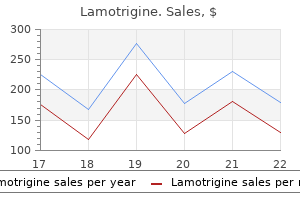
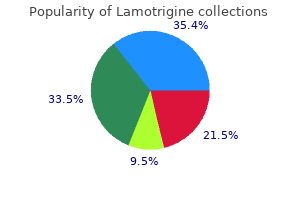
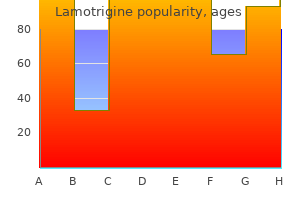
|
Lamotrigine dosages: 200 mg, 100 mg, 50 mg, 25 mg
Lamotrigine packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Best purchase lamotrigineSystemic poisoning with atropine or with medication which have atropinic qualities, particularly the tricyclic anti depressants, is characterized by extensive dilatation and fix ity of the pupils. Hippus, or fluctuating pupillary dimension, is occasionally characteristic of metabolic encephalopathy. A unilaterally enlarged pupil is an early indicator these are altered in a selection of methods in coma. In gentle coma of metabolic origin, the eyes rove conjugately from aspect to side in seemingly random trend, generally resting briefly in an eccentric position. These movements disappear as coma deepens, and the eyes then remain immobile and slightly exotropic. A lateral and slight downward deviation of one eye suggests the presence of a third-nerve palsy, and a medial deviation, a sixth-nerve palsy. During a focal seizure the eyes turn or jerk towards the convuls ing aspect (opposite to the irritative focus). The globes flip down and inward (looking on the nose) with hematomas or ischemic lesions of the thalamus and higher midbrain (a variant of Parinaud syndrome). Abducens palsy is indicated by an esotropic resting place and an absence of outward deviation of one eye with the reflex maneuvers. The full absence of ocular motion in response to oculovestibular testing indicates a extreme disruption of brainstem tegmental techniques in the pons or midbrain or, as already mentioned, a profound overdose of sedative, anesthetic, or anticonvulsant drugs. A reduction in the frequency and eventual loss of spontaneous blinking, then a lack of response to touching the eyelashes, and, finally, a scarcity of response to corneal touch (the corneal reflex afferent limb travels within the tri geminal nerve and efferent limb, facial nerve) are among the most reliable indicators of deepening coma. A marked asymmetry in corneal responses signifies either an acute lesion of the opposite hemisphere or, much less often, an ipsilat eral lesion in the brainstem. Abduction actions (away from the midline) to escape a noxious stimulus have the same significance and differentiate a motor response from posturing, described under. Focal motor epilepsy indicates that the corticospinal pathway to the convulsing aspect is intact. With large destruc tion of a cerebral hemisphere, as occurs in hypertensive hemorrhage or internal carotid-middle cerebral artery occlusion, seizure activity could additionally be manifest solely in the ipsilateral limbs, the contralateral limbs being prevented from collaborating by the hemiplegia. Elaborate forms of semivoluntary motion may be manifest on the non hemiparetic side in patients with extensive disease in a single hemisphere; they probably represent some sort of disin hibition of cortical and subcortical motion patterns. The response in coma of metabolic origin or that brought on by bihemispheric struc tural lesions consists of conjugate motion of the eyes in the other way. Elicitation of these ocular reflexes in a comatose patient provides two pieces of knowledge: (1) proof of unimpeded function of the midbrain and pontine tegmental structures that integrate ocular move ments and of the oculomotor nerves, and (2) loss of the cortical inhibition that normally holds these movements in check. There must as an alternative be widespread cerebral dysfunction, similar to occurs after anoxia or with metabolic-toxic suppression of corti cal neuronal exercise. It should be conceded, however, that sedative or anticonvulsant intoxication profound enough to cause coma may obliterate the brainstem mechanisms for oculocephalic reactions and, in excessive instances, even the vestibular-ocular (caloric) responses as noted under. Asymmetry of the elicited eye movements remains a dependable sign of focal brainstem disease. In situations of coma caused by a big mass in a single cerebral hemisphere that secondarily compresses the higher brainstem, the oculocephalic reflexes are normally present, but the move ment of the attention on the side of the mass could additionally be impeded in adduction on account of a compressive third-nerve paresis. Irrigation of one ear with 10 mL of chilly water (or room-temperature water if the affected person is arousable) causes sluggish conjugate deviation of the eyes toward the irrigated ear, adopted in a few seconds by compensatory nystagmus (fast part away from the stimulated side). In coma tose sufferers, the quick "corrective" phase of nystagmus is misplaced and the eyes are tonically deflected to the side irrigated with chilly water or away from the side irrigated with heat water; this position could additionally be held for ful in localizing the cause for coma. This postural pat tern was first described by Sherrington, who produced it in cats and monkeys by transecting the brainstem at the intercollicular level. Decerebrate posture was noted in animals to be ipsilateral to a one-sided lesion, hence not a results of involvement of the corticospinal tracts; the opposite is true in humans. Patients with an acute lesion of 1 cerebral hemisphere might present an analogous type of extensor postur ing of the contralateral and generally ipsilateral limbs, and this may coexist with the power to make purposeful movements of the identical limb. Another associated pattern consists of extensor posturing of an arm and leg on one aspect, and flexion and abduction of the other arm. In some sufferers with the extensor postural adjustments the lesion is clearly in the cerebral white matter or basal ganglia, which is difficult to reconcile with the clas sic physiologic explanation for decerebrate posturing. Decerebrate posturing, both in experimental prepara tions or in humans, is usually not a persistent state.
