|
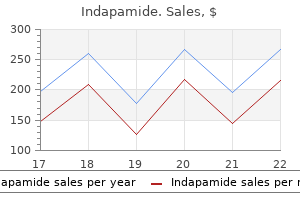
Indapamide dosages: 2.5 mg, 1.5 mg
Indapamide packs: 30 pills, 60 pills, 90 pills, 120 pills, 180 pills, 270 pills, 360 pills

Buy generic indapamide lineAs a outcome, an experienced B cell is ready to act as an antigen presenting cell for Th cells. However, later in the midst of the an infection or during subsequent infections, presentation of antigen by skilled B cells plays an important role. Because B cell receptors have such a high affinity for antigen, they act like "magnets," amassing antigen for presentation to Th cells. Then, while the battle is raging, activated macrophages on the entrance strains present antigen to warring T cells to hold them pumped up. Certainly one cause for sophistication I presentation is to focus the attention of killer T cells on contaminated cells, not on viruses and other pathogens which are outside our cells in the blood and tissues. So long as pathogens remain outside of our cells, antibodies can tag them for destruction by professional phagocytes, and can bind to them and prevent them from initiating an infection. Since each plasma B cell can pump out about 2000 antibody molecules per second, these antibodies are "cheap" weapons that deal quite effectively with extracellular invaders. When this occurs, killer T cells � the hightech, "costly" weapons, particularly designed to destroy infected cells � are needed. In addition, it would be extremely dangerous to have unpresented antigen signal T cell killing. Imagine how horrible it will be if uninfected cells happened to have particles from dead viruses stuck to their surfaces, and killer T cells recognized this unpresented antigen and killed these "harmless bystander" cells. Another purpose class I show is so essential is that most proteins made in a pathogeninfected cell remain inside the cell, and by no means make their approach to the cell surface. So without class I display, many pathogeninfected cells would go undetected by killer T cells. After all, there are so much of different varieties within the human inhabitants that most of us inherit genes for six totally different class I molecules. Such a virus might wipe out the entire human population, as a end result of no killer T cells could possibly be activated to destroy virusinfected cells. Antigen presenting cells only current antigen efficiently when a battle is occurring, and helper T cells are educated not to react against our personal proteins. Consequently, both the helper T cell and the antigen presenting cell should "agree" that there was an invasion before a helper T cell may be activated. As a end result, the number of targets that a helper T cell can "see" throughout presentation far exceeds these out there for viewing in a large, folded protein. The consequence of this expanded number of targets is a stronger, extra numerous immune response during which many various helper T cells might be activated � helper T cells whose receptors recognize the many completely different epitopes that make up the antigens of an invader. Consequently, I will "persist with the rule" that T cells solely acknowledge protein antigens. Transplantation studies really started within the Nineteen Thirties with experiments involving mouse tumors. In these days, tumors were normally induced by rubbing some horrible chemical on the pores and skin of a mouse, and then waiting for a really lengthy time for a tumor to develop. Because it was a lot hassle to make these tumors, biologists wished to keep the tumor cells alive for examine after the mouse had died. What they observed, however, was that the tumor cells solely could be efficiently transplanted when the 2 mice had been from a strain of mice in which there had been a lot of inbreeding. And the more inbred the strain, the better the chance for survival of the transplant. This offered the impetus for the creation of a quantity of inbred mouse strains that immunologists depend on right now. Once inbred mouse strains have been available, immunologists began to study the transplantation of regular tissues from one mouse to another. Right away they noticed that if a small patch of skin from one mouse was grafted onto the skin of one other mouse, this new pores and skin retained its wholesome pink colour and continued to develop � as lengthy as the two mice had been from the same inbred strain. To identify the genes that are concerned in "tissue compatibility" (histocompatibility), immunologists bred mice to create strains that differed by just a few genes, yet which were nonetheless incompatible for tissue transplants. Some of their favorite targets are the cells that make up the blood vessels contained inside the donated organ. There they meet up with proteins which have been taken into the cell by phagocytosis and minimize up into peptides by enzymes. In addition, because protein folding can hide giant parts of a protein from view, chopping a protein up into small peptides reveals many potential T cell targets that would be inaccessible in an intact protein.
Syndromes - Short height
- Items such as jewelry, watches, credit cards, and hearing aids can be damaged.
