This could additionally be an underestimate for the rationale that anogenital space was only examined in this study in patients with suggestive medical signs similar to burning, itching, pain, dysuria or dyspareunia, and so asymp- tomatic patients, or those not admitting to signs, would have been missed. Accordingly, in a French research of seventy six sufferers with morphoea (58 feminine, median age 59 years), who underwent a mandatory full scientific examination, 38% had been discovered to have genital lichen sclerosus in contrast with 3% of the management group. Again, the condition was a lot commoner in patients with plaque morphoea (45%, 22/29 cases) [48]. That these two conditions coexist is clear, however their relationship is still in question.
Purchase genuine proveraThe pores and skin and hair have been normal in all affected people, but some had lacrimal duct atre sia, nail dysplasia, hypohidrosis, hypodontia or cleft palate [49] In addition, inner female genital dysplasias have been noticed [53]. Defects in transcription components other than p63 In addition to the p63 pathway, a number of other ectodermal dyspla sias have now been attributed to defects in transcription factors that control the expression of several target genes important in ectodermal morphogenesis [54]. In many circumstances, positional clon ing research have yielded the primary mutation in a specific gene however the detailed molecular signalling pathways have yet to be delineated. There is proof that the two ciliary proteins, Evc and Evc2, the products of human dis ease genes associated with the EvC syndrome, act downstream of smoothened to transduce sonic hedgehog signalling. A third baby had a milder phenotype with repeated infections as a end result of Staphylococcus aureus and Streptococcus pneumoniae, and three further siblings from a unique kindred had recurrent severe infections with S. Since these unique reviews, the disease phenotypic spectrum has been delineated and consists of severe lifethreatening or recurrent bacte rial infections within the decrease respiratory tract, pores and skin, delicate tissues, bones and gastrointestinal tract, in addition to meningitis and septicaemia in early childhood. Most patients have extreme hypogamma globulinaemia, with low serum IgG ranges and varied ranges of other immunoglobulin isotypes (IgA, IgM and IgE). Some patients have massively elevated IgM ranges, and an impaired antibody response to polysaccharides is essentially the most consistent function of this condition. It has been shown that the pathogenic mutation preferentially impairs the interplay with K63 and M1linked diUb, which correlates with its ubiqui tinbinding defect in vivo [5]. Genetics As ectodermal dysplasias are such a heterogeneous group of ailments, all inheritance patterns have been described includ ing autosomal recessive, autosomal dominant, Xlinked and mitochondrial. Environmental components Epigenetic factors appear to be necessary for the phenotypical expression of the illness. Often sufferers have comorbidity with inflammatory bowel disease and rheu matoid arthritis. The incidence has been assumed to be roughly 1 in 250 000 stay male births for the Xlinked kind. Sparse hair with hypotrichosis or complete alopecia, abnormal teeth with conical form or lacking teeth and sweating impairment, combined with recurrent infections, are the leading medical findings to make an early diagnosis. Associated illnesses Twentyfive per cent of sufferers have comorbidity with inflam matory bowel disease and rheumatoid arthritis. Early prognosis is crucial to avoid lifethreatening problems induced by hyperthermia and infections. Synonyms and inclusions � Ectodermal dysplasia 1 � Xlinked hypohidrotic/hair/toothtype ectodermal dysplasia � Xlinked anhidrotic ectodermal dysplasia � Christ�Siemens�Touraine syndrome Genetics the disease is usually inherited in an Xlinked recessive style. Hypohidrotic or anhi drotic ectodermal dysplasia is probably the most prevalent kind throughout the spectrum of ectodermal dysplasias. Clinical hallmarks are hypotrichosis on the scalp but in addition of the eyebrows and eye lashes, hyperpigmentation around the eyes, dry skin and peg shaped primary and secondary tooth with hypodontia (Table sixty seven. Affected individuals present heat intolerance with episodes of hyperpyrexia, which can lead to seizures and neurological damage [1]. Fever of unknown origin as a toddler and later heat intol erance are typical constellations. Missing teeth or malformed enamel are also characteristic and a clue for prognosis in youngsters. As mentioned, an autosomal dominant type of the illness may be distinguished on the idea of its mode of inheritance. The dysfunction is characterized by hypotrichosis with fine, slowgrowing scalp and body hair, sparse eyebrows, hypo hidrosis, nail anomalies and hypodontia. Complication Smooth, dry skin Sparse hair Sparse eyebrows Sparse physique hair Decreased sweating Heat intolerance Onychodysplasia Dental anomalies Adapted from Aswegan et al. Clinical options [1] History A history of warmth intolerance is attribute however not obligatory. There are parallel darkish bands of various lengths operating across the full width of the shaft. Scanning electron microscopy research have proven fol licular distortion, follicular ridging and distorted bulbs however these findings are nonspecific.