Lamotrigine 50mg for saleThis is especially obvious within the dis cussion of the anatomy of advanced cognitive properties corresponding to intelligence, as described in Chap. Thus, many primary functions are anchored in one cortical region and a lesion there causes lack of a selected capacity. These features of cerebral localization-brought out so clearly in the writings of Wernicke, Dejerine, and Liepmann, have been elaborated by Luria (1966 and 1969) and the Russian college of physiologists and psy chologists and prolonged by Geschwind (1965). In maintaining with the mannequin of interconnected networks, they viewed perform not as the direct property of a selected, extremely specialized area of the cerebrum however because the product of complicated, diffusely distributed exercise by which sensory stimuli are analyzed and built-in at various levels of the nervous system and then united, through a system of quickly acquired connections, into a working mosaic adapted to accomplish a particular task To some extent, this model has been corroborated by practical imaging studies, which present increased metabolic activity in sev eral cortical areas throughout almost every form of human conduct, together with willed motor acts, language tasks, and those coinciding with perceptive and apperceptive sensory experiences. Within such a functional system, the preliminary and last points (the task and the effect) stay unchanged, but the intermediate links (the means of efficiency of a given task) may be modified within broad limits and will by no means be precisely the identical on two consecutive events. Thus, when a sure act is identified as for by a spoken command, the dominant temporal lobe should receive the message and transmit it to the premo tor areas. Or it might be initiated by the intention of the individual, by which case the first measurable cerebral activity (a "readiness potential") happens anterior to the premotor cortex. The motor cortex can be at all times under the dynamic management of the proprioceptive, visual, and vestibular methods. Thus, a lesion that affects any certainly one of several components within the act could trigger loss of a skilled ability, either the motor facilities themselves or their con nections with the opposite parts. Another theoretical scheme of cerebral perform identifies cortices of comparable total structure and divides the cerebral mantle into three longitudinally oriented zones, the triune mind articulated by Paul Maclean. A central vegetative neuronal system (allocortex and hypothalamus) supplies the mechanisms for all internal functions, the milieu interieur of Bernard and Cannon. This ostensibly metaphoric idea of central nervous sys tem perform, first proposed by Broca, was elaborated by Yakovlev and has been adopted more lately by Benson and by Mesulam (1998). Such a model retains to a large degree the cytoarchitectural similarities amongst areas that serve similar capabilities. In this manner, localization could also be considered because the product of genetic patterns of structure, which mature throughout development, and their synaptic formations, which per mit the event of complicated circuits throughout lifelong learning and experience. From these remarks, it follows that subdivision of the cerebrum into frontal, temporal, parietal, and occipital lobes is considerably of an abstraction in terms of land marks and cerebral function. Some of these delineations had been made lengthy before our first glimmer of know ledge about the perform of the cerebrum. Invariably, an ensemble of areas, a "network" of the variability described earlier, is activated to perform even seemingly easy tasks such as recalling a name, visualizing or figuring out an object, or finishing up a commanded task. Also, the cortex has been proven to differ in its various parts by virtue of connections with different areas of the cortex and with the thalamic nuclei and other decrease centers. Hence, one should regard the cortex as a heterogeneous array of many anatomic systems, every with extremely organized intercortical and dience phalic connections. Unfolded, it has a surface extent of about 4,000 cm2, concerning the measurement of a full sheet of newsprint (right and left pages). Contained in the cortex are many billions of neurons (estimated at 10 to 30 billion) and 5 instances this variety of support ing glial cells. Because nerve cells look alike and presumably perform alike, the remarkable variety in human intelligence, retailer of information, and behavior should depend on the potential for nearly infinite varia tions in neuronal interconnectivity. Most of the human cerebral cortex is phyloge netically recent, hence the time period neocortex. Approximate distribution of functional zones on lateral (A) and medial (B) aspects of the cerebral cortex. These latter features distinguish the neocortex from the older and less uni kind allocortex ("different cortex"), which contains mainly the hippocampus and olfactory cortex. Two cell types-relatively large pyramidal cells and smaller, more numerous rounded (granular) cells-predominate within the neocortex, and varia tions in its lamination are largely decided by variations in the measurement and density of these neuronal sorts. Many variations in lamination have been described by cortical mapmakers, however two major types of neocortex are recognized: (1) the homol:t pical cortex, during which the j six-layered arrangement is quickly discerned, and (2) the heterotypical cortex, in which the layers are less distinct. The precentral cortex (Brodmann areas four and 6, mainly motor region) is domi nated by pyramidal quite than granular cells, especially in layer V (hence the time period agranular). Beyond these morphologic distinctions, the intrinsic organization of the neocortex follows a pattern elucidated by Lorente de N6. He described vertical chains of neu rons arranged in cylindrical modules or col umns, each containing 100 to 300 neurons and closely interconnected up and down between cortical layers and to a lesser extent, horizontally. Their impulses are then transmitted by internuncial neurons (intemeurons) to adjoining superficial and deep layers and then to acceptable efferent neurons in layer V.