- Painful sensations in the arms and legs
- Passing large amounts of urine, which can lead to dehydration
- Infection (a slight risk any time the skin is broken)
- Mifepristone
- General paresis
- Increased risk of infections
- Sleeping difficulty
2.5mg indapamide with mastercardOccasionally, hemangiomas become clinically evident through the first decade of life. Hemangiomas regularly happen within the craniofacial bones, predominantly within the calvarium, and in some collection almost 50% of the lesions occur at this site. On the other hand, if post-mortem information on asymptomatic lesions are included, the vertebral our bodies represent the most frequent website of involvement by hemangioma. The major long tubular bones are the bones of the appendicular skeleton most incessantly involved. The small multifocal lesions are most frequently recognized in the vertebral column involving adjoining vertebral bodies. Radiographic Imaging Radiographically, hemangiomas present as lucent, welldemarcated defects. Peak age incidence and most frequent websites of skeletal involvement are indicated by solid black arrows. A, Hemangioma of frontal bone with distinguished striations of bone trabeculae traversing lesion. A, Expansile lesion of vertebral finish of rib has honeycomb appearance and spiculated reactive bone of periosteal origin. B, Specimen radiograph exhibits radiating spicules of periosteal new bone and coarse trabeculation. C, Gross photograph of resected rib shows radiating spicules of periosteal new bone and outstanding trabeculation. D, Lateral plain radiograph of face shows honeycomb look of nasal bone produced by cavernous hemangioma. E, Low energy photomicrograph of nasal bone hemangioma shown in D composed of cavernous vascular channels. A and B, Anteroposterior and lateral radiographs of knee of young lady who sustained pathologic fracture via large, beforehand asymptomatic honeycomb lesion occupying proximal half of tibia. Radiating spicules of periosteal reactive bone are outstanding, particularly on lateral facet, and counsel preoperative diagnosis of major malignant bone tumor. They can mimic benign osteoblastic lesions (osteoid osteoma, osteoblastoma) radiographically. Magnetic resonance imaging of hemangiomas usually reveals a low signal on T1-weighted pictures and a excessive signal on T2-weighted pictures. In vertebral physique hemangiomas, the loss of hematopoietic cells in the interstices of hemangiomas and apparent enhance in fats can produce a high sign in T1-weighted images. Gross Findings Hemangioma presents as a brown-red or dark red, welldemarcated, medullary lesion. A, Anteroposterior radiograph reveals expansible trabeculated lucent lesion of distal tibial shaft. B, Photomicrograph of biopsy material of same lesion exhibits engorged capillary-sized vessels (�50; hematoxylin-eosin). Microscopic Findings Hemangiomas are composed of a conglomerate of thinwalled blood vessels. A majority of bone hemangiomas are of cavernous or blended types (cavernous and capillary). The intercellular tissue consists of unfastened connective tissue that will exhibit myxoid change. In such instances, the lesion consists of vessels and stromal tissue, but more usually, some residual trabeculae of cancellous bone are present. Some hemangiomas may trigger pronounced sclerosis of the intralesional and adjoining bone. In vertebral physique hemangiomas, the blood-forming parts may be misplaced utterly in the interstices, resulting in an unmasking of adipose tissue. This obvious increase in fats in the interstitial tissue of vertebral hemangiomas can be fairly outstanding. Hemangiomas have a attribute microscopic appearance and within the majority of circumstances are simple to recognize. However, secondary adjustments might alter this traditional pattern and make the prognosis troublesome. Hemangiomas of any sort, but especially those with massive cavernous vessels, sometimes develop thromboses with calcifications.
Proven indapamide 2.5 mgIn some cases, a mass was famous up to 20 years earlier than the onset of generalized signs. Occasionally an asymptomatic bone tumor is recognized in radiographs in a affected person with a analysis of vitamin-D resistant rickets. The urinary phosphate degree is normally elevated, and most instances exhibit decreased tubular reabsorption of phosphate (23% to 70%). Serum levels of 1,25-dihydroxyvitamin D3 are low or detectable, whereas serum levels of 25-hydroxyvitamin D3 are generally normal. In addition, aminoaciduria and glycosuria with regular serum glucose ranges may be current. In addition, skeletal radiographs might reveal the presence of an asymptomatic or symptomatic tumor. Pathologic Findings Histomorphometry on undecalcified bone sections exhibits hyperosteoidosis with increased osteoid quantity and elevated width of osteoid seams. The specific lesions of this group are nonossifying fibromas and giant cell reparative granuloma, giant cell tumor, and pigmented villonodular synovitis. The majority of tumors are comparatively small-within the vary of 1 to 4 cm-but occasionally measure 7 cm or bigger. It was recognized by several authors that many of these tumors show a distinctive morphology and have microscopic features in widespread. These authors identified that wider recognition of the histologic features of phosphaturic mesenchymal tumors might sometimes establish sufferers with previously undiagnosed osteomalacia. A, Radiograph of knee of identical case in A showing radiolucent zones on metaphyseal