Cheap provera 5mg otcVegetating, pustular lesions in flexures have to be differentiated from continual infections or Hailey� Hailey disease (benign familial pemphigus). Vegetating plaques mimicking pemphigus vegetans might happen in IgA pemphigus and paraneoplastic pemphigus and the hyperkeratotic lesions of continual pemphigus vegetans may simulate cutaneous tumours. The Investigations Histopathology the earliest histological adjustments consist of intercellular oedema with lack of intercellular attachments within the basal layer. Suprabasal epidermal cells separate from the basal cells to kind clefts and blisters. Pemphigus erythematosus needs to be distinguished from each seborrhoeic dermatitis and persistent cutaneous lupus erythematosus. The superficial dermis has a mild, superficial, combined inflammatory infiltrate which will embrace eosinophils. Patients with generalized disease could require aggressive immunosuppression to suppress blistering and a major difficulty in managing these patients is attaining a balance between the dangers associated with highdose steroid remedy and those of poorly managed disease. IgG1 and IgG4 are the commonest subclasses; IgM and IgA are present less frequently than IgG. The use of a couple of substrate improves sensitivity, oesophageal mucosal substrates being preferable for the detection of antibodies to Dsg three [100] whereas normal human pores and skin reveals larger sensitivity for the detection of antibodies towards Dsg 1. Pemphiguslike circulating intercellular antibodies have been reported in circumstances corresponding to thermal burns [105], poisonous epidermal necrolysis [106] and in firstdegree family members of relations of pemphigus patients [107,108]. Azathioprine Azathioprine has been extensively used in the administration of pemphigus at a dose of 2�3 mg/kg/day and multiple case collection help its use. The combination of prednisolone and azathioprine is more effective than prednisolone alone both by means of mortality and remission [117]. One randomized controlled trial of pemphigus treatment discovered azathioprine to be the best steroid sparing agent, followed by cyclophosphamide (pulse therapy) and mycophenolate mofetil [118]. Another trial discovered azathioprine and mycophenolate mofetil to be equally efficient [119]. Potential adverse effects of azathioprine include bone marrow suppression, nausea and liver dysfunction and careful blood monitoring is due to this fact mandatory, particularly in the early levels of therapy. Management Because of the rarity of the pemphigus group of ailments, progress with informative randomized controlled trials has been slow. However, systemic corticosteroid remedy stays the mainstay of therapy, usually in combination with a steroidsparing immunosuppressant. Mycophenolate mofetil Mycophenolate mofetil (1�3 g/day) has been discovered helpful as a steroidsparing agent [119,121,122] in pemphigus. Mycophenolate mofetil is a prodrug of mycophenolic acid and has a relatively selective effect on T and B lymphocytes via its impact on the inhibition of inosine monophosphate dehydrogenase. A doubleblind randomized controlled research comparing azathioprine and mycophenolate confirmed no vital difference in efficacy between the two medication though there was a development in the course of fewer opposed results and more fast remission within the mycophenolate group [119]. Adverse results of mycophenolate embody bone marrow suppression and gastrointestinal symptoms and, as with azathioprine, patients require shut monitoring within the early phases of therapy. Gastrointestinal symptoms may respond to using entericcoated delayedrelease mycophenolic acid instead of mycophenolate mofetil. Topical remedy Patients who current with oral disease and mild cutaneous involvement may remain on this localized part for months. Potent topical or intralesional steroids could scale back the requirement for oral steroids. Cyclophosphamide Cyclophosphamide is a potent antiBcell agent with vital activity in pemphigus and other antibodymediated autoimmune illnesses [123,124]. Other therapies Although preliminary case stories have been suggestive of benefit of ciclosporin in pemphigus [141,142], more modern studies forged doubt on this [143]. Gold could have modest impact in pemphigus [145,146], though toxic effects limit its utility. Dapsone has been advocated as an adjunct in some sufferers with delicate disease [147] and a latest prospective, placebocontrolled research confirmed a modest steroid sparing effect [148]. Acetretin has been used in conjunction with prednisolone in pemphigus vegetans [149]. Tetracycline antibiotics with or with out nicotinamide could additionally be helpful as steroidsparing brokers in some sufferers [156,157].