Syndromes - Biliary stricture
- Stiff neck
- Weakness
- Blurred vision
- Fatigue
- Hospital cafeterias
- Trichloroethane
Lamotrigine 50mg genericIt is necessary to grasp the digit at the sides, perpendicular to the aircraft of transfer ment; otherwise the stress utilized by the examiner may allow the affected person to identify the course of move ment. The affected person ought to be instructed to report each motion as being "up" or "down" from the earlier position (directional kinesthesia). It is useful to show the take a look at with a large and easily recognized motion, however as soon as the idea is evident to the affected person, the smallest detectable modifications should be determined. Normally, a really slight diploma of motion is appreciated within the digits (as little as 1 diploma of an arc). The test must be repeated enough instances to get rid of probability (50 p.c of responses). Defective perception of passive move ment is judged by comparability with a normal limb or, if notion is bilaterally defective, on the idea of what the examiner has discovered via experience to be normal. Slight impairment may be disclosed by a slow ness of response or, if the digit is displaced very slowly, by an unawareness or uncertainty that movement has occurred; or, after the digit has been displaced in the same course several times, the affected person could misjudge the first movement in the opposite direction; or, after the examiner has moved the toe, the affected person may make a quantity of small voluntary movements of the toe in an apparent try to decide its place or the direc tion of the motion. The lack of position sense in the legs can additionally be demonstrated by displacing the limb from its authentic place and having the affected person, with eyes closed, place the other leg in the same place or point to the nice toe. If proprioception if abnormal in axial constructions, the affected person will be unable to preserve his steadiness with feet collectively and eyes closed (Romberg sign). In the Romberg place, even a standard person whose eyes are closed will sway barely, and the affected person who lacks steadiness because of cerebellar ataxia or another motor dysfunction will sway significantly extra if his visible cues are removed. Only a marked discrepancy in stability with eyes open and with eyes closed qualifies as a Romberg sign. The most sure indication of abnormality is the necessity to step to the facet or backward to avoid falling. Mild degrees of unsteadiness in an anxious or suggestible patient could also be overcome by diverting his attention. Patients with authentic proprioceptive problems will sway when there gaze is diverted from the ground and then become more unsteady when the eyes are closed. Patient with facti tious unsteadiness, usually will stay secure after they have a look at the ceiling or a distant object after which become very unsteady when the eyes are closed. Testing of Vibratory Sense this is a composite sensation comprising touch and rapid alterations of deep-pressure sense. The only cutaneous structure capable of registering such stimuli of this fre quency is the quickly adapting pacinian corpuscle. The conduction of vibratory sense depends on each cutane ous and deep afferent fibers that are carried in the muscle spindle afferent fibers and ascend primarily within the dorsal columns of the cord. Vibration and place sense are usually impaired in related situations, although considered one of them (most usually vibration sense) may be affected disproportionately. With advancing age, vibra tion is the feeling most commonly diminished, espe cially on the toes and ankles (see further on). As with thermal and ache testing, there are mechani cal units that quantitate vibration sense. The examiner might detect the vibration after it ceases for the affected person by holding a finger under the distal interpha langeal joint, the deal with of the tuning fork being placed on the dorsal side of the joint. Or the vibrating fork is allowed to run down till the moment that vibration is now not perceived, at which level the fork is transferred rapidly to the corresponding a part of the examiner and the time to extinction is noted. There is a small diploma of accommodation to the vibration stimulus, so that slight asymmetries detected by speedy shifting from a body part on one side to the opposite must be interpreted accord ingly. The notion of vibration at the patella after it has disappeared at the ankle or at the anterior iliac spine after it has disappeared on the knee is indicative of a size dependent peripheral neuropathy. The approximate degree of pinprick loss from a spinal wire lesion can be corrobo rated by testing vibratory sensation over the iliac crests and successive dorsal vertebral spines. Lesions in these constructions often disturb advanced sensory perception but leave the primary modalities (touch, ache, temperature, and vibration sense) relatively little affected. If a cerebral lesion is suspected, discriminative function should be examined further in the following methods.
Buy 25mg lamotrigine fast deliveryThe massive motor items take part primarily in phasic actions, that are characterised by an preliminary burst of activity in the agonist muscle tissue, then a burst within the antagonists, followed by a third smaller burst in the agonists. The basal ganglia and cerebellum set the sample and timing of the muscle motion in any projected motor performance. In help of the body in an upright posture, when the legs must act as rigid pillars, and in shivering, agonists and antagonists contract simultaneously. Locomotion requires that the extensor pattern of reflex standing be inhibited and that the coordinated pattern of alternating stepping actions be substituted; the latter is accom plished by multisegmental spinal and brainstem reflexes, the so-called locomotor facilities. Suprasegmental management of the axial and proximal limb musculature (antigrav ity postural mechanisms) is mediated primarily by the reticulospinal and vestibulospinal tracts and manipula tory movements of the distal extremity muscle tissue, by the rubrospinal and corticospinal tracts. Muscle stretch (tendon) reflex activity and muscle tone depend on the status of the large motor neurons of the anterior horn (the alpha motor neurons), the muscle spindles and their afferent fibers, and the small anterior horn cells (gamma neurons), whose axons terminate on the small intrafusal muscle fibers throughout the spindles. Each anterior horn cell has on its floor membrane roughly 10,000 receptive synaptic terminals. Some of those terminals are excitatory, others inhibitory; in combination, they determine the activity of the neuron. Some of the gamma motor neurons are tonically energetic at rest, maintain ing the intrafusal (nuclear chain) muscle fibers taut and delicate to energetic and passive changes in muscle length. A faucet on a tendon stretches or perhaps causes vibra tion of the spindle and prompts its nuclear bag fibers. Afferent projections from these fibers synapse directly with alpha motor neurons in the same and adjoining spinal segments; these neurons, in flip, send impulses to the skeletal muscle fibers, resulting in the famil iar monosynaptic muscle contraction or monophasic (myotatic) stretch reflex, generally referred to because the tendon reflex or "tendon jerk". The alpha neurons of antagonist muscles are concurrently inhib ited but via disynaptic quite than monosynaptic connections. This is accomplished partly by inhibitory interneurons (reciprocal inhibition), which additionally obtain input from descending pathways. Renshaw cells also take part by offering negative suggestions by way of inhibitory synapses of alpha motor neurons (recurren t inhibition). Thus the setting of the spindle fibers and the state of excitability of the alpha and gamma neurons (influenced greatly by descending fiber systems) determine the extent of activity of the tendon reflexes and muscle tone (the responsiveness of muscle to stretch). Other mechanisms, of an inhibitory nature, contain the Golgi tendon organs, for which the stimulus is pressure produced by energetic contraction of muscle. These encapsulated receptors, which lie within the tendinous and aponeurotic insertions of muscle, activate afferent fibers that finish on internuncial cells, which, in turn, project to alpha motor neurons, thus forming a disynaptic reflex arc. Golgi tendon receptors are silent in relaxed muscle and through passive stretch; they serve, together with muscle spindles, to monitor or calibrate the length and pressure of muscle contraction beneath different situations. They additionally play a task in naturally occurring limb actions, significantly in locomotion. The alpha motor neurons of the medial components of the anterior horn provide trunk or axial muscular tissues, and neurons of the lateral components supply the appendicular muscular tissues. Smaller ante rior horn cells innervate small muscles and control more delicate movements, notably those within the fingers and hand. All the facilita tory and inhibitory influences equipped by cutaneous and proprioceptive afferent and descending suprasegmental neurons are coordinated at segmental ranges. For further details the reader may consult Burke and Lance and likewise Davidoff (1992). The massive neurons of the anterior horns of the spinal cord comprise excessive concentra tions of choline acetyltransferase and use acetylcholine as their transmitter on the neuromuscular junction. The main neurotransmitters of the descending corticospinal tract, in as far as may be decided in humans, are aspartate and glutamate. Glycine is the neurotransmitter released by Renshaw cells, that are responsible for recurrent inhibition, and by interneurons that mediate reciprocal inhibition during reflex motion. L-glutamate and L-aspartate are launched by primary afferent terminals and interneurons and act particularly on excitatory amino acid receptors. Sensory fibers of the femoral nerve (spinal segments L2 and L3) mediate this myotatic reflex. The principal receptors are the muscle spindles, which respond to brisk stretching of the muscle effected by tapping the patellar tendon. In this monosynaptic reflex, afferent fibers entering spinal segments L2 and L3 and efferent fibers issuing from the anterior horn cells of these and lower ranges complete the reflex arc. Motor fibers shown leaving the 52 spinal section and passing to the hamstring muscle tissue show the clisynaptic pathway by which inhibi tory influences are exerted upon an antagonistic muscle group in the course of the reflex. Contractions of the intrafusal fibers in the polar parts of the spindle stretch the nuclear bag area and thus cause an afferent impulse to be conducted centrally.
Purchase 100mg lamotrigine with visaThe prognosis is confirmed when the pain is relieved for a vari able period by injection of the joint with local anesthetic. Often one is unsure whether it was the analgesic effect on the joint or the infiltration of the region around the nerve root that relieved the pain. Two controlled studies have offered evidence of the inefficacy, both within the quick and long term, of corticosteroid injections into the facet joints (Carette et al, 1991; Lilius et al). Some sufferers have discovered that they might get hold of short-term aid from aspect ache by forcefully twisting or stretching the back and creating an audible pop on the affected joint, corresponding to chiropractic manipulation. Over time, they purchase a laxity of the supporting constructions of the joint, which can actually perpetuate the problem. If the analysis is established by native injection, pain facilities provide radiofrequency ablation of the small recur hire sensory nerves that innervate the j oint as a means of everlasting relief. Some writers have used the term side syndrome to describe a painful state from facetal hypertrophy that gives rise to a lumbar monoradiculopathy indistinguish ready from that caused by a ruptured disc or spondylosis. At operation, the spinal root is compressed in opposition to the floor of the intervertebral canal by overgrowth of an infe rior or superior aspect. Foraminotomy and facetectomy, after exploration of the root from the dural sac to the pedicle, have relieved the pain in many operated cases. At first, the signs are obscure (tired again, "catches" up and down the again, sore back), and the diagnosis may be overlooked for many years. Although the ache is recurrent, limitation of move ment is fixed and progressive and comes to dominate the scientific picture. In superior phases, a cauda equina compression syndrome might compli inflammatory response and proliferation of connective tissue (Matthews). Limitation of chest growth, tender ness over the