sides of development plates and circumscribed eccentric lesion of distal femur recognized as hemangiopericytoma. B, Radiograph of wrist with radiolucent zones on metaphyseal sides of the growth plates and flaring of the metaphyses characteristic of rachitic adjustments. Pathogenesis A extensive variety of causes could give rise to osteomalacia or rickets, and their description is past the scope of this book. In developed countries, nevertheless, on condition that inadequate nutrition is rare, a few of the uncommon causes are X-linked hypophosphatemia and autosomal dominant hypophosphatemia. After the tumor is excised, a dramatic reversion to normal bone metabolism implies that the tumor is directly liable for skeletal changes. Immunoassays performed on saline tumor extracts present no evidence of parathyroid hormone or calcitonin. Phosphaturia would be a direct effect of 1,25-dihydroxyvitamin D3 deficiency, as a result of it has been proved that the latter will increase renal phosphate resorption. They additionally play a job in autosomal dominant hypophosphatemic rickets, which has medical manifestations nearly equivalent to those of X-linked hypophosphatemic rickets and tumor-induced osteomalacia. Recurrence of the original tumor (benign or malignant) ends in the reappearance of the chemical findings with or with out accompanying clinical symptoms or skeletal adjustments. In truth, chemical monitoring can be used for identification of local recurrence or metastasis. Correction of the laboratory abnormalities often occurs from 1 day to 20 months after surgical procedure. B, Photomicrograph of tumor composed of oval and spindle cells with branching stag-horn pattern of vascular spaces. C, Different space of tumor proven in B with tightly packed parieytic cells and prominent cystic vascular spaces. A and B, Radiograph of the knee exhibiting radiolucent zones on the metaphyseal sides of progress plates. Note an inconspicuous eccentric lesion with sclerotic margins involving the femoral metastasis identified as nonossifying fibroma (arrows). C-E, Photomicrographs of nonossifying fibroma displaying proliferation of spindle cells organized in storiform sample with interstitial hemorrhage and scattered osteoclast-like multinucleated large cells. A, Radiograph of tibia displaying radiolucent intracortical lesion involving the proximal metaphysis. Note radiolucent zones on metaphyseal sides of progress plates characteristic of rickets. B, Magnetic resonance image of same case as A showing eccentric intracortical lesions of low signal intensity. C, Gross photograph of case shown in A and B, exhibiting expansile intracortical lesion with closely mineralized matrix. D, Low energy photomicrograph showing intracortical lesion with outstanding production of tumor osteoid.
Order on line indapamideGoodfellow P, Banting G, Sheer D, et al: Genetic evidence that a Y-linked gene in man is homologous to a gene on the X chromosome. Kiyonari S, Kadomatsu K: Neuroblastoma models for insights into tumorigenesis and new therapies. Li Q, Cui W, Abulajiang G, et al: Application of immunohistochemistry within the diagnosis of small round blue-cell tumors of soft tissue. Martin-Zanca D, Oskam R, Mitra G, et al: Molecular and biochemical characterization of the trk proto-oncogene. Ushigome S, Shimoda T, Nikaido T, et al: Primitive neuroectodermal tumors of bone and soft tissue. Gamberi G, Cocchi S, Benini S, et al: Molecular prognosis in Ewing household tumors: the Rizzoli experience-222 consecutive circumstances in 4 years. Bertoni F, Picci P, Bacchini P, et al: Mesenchymal chondrosarcoma of bone and gentle tissue. In such situations, a bone pathologist or maybe a general pathologist, somewhat than a hematopathologist, is extra likely to be confronted with diagnostic challenges. For these causes, familiarity with skeletal manifestations of hematopoietic lesions ought to be of basic interest. This chapter also discusses plasma cell myeloma and different plasma cell neoplasms, non-Hodgkin lymphomas, leukemias, histiocytic and dentritic cell proliferations, and mastocytosis, with specific reference to their involvement of skeletal tissue. The earliest hematopoietic stem cells are able to producing cells of all blood lineages. Both fashions begin with a long-lived uncommitted hematopoietic stem cell that then differentiates into a shortlived multipotent hematopoietic stem cell. The first mannequin, the classical myeloid-lymphoid model, postulates that the first step occurs with lineage dedication to myeloid or lymphoid differentiation. The widespread myeloid precursor then provides rise to two lines of differentiation, a megakaryocyte/erythroid line, and a granulocyte/monocyte lineage. The myeloid-based model of lineage differentiation can be supported by examples of neoplasms exhibiting lineage plasticity similar to acute leukemias of ambiguous lineage with both myeloid and lymphoid options. Normal Langerhans cells arise from fetal macrophages that differentiate after migrating to the skin. Neoplastic Langerhans cells, nevertheless, are thought to arise from a myeloid precursor. Currently, probably the most broadly accepted classification is the World Health Organization Classification of Hematopoietic and Lymphoid Tissues, first published in 2001 and revised in 2008. As targeted remedy turns into increasingly more prevalent, the molecular alteration of pathways that drive the proliferation and survival of those hematopoietic neoplasms is turning into essential within