Buy cheap provera 5mg lineLiver transplantation has been successfully used to remedy variegate porphyria (and acute intermittent porphyria) in cases Introduction, epidemiology and pathophysiology [1] the causes of pseudoporphyria are photosensitizing medication, haemodialysis and sunbeds. Other drugs reported to induce pseudoporphyria embody nalidixic acid, tetracyclines including minocycline, bumetanide, furosemide, isotretinoin and dapsone. Another situation in which pseudoporphyria is frequent is in patients with chronic renal failure present process haemodialysis (or less generally peritoneal dialysis). General concerns Clinical features of the porphyrias: common concerns Porphyria and the pores and skin three Takeshita K, Takajo T, Hirata H, et al. Erythropoietic protoprophyria � submicroscopic events through the acute photosensitivity flare. New sunscreens confer improved safety for photosensitive sufferers within the blue mild area. Erythropoietic uroporphyria associated with myeloid malignancy is likely distinct from autosomal recessive congenital erythropoietic porphyria. A management algorithm for congenital erythropoietic porphyria derived from a study of 29 circumstances. Porphyria cutanea tarda: clinical features and laboratory findings in 40 sufferers. Hemochromatosis genes and other components contributing to the pathogenesis of porphyria cutanea tarda. Increased frequency of the haemochromatosis Cys282Tyr mutation in sporadic porphyria cutanea tarda. Plasma ferritin levels as a guide to the treatment of porphyria cutanea tarda by venesection. A comparative examine of the outcomes of phlebotomy therapy and lowdose chloroquine remedy in porphyria cutanea tarda. Presentation the scientific features within the skin are indistinguishable from porphyria cutanea tarda [1]: vesicles, bullae, fragility, milia and scarring on uncovered pores and skin, notably the dorsal arms, but also the face, chest and occasionally different sites. It is preferable though not essential to determine a recognized explanation for pseudoporphyria in the patient. Other related illnesses also need to be excluded (epidermolysis bullosa acquisita, bullous pemphigoid, and so forth. Haemodialysis is related to increased plasma porphyrin concentrations anyway [4], and urine could additionally be unavailable to take a look at in these patients. It is important to attempt to differentiate the two diseases in renal failure, because of the implications regarding aetiological factors and treatment options. Management In druginduced and sunbedrelated pseudoporphyria, the important thing to administration is to take away the scary issue by stopping the relevant drug or sunbed usage. However, signs might proceed for several months after the discontinuation of a causative drug [6], and scarring persists. Dialysisrelated pseudoporphyria typically persists till renal transplantation removes the necessity for dialysis. Curative bone marrow transplantation in erythropoietic protoporphyria after reversal of extreme cholestasis. Hereditary coproporphyria in Germany: medical biochemical studies in fifty three patients. Detection of latent variegate porphyria by fluorescence emission spectroscopy of plasma. Lowdose hydroxychloroquine is as efficient as phlebotomy in therapy of sufferers with porphyria cutanea tarda. Acquired erythropoietic protoporphyria on account of myelodysplasia inflicting loss of chromosome 18. Protection from phototoxic injury throughout surgery and endoscopy in erythropoietic protoporphyria. Synonyms and inclusions � Cutaneous calcification � Calcinosis cutis � Subcutaneous calcification � Calcific arteriolopathy larger threat of autoimmune disease in women, related calcinosis can also be more frequent in ladies (male: female 1: 4 in one series [2]). Associated diseases Connective tissue ailments, notably dermatomyositis and scleroderma, but additionally lupus. Rarer associations include porphyria cutanea tarda, morphoea and lichen sclerosus.