sternum, decreased movement and tendency to progressive flexion of the hips, and the characteristic immobility and flexion deformity of the backbone ("poker spine") may be present early in the course of the illness. The radiologic hallmarks are destruction and sub sequent obliteration of the sacroiliac joints, adopted by bony bridging of the vertebral our bodies to produce the characteristic "bamboo backbone. The time period is also applied to thickening of the arachnoidal sheaths round roots (normal roots have primarily no epineurium). Axial T2-weighted picture on the L3 vertebral degree showing lateral displacement of nerve roots by acquired arachnoid cysts. The great risk in this disease is fracture dislocation of the backbone from comparatively minor trauma, significantly flexion extension injuries. Occasionally, ankylosing spondylitis is complicated by harmful vertebral lesions. This complication ought to be suspected every time the pain returns after a period of quiescence or becomes localized. The main lesion could additionally be small and asymp tomatic, and the first manifestation of the tumor could additionally be ache in the back attributable to metastatic deposits. A fracture of a vertebral physique in an otherwise healthy young or middle-aged individual ought to alert the doctor to the potential for an underlying metastasis. At the time of onset of the back pain, there may be no radiographic modifications on plain radiographs; when such adjustments do appear, they usually take the form of damaging lesions in one or several vertebral bodies with little or no involvement of the disc space, even in the face of a com pression fracture. Infection of the vertebral col umn, osteomyelitis, is usu ally caused by staphylococci and less typically by coliforms and mycobacteria. The affected person complains of subacute or persistent ache within the again, which is exacerbated by move ment however not materially relieved by rest. A paravertebral mass is commonly found, indicating an abscess, which can, within the case of tuberculosis, drain spontaneously at sites fairly distant from the vertebral column. The again pain tends to replicate the tempor charac teristics of the ache from the affected organ;. Diseases of the pancreas are apt to trigger pain within the again, being more to the best of the spine if the pinnacle of the pancreas is involved and to the left if the physique and tail are implicated. A tumor in the iliopsoas area typically produces a urillateral lumbar ache with radia tion toward the groin and labia or testicle; there can also be indicators of involvement of the higher lumbar pinal roo. An aneurysm of the stomach aorta may mduce pam localized to a similar area of the spine.
Cheap lamotrigine 25 mg with amexToday, the vaginal wall is cleaned just before surgery with Betadine after the bladder is catheterized. If spinal or epidural anaesthesia is employed, the lady may not be able to micturate as such and bladder catheter for twenty-four h postoperatively turns into essential. In prolapse, if infection or a decubitus ulcer is current, vaginal packing with Betadine for a couple of days heals the ulcer. Most girls are actually admitted early on the day of the operation, and this saves the price. Only these at excessive risk or with a medical disorder get admitted at some point prior to surgery. Anaesthesia It is left to the selection of the anaesthetist, and this partly depends upon the condition of the woman. The abdominal dressing must be modified on the third day and when the sutures are removed. Following a minor surgery, oral fluids are allowed 4 h after the surgery, and soft food regimen is given on the day of surgical procedure. The woman needs counselling relating to way of life, sexual exercise and any particular precaution. A girl operated for cancer needs extended chemotherapy and radiotherapy and ought to be beneath statement for recurrence. Analgesics are required for a day or two, and the choice relies upon upon the need of the girl. The affected person must be observed for respiratory problems and pain within the legs (thrombosis). Urine tradition should be obtained if the indwelling catheter is positioned for 2 days or more. A slight bleeding is noted during the first few days, and this wears off steadily. If postoperative haemoglobin falls beneath eight g%, iron remedy will restore it to normal. It ought to be famous that one unit of blood raises haemoglobin by just 1 g, with its other related dangers of blood transfusion. Pelvic vein thrombosis with fever and tachycardia is less frequent with early ambulation and prophylactic antibiotics. It is especially a diagnostic process, not often accomplished for therapeutic purpose (mainly obstetric). To stop cervical stenosis following Manchester operation for prolapse of the uterus. To prevent postoperative cervical stenosis in cauterization of cervical erosion and conization. Obstetric indications are: Prior to evacuation in missed abortion, incomplete abortion, evacuation of hydatidiform mole. Until recently, D&C was performed premenstrually to detect if ovulation has occurred. Corpus luteal phase defect is recognized when the endometrial histology lags behind the menstrual date by 2 days. A menopausal woman on hormonal alternative remedy; she must be watched for endometrial hyperplasia and cancer. A woman on tamoxifen for breast cancer ought to undergo curettage 6-monthly to diagnose endometrial hyperplasia and cancer. Karman plastic curette is especially used for suction evacuation in medical termination of first-trimester pregnancy. Slow cervical dilatation is performed with prostaglandin E1 (misoprostol) vaginal pessary (200�400 �g). The pessary is inserted within the vagina three h prior to D&C, and this slow dilatation avoids cervical trauma. Local anaesthesia is enough in a multiparous girl, however a nulliparous or an apprehensive girl may require general anaesthesia. The perineal area and inside thigh space and vagina are cleaned with Savlon or Betadine. Bimanual examination is completed to ascertain the dimensions of the uterus and its direction and to rule out adnexal mass.
Purple Pitcher Plant (Pitcher Plant). Lamotrigine. - Digestive disorders, constipation, urinary tract diseases, fluid retention, preventing scar formation, pain, and other conditions.
- Are there safety concerns?
- What is Pitcher Plant?
- How does Pitcher Plant work?
- Dosing considerations for Pitcher Plant.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96145
Order lamotrigine 200mg overnight deliveryIt may be noticed in certain types of muscular dystrophy by which the distal musculature of the limbs is concerned. A specific disorder of gait, additionally of peripheral origin and resembling steppage gait, could additionally be noticed in patients with painful dysesthesias of the soles of the feet. Because of the exquisite ache evoked by tactile stimulation of the feet, the patient treads gingerly, as though walking bare foot on hot sand or pavement, with the ft rotated in such a method as to limit contact with their most painful parts. The usual trigger is likely considered one of the painful peripheral neuropa thies (most often alcoholic-nutritional but in addition toxic and amyloid types), causalgia, or erythromelalgia. This disorder of gait is also seen in a big selection of chronic spinal twine diseases involving the dorsolateral and ventral tracts, most frequently multiple sclerosis, but additionally including syringomyelia, any kind of continual meningomyelitis, subacute mixed system disease of both the pernicious anemia and nonpernicious anemia varieties, spinal twine compression or traumatic injury, adrenomyeloneuropathy, and familial forms of results of posterior col umn illness are added, giving rise to a combined gait disturbance-a spinal spastic ataxia, characteristic of a quantity of sclerosis and sure spinal cord degenerations similar to Friedreich ataxia. Frequently in these illnesses, the Parki nsonian and Festinati ng Gait Diminished or absent arm swing, ahead bent torso, brief or shuffling steps, turning en bloc, hesitation in beginning to stroll, shuffling, or "freezing" when encounter ing doorways or different obstacles are the options of the parkinsonian gait. The steps are brief, and the feet barely clear the bottom as the affected person shuffles along. Once walking has started, the higher a part of the physique advances ahead of the lower half, and the affected person is impelled to take more and more quick and speedy steps as though trying to catch up to his center of gravity. The steps become more and more fast, and the patient might simply break right into a trot and collide with an obstacle or fall if not assisted. The leg tends to rotate outward to describe a semicircle, first away from and then towards the trunk (circumduction). The foot scrapes the ground, contact being made by the toe and outer sole of the foot. One can recognize a spastic gait by the sound of slow, rhythmic scuffing of the foot and carrying of the medial toe of the shoe. This sort of gait disorder is most often a sequela of stroke or trauma but might result from any situation that damages the cor ticospinal pathway on one facet. The spastic paraplegic or paraparetic gait is, in effect, a bilateral hemiplegic gait. Each leg is superior slowly and stiffly, with restricted movement at the hips and knees. The legs are extended or barely bent on the knees and the thighs could also be strongly adducted, causing the legs nearly to cross because the affected person walks (scissor-like gait). The steps are regular and brief and the affected person advances only with great effort as though wading waist-deep in water. The defect is in stiffness of the stepping mechanism and in propulsion, not in assist or equilibrium. A spastic paraparetic gait is the main manifestation of cerebral diplegia (Little disease, a type of cerebral festinare, "to hasten," and appropriately describes the involuntary acceleration or hastening that characterizes the gait of patients with Parkinson disease. Festination could additionally be obvious when the affected person is walking ahead or ing the legs shortly sufficient to overtake the center of gravity. The defects are in rocking the body from facet to facet, so that the feet can clear the ground, and in mov postural assist reflexes, demonstrable in the standing affected person by falling in response to a push against the ster num or a tug backward on the shoulder. A regular particular person readily retains his stability or adjusts to modest displace ment of the trunk with a single step, but the parkinsonian patient could lean backward with the upper torso and then stagger or fall unless someone stands by to prevent it. Quite often, one encounters an elderly patient with solely the instability and freezing parts of the parkinsonian gait dysfunction, so-called lower-half parkin sonism. The basis is then most likely a particular isolated frontal lobe degeneration (see additional on). Within a few years, as identified by Factor and colleagues in their two papers, the affected person is usually reduced to a chair-bound state. Other very unusual gaits are generally noticed in Parkinson illness and have been particularly distinguished within the postencephalitic kind, which is now practically extinct. For example, such a patient may be unable to take a step forward or does so only after he takes a few hops or one or two steps backward (aptly mimicked by the Monty Python troupe in their skit, "Ministry of Silly Walks"). Or walking could also be initiated by a series of quick steps or a sequence of steps of increasing dimension. In the more superior stages, walking turns into impossible owing to torsion of the trunk or the continual flexion of the legs. Kyphosis due to spinal defor mities does the same and all of these situations trigger the patient to walk while trying at the floor beneath the feet, but they hardly ever trigger falling. Chapter four extra fully describes the general features of the gaits of choreoathetosis and dystonia.