Buy provera 5 mg visaThe mildest circumstances present in late childhood with dysarthria, dystonia and skeletal dysplasia (affecting the backbone and hip). Telangiectasia and intensive Mongolian blue spots have additionally been reported in childish instances. Patients normally current in early infancy with a hoarse cry, painful swollen joints and subcutaneous nodules. The most commonly affected joints are these of the hand and wrist, elbows, knees and ankles. The subcutaneous nodules could also be associated with erythematous papules and are generally close to affected joints and over strain factors, such because the occiput and decrease backbone. Histology reveals granulomas containing giant, foamy histiocytes; electron microscopy exhibits that these have cytoplasmic vacuoles containing curvilinear inclusions (Farber bodies) [17]. Most sufferers have psychomotor retardation, poor weight achieve and die in early childhood from respiratory infections. Introduction and common description this may be a uncommon Xlinked lysosomal storage dysfunction, characterized by angiokeratomas and multisystem issues [19]. Affected males usually present in childhood with episodes of pain within the extremities, adopted by the looks of angiokeratomas. Many heterozygous females also develop signs, though the onset is usually later. Pathophysiology A deficiency of galactosidase A prevents the degradation of glycosphingolipids with terminal galactose residues, predominantly globotriaosylceramide (Gb3). Gb3 accumulation in vascular endothelial, perithelial and clean muscle cells results in aneurysmal dilatation of blood vessels, ischaemia and infarction. Glycosphingolipids also accumulate within the renal glomeruli and tubules, cardiac muscle, autonomic ganglion cells and corneal epithelium. Investigations the prognosis is established by enzyme assays on leukocytes (or cultured cells). Niemann�Pick cells are typical examples � massive, often mononucleate histiocytes, whose cytoplasm is full of lipid droplets; they stain readily with Sudan stains and comprise doubly refractile materials. Ultrastructurally, the cytoplasm of Niemann� Pick cells accommodates granular lipid inclusions that may seem lamellar [15]. Ultrastructurally, Gaucher cells have vesicles that include twisted tubular structures [18]. Clinical options the first symptoms are often episodes of severe burning pain within the palms and soles (acroparesthesiae). These happen in 70�85% of male sufferers, usually beginning at between 5 and 15 years of age, though diagnosis is commonly delayed [21]. Acroparesthesiae occur in 50�70% of female sufferers, with a mean age of onset of 15 years [22]. Painful crises are sometimes triggered by fever or exertion and should final hours or days. Angiokeratoma corporis diffusum happens in 65�70% of male sufferers and 35�40% of female patients [21,22]. Lesions can also be discovered on the higher arms, around the border of the lips, around the nail folds and on the palms and soles � these are normally macular angiomas with minimal hyperkeratosis. In girls, lesions are most frequent on the trunk and proximal limbs; genital lesions are rare. Telangiectases are present in 23% of male patients and 9% of female sufferers, often on the lips, buccal mucosa, ears or conjunctiva [23]. Anhidrosis or hypohidrosis happens in 53% of male sufferers and 28% of female sufferers, normally starting within the third decade [23]. Miglustat is an oral drug that decreases the buildup of glucocerebroside by lowering the synthesis of glycosphingolipids (substrate reduction therapy) [12]. Without enzyme alternative remedy, endstage renal failure is usually reached between forty and 50 years of age [21].