Buy lamotrigine with a mastercardAmong the particular modules of reminiscence, the notion of a working reminiscence has each clini cal and neuropsychologic credibility. Several areas of the brain have to be active throughout tasks of working memory, together with the hippocampi and dorsal thalamus, however lesions of the dorsolateral prefrontal cortex most particularly impair the skill. The unique work of Goldman-Rakic could additionally be referred to for dialogue of the mechanisms that underlie working memory. Finally, there are causes, primarily based mainly on the neuro anatomic and practical imaging research mentioned later, to view episodic memory for spatial and topographic info in a specific way. Certainly the recollec tion of personally skilled events could be dissociated to a point from the memory of the topographic association of the scene during which these memories were fashioned, however often these two components are inextricably certain in one expertise. Observations of human illness have confirmed the fundamental importance of the diencephalic-hippocampal constructions in all reminiscence operate. The difficulty of evalu ating memory perform in monkeys has been largely over come by use of the "delayed nonmatching-to-sample task," which is essentially a refined check of recognition reminiscence and is impaired both in patients with the amnesic syndrome and in monkeys with lesions of the mediodorsal nuclei of the thalamus and inferomedial temporal cortical areas (Mishkin and Delacour). Using this technique and various other others that simulate a restricted type of human amnesia, Zola-Morgan and colleagues have proven that bilateral lesions of the hippocampal formation cause a permanent impairment of reminiscence perform. However, lesions that had been restricted to the perirhinal and entorhinal cortex (Brodmann areas 35 and 36) and the carefully related parahippocampal cortex did trigger a persistent reminiscence defect, presumably cortical information to the hippocampus. Lesions of the anteromedial components of the diencephalon, which receive and ship fibers to the amygdala and hippocampus, similarly abolished reminiscence perform. Discrete bilateral lesions in these two major regions derange mem ory and studying disproportionate to all different cognitive capabilities, and even a unilateral lesion of these buildings, especially of the dominant hemisphere, can produce a lesser diploma of the identical impact. The clinical-anatomic relationships that bear on this subject are mentioned intimately by Aggleton and Saunders and within the monograph on Wernicke-Korsakoff syndrome by Victor et al. A extreme but less-enduring defect in memory is noticed with harm of the anterior septal gray matter; a cluster of midline nuclei on the base of the frontal lobes, just below the interventricular septum and including the septal nucleus, nucleus accumbens, diagonal band of Broca; and paraventricular hypothalamic gray matter. The case of infarction of this region reported by Phillips and colleagues confirms the participation of this region in memory formation and retrieval. The amnesic syndrome, normally not everlasting, that follows a ruptured anterior communicating aneurysm is a consequence of disruption of those nuclei. These septal nuclei have connections with the hippocampus by way of the precommissural fornix and addresses the anatomic mechanisms of reminiscence func tion. It has been discovered that the hippocampal formations are persistently engaged during memory acquisition and retrieval tasks. These observations in combination verify that integ rity of the hippocampal formations and the medial-dorsal nuclei of the thalamus are essential for normal reminiscence and learning. Interestingly, there are only sparse direct anatomic connections between these two regions. Normal memory perform, as emphasized, entails many elements of the brain in addition to diencephalic-hippocampal buildings. The aforementioned basal frontal nuclei that project to the hip pocampi are an instance. Thus, a lesion of the dominant temporal lobe impairs the ability to keep in mind phrases (loss of express semantic memory), and a lesion of the inferior parietal lobule undermines the recognition of written or printed phrases in addition to the power to relearn them (alexia). The dominant parietal lobe is related to recollection of geo metric figures and numbers; the nondominant parietal lobe, to visuospatial relations; the inferoposterior tem poral lobes, to the popularity of faces; and the dominant posterofrontal region, to acquiring and remembering motor skills and their affective associations. Whether these are actually types of memory, or whether these areas of cortex must be entrained to have the ability to retrieve and "experience" the reminiscence, is philosophical. What stays inviolate is that the integrity of both the hippocampal-thalamic system and the suitable cortical area is required for memory as we check with it in this chapter, but only the previous is integrated into all modalities of studying and retrieval. Certain past recollections could be recalled, but imperfectly and with no regard for their regular temporal relationships, giving them a fictional high quality and explaining many instances of confabulation. Another noteworthy fact is that long-standing social habits, automatic motor skills, and memory for phrases (language) and visible impressions (visual or pictorial attributes of persons, objects, and places) are unimpaired. Long periods of repetition and utilization could have made these implicit or procedural recollections just about auto matic; they now not require the participation of the diencephalic-hippocampal constructions that were neces sary to learn them originally.
Lamotrigine 100mg saleSevere seizures may be accompanied by a systemic lactic acidosis with a fall in arterial pH, reduction in arterial oxygen saturation, and rise in these results are secondary to the respiratory arrest and excessive muscular activity. If extended, they could trigger hypoxic-ischemic injury to remote areas in the cerebrum, basal ganglia, and cerebellum. In paralyzed and artificially ventilated subjects receiving electrocon vulsive remedy, these adjustments are much less marked and the oxygen rigidity in cerebral venous blood may very well rise. According to Plum and colleagues, the rise in blood pressure evoked by a seizure normally causes a enough improve in cerebral blood move to meet the increased metabolic wants of the mind. Medial temporal sclero sis, heterotopias and other disorders of neuronal migration, glial scars, and porencephaly can be clearly visualized. There is an approximate relationship between the duration of seizure exercise and the depth and extent of these secondary modifications. Likewise, angiography or perfusion imaging performed soon after a seizure might show a focal area of enhanced blood move or elevated blood volume. All of these imag ing abnormalities are thought to replicate transient disrup tion of the blood-brain barrier, they usually rarely persist for more than a day or two. There are also imaging adjustments in the white matter, notably the splenium of the cor pus callosum that will happen soon after the withdrawal of certain antiepileptic medicines as discussed within the later section on using these medication and by Gurtler and colleagues). Like the imaging abnormalities these findings may lead to spurious conclusions in regards to the presence of an energetic intracranial lesion, notably if polymorphonuclear leukocytes predominate; a bigger pleocytosis should at all times be construed as a sign of inflammatory or infec tious disease. Of more practical value is the truth that virtually all generalized convulsions produce an increase in serum creatine kinase exercise that persists for hours, a finding that could be used to larger advantage in emergency departments to help in distinguishing seizures from fainting. Of course, in depth muscle harm from a fall or extended compression during a interval of unconscious ness can produce the identical abnormality. Concentrations of serum prolactin, like those of different hypothalamic hormones, rise for 10 to 20 min after all kinds of generalized seizures, including complicated partial types, but not in absence or myoclonic sorts. An elevation could assist differentiate a psychogenic seizure from a genuine one; nonetheless, serum prolactin may also be slightly elevated after a syncopal episode. Testing is facilitated by amassing capillary blood from the finger on filter paper for evaluation (Fisher et al). If elevations in these hormonal ranges are used as diagnostic tests, one should have details about normal baseline levels, diurnal variations, and the results of concurrent medica tions. Changes in physique temperature, that are mentioned to typically precede a seizure, could replicate hypothalamic modifications however are far much less consistent and tough to use in scientific work. Not surprisingly, there are also no seen lesions in the seizure states com plicating drug intoxication and withdrawal, transient hyper- and hyponatremia, and hyper- and hypoglycemia, which presumably represent derangements at the cellular stage. These embody zones of neuronal loss and gliosis (scars) or different lesions such as heterotopia, dysgenic cor tex, hamartoma, vascular malformation, porencephaly, and tumor. Certainly the focal epilepsies are associated with the highest incidence of structural abnorm:Uite, altho ugh in certain instances no morphologic change 1s VlSlble. W1th reference to the focal epilepsies, it has not been possible to determine which element of the lesion is answerable for the seizures. However, adolescence head trauma, infections, and quite lots of less-common perturbations may cause the ensemble of neuron loss and delicate gliosis of medial tem poral sclerosis. The cessation of seizures in lots of patients following surgical resection of the medial temporal lobe favors the primary interpretation that the pathologic change is major typically (see further on underneath "Surgical Treatment of Epilepsy"). Attesting to the uncertainty of cause or effect are numerous surgical collection that favor one view or the other (see editorial by Sutula and Pitkiinen). Role of Genetics Most major epilepsies have a genetic foundation and, as in many other ailments corresponding to diabetes and atherosclerosis, the mode of inheritance is advanced, i. That a genetic issue is operative within the primary generalized epilepsies is suggested by a familial inci dence in 5 to 10 p.c of such sufferers and, in certain households, the inheritance of a seizure dysfunction via specific genes (Gourfinkel-An et al). The significance of genetic elements within the primary epilepsies is also underneath scored by evidence from twin studies; in six main sequence, the overall concordance fee was 60 % for monozy gotic twins and thirteen p.c for dizygotic pairs. Of course, epilepsy is a part of many genetic syndromes which are defined by their dysmorphic seem ance or neurocutaneous disorder with or with out mental retardation.
Purchase 25mg lamotrigine otcRe-surgery could additionally be very troublesome including morbidity within the type of trauma to the organs, bleeding and infection. Incidence It is acknowledged that 95% girls develop adhesions following an infection, trauma and surgical procedures, although not all manifest the symptoms. Flimsy adhesions could stay asymptomatic and should never be found except repeat surgical procedure is performed for other indications. In obstetrics, the speed of caesarean part surgeries has gone up two- to threefold, and that alone has elevated the danger of stomach adhesions. Fitz-Hugh�Curtis syndrome forms a band between the best tube and the undersurface of the liver. Peritonitis causes belly as properly as peritoneal adhesions that lead to chronic abdominal pain or intestinal obstruction. Infection throughout intestinal surgery or lapses in aseptic technique, prolonged surgical procedure. It is an extract of the placenta containing enzymes that forestall or dissolve early adhesions. Surgical Adhesions n Laparoscopy is said to cause much less abdominal and pelvic adhesions. Of late, this is disputed, if surgical procedure is extended or trauma to the abdominal organs happens. Pathophysiology of Formation of Adhesion Adhesions are the connective tissues (fibrin) that bridge two organs or surfaces together. The plasma protein leaks and oozes causing fibrin deposition which begins as early as after 3 h of surgical procedure. Normally, the fibrin course of is reversed via enzymatic degradation by locally released fibrinolysin. Trauma and different factors similar to ischaemia and infection throughout surgery cut back the extent of fibrinolysis, thus initiating adhesion formation. Adhesion is fashioned as early as 5� 7 days after surgery, although they might not manifest for some time. Acute ache occurs with intestinal obstruction, when vomiting, incapability to pass flatus and abdominal distension happen. Chronic obstruction causes intermittent symptoms, with tubercular peritonitis causing cysts or persistent signs. There is less threat of adhesions if organs and tissues are handled gently and trauma to the visceral peritoneum prevented. Sutures over the visceral peritoneum (peritonization) and parietal peritoneum ought to be avoided-this is expected to reduce adhesions. Earlier, when postoperative adhesions were anticipated, omental or peritoneal graft was positioned over the suture line. Placentrex appears to assist in dissolving adhesions if given early within the administration. Since trauma and bleeding kind part of any surgery, formation of postoperative adhesion of no matter diploma and severity appears to be inevitable. Lately, some steps have been introduced to scale back postoperative adhesions in the form of insertion of adhesion-reducing agents. Locally, they get absorb-Assed too shortly into systemic circulation to be effective. Physical limitations have been subsequent introduced to maintain the 2 traumatic surfaces separate or to cowl the uncooked sutured space. Adept (4% icodextrin) resolution has a sufficiently lengthy peritoneal residence and provides hydroflotation during the crucial period of adhesion formation (5�7 days). It has been shown to scale back the incidence, extent and severity of postoperative adhesions. Interceed can nonetheless kind adhesions if not correctly applied and in the presence of incomplete haemostasis and an infection. Seprafilm (hyaluronic acid with carboxymethylcellulose) is a film placed over the suture line. It stays in the course of the interval of re-epithelization and will get spontaneously absorbed.
|