Purchase provera cheap onlineThe first begins after a quantity of days or perhaps weeks and lasts a few month, involving spontaneous burning and stinging, or tearing or taking pictures, pain, precipitated by mechanical stimuli corresponding to bathing, clothing on the skin or draughts [7]. Symptoms relate to sympathetic hyperactivity and embrace cool, oedematous pores and skin, hyperhidrosis and cyanosis, or livedolike modifications. Nails might present decreased or elevated progress or thickening, turn into brittle or develop striations. Stage three, beginning around 8 months after harm, involves progressive tissue harm, which might become permanent. The adjustments may be as a result of vasoconstriction (resulting in skin hypoxia) or decreased motion of the pores and skin from inactivity of underlying joints, tendons or ligaments. If the ache is worsened by bodily stimuli, the patient could protect the limb resulting in trophic modifications in the bone, muscle and pores and skin (Sudeck atrophy). Bone scintigraphy using threephase bone scans may usefully identify early adjustments. Other tests embrace: ache reduction on 1adrenergic blockade with intravenous phentolamine; pain exacerbation on 2 stimulation by clonidine; and severe ache on cold stimulation. These include the presence of allodynia and/or hyperalgesia; temperature asymmetry and/or skin color changes/asymmetry; oedema and/or sweating changes/asymmetry; and decreased vary of movement and/or motor dysfunction (weakness, tremor, dystonia) and/or trophic adjustments [5,8]. Pragmatically, encouragement of light limb use and lively life-style is recommended [8]. Psychological interventions, together with biofeedback, cognitive behavioural and rest strategies are crucial, though usually missed. Primary aims are to reduce pain, to protect or restore operate, and to enable patients to handle their situation [8]. Patients ready to see a pain specialist ought to be seen often and be suggested about the usage of simple analgesics. Pathophysiology the sympathetic fibres supplying the facial skin travel from the hypothalamus via the spinal twine, to relay on the stage of the primary and second thoracic segments in the lateral column of the spinal grey matter. Preganglionic fibres emerge from the primary and second thoracic spinal nerves, and cross up the cervical sympathetic chain to relay within the superior cervical ganglion. From here, postganglionic fibres pass to provide the eye and the skin of a small central space of the face through the interior carotid sympathetic plexus. Other fibres pass alongside the exterior carotid artery and its branches to innervate most of the facial pores and skin with vasomotor and sudomotor fibres. This pathway could be interrupted centrally within the spinal wire, for instance by medullary infarction, syringomyelia, multiple sclerosis or intraspinal tumours. The peripheral fibres may be broken by aortic aneurysm, cervical lymphadenopathy, surgery, regional anaesthetic procedures or tumours. Horner syndrome could follow sympathectomy for the remedy of palmar and axillary hyperhidrosis, and happens in up to 40% of sufferers after open cervical sympathectomy, and 8% of these having transthoracic endoscopic sympathectomy [2]. In such cases, there could also be decision of longstanding pompholyxtype hand eczema ipsilaterally, suggesting a neurological pathogenesis for endogenous pompholyx in some patients [3,4]. Gustatory sweating is localized to certain areas, together with the scalp, higher lip, perioral area and sternum. It can occur following damage to the sympathetic cervical trunk, the vagus nerve or the auriculotemporal nerve [1]. Clinical options Horner syndrome is usually present in adults and solely rarely in children, the place it can be either congenital or acquired [1]. An irritative phase occurs rarely at the outset of Horner syndrome, characterized by transient unilateral hyperhidrosis and vasoconstriction. The paralytic phase involves drooping of the eyelid (ptosis) with narrowing of the palpebral fissure. The pupil is small, however shows normal reflex constriction to mild and accommodation. Sweat glands on the medial and lateral elements of the brow are innervated separately, the previous by fibres from the sympathetic plexus of the internal carotid, and the latter from the plexus surrounding the exterior carotid [5]. This explains the findings in Raeder syndrome, where harm involving the perivascular plexus of the interior carotid results in anhidrosis solely medially on the forehead [6]. Three circumstances of bilateral Horner syndrome, and three instances of contralateral Horner syndrome have been reported [7�10]. Pathophysiology Gustatory hyperhidrosis might complicate surgery involving the parotid gland or the temporomandibular joint.
|