the description of these entities. Uncommited hematopoietic stem cells give rise to cells with progressive dedication to improvement of assorted cell lineages. Hematopoietic neoplasms come up from cells of particular dedicated lineages or their precursors. Clinical Features Plasma cell myeloma is amongst the most regularly occurring hematopoietic neoplasms and accounts for about 1% of all malignant neoplasms in white sufferers and roughly 2% in black sufferers. It is the second commonest hematopoietic malignancy, accounting for approximately 10% of hematopoietic neoplasms, and essentially the most frequent neoplasm presenting as skeletal lesions. Peak age incidence and most regularly involved skeletal websites are indicated by solid black arrows. Plasma cell myeloma often presents with multifocal osteolytic lesions, proliferation of plasma cells, and monoclonal gammopathy. In the overwhelming majority of sufferers, increased levels of monoclonal immunoglobulins (M-protein) may be detected by serum or urine electrophoresis. Two broad classes of plasma cell myeloma are designated smoldering (asymptomatic) myeloma and symptomatic myeloma. Br J Haematol 121:749-757, 2003 and Kilciksiz S, et al: A evaluate for solitary plasmacytoma of bone and extramedullary plasmacytoma. Adapted from Dimopoulos M, et al: Consensus suggestions for normal investigative workup: report of the International Myeloma Workshop Consensus Panel 3. Blood 117:4701-4705, 2011 and Kilciksiz S, et al: A evaluation for solitary plasmacytoma of bone and extramedullary plasmacytoma. In the present era of novel therapeutic agents, overall median survival is now approximately eight years.
Order 2.5mg indapamide visaD, Higher magnification of C exhibiting pronounced atypia and focal clearing of the cytoplasm in sarcomatoid cells. Grade 2 corresponds to an intermediate tumor with elevated stromal cellularity, excessive mitotic exercise, and greater than traditional native aggressiveness. However, it is rather difficult to predict the conduct of grade 1 and a pair of lesions in phrases of their local development potential and tendency for recurrence. For this cause, Jaffe himself, along with many others, discontinued the numeric grading of giant cell tumors. The abandoned grading system and the overall method to big cell tumors have alerted clinicians and pathologists to a spectrum of biologic behaviors in these lesions. These can be separated into a number of distinct clinicopathologic entities on the premise of their unique presentation, associated disorders, and genetic background. Giant cell reparative granulomas which are associated with primary or secondary hyperparathyroidism are actually reactive conditions and are referred to because the brown tumor of hyperparathyroidism. Definition Giant cell reparative granulomas are unusual benign lesions with a predilection for the craniofacial bones. In 1962, Ackerman and Spjut120 described the primary two circumstances involving the small tubular bones of the arms and designated the lesions as large cell reactions. In 1980 the term large cell reparative granuloma was proposed by Lorenzo and Dorfman176 in reference to reactive lesions with a giant cell�containing fibrous look within the quick tubular bones of hands and toes. Subsequently, microscopically related lesions of vertebrae and ethmoid bones were described by Sanerkin et al. All such lesions are microscopically related and were perceived as representing an analogous course of that merely presents in several skeletal websites. In reality, giant cell reparative granulomas had been thought-about as an initial stage in the spectrum of intraosseous responses that, in some cases, can culminate as rapidly expanding harmful multicystic lesions. It seems that patients with large cell reparative granuloma of the lengthy tubular bones and the vertebrae are considerably older; the height age incidence in these anatomic websites is within the third decade of life. The contour of bone can be expanded with markedly thinned however often intact cortex and no periosteal reaction. In skeletally mature patients, the lesion can contain the epiphysis and even the entire bone. In the small tubular bones, the lesion is centrally situated with markedly expanded contour of the bone and a thinned but intact cortex. Microscopic Findings Giant cell reparative granuloma is composed of fibrous stromal tissue with spindle-shaped fibroblasts and varying quantities of collagen. The giant cells and their clustering are significantly evident in areas of hemorrhage. Usually, there are few mononuclear inflammatory cells and trabeculae of newly shaped reactive bone rimmed by osteoblasts. Microscopic evidence of hemorrhagic cyst formation resembling an aneurysmal bone cyst is incessantly current. On the opposite hand, some giant cell reparative granulomas may be hypercellular, exhibiting florid proliferation of plump fibrohistiocytic cells. Special Techniques Ultrastructurally, multinucleated giant cells of big cell reparative granuloma are similar to these current in large cell tumor and specific features of osteoclasts. B, Typical appearance of big cell reparative granuloma of fifth metacarpal bone in a skeletally mature 15-year-old boy with involvement of epiphysis. E, A seventeen-year-old boy with pathologic fracture by way of expanded lytic diaphyseal lesion involving shaft of first metatarsal bone. F, Extensive lytic lesion involving almost complete first metatarsal bone in a skeletally mature 17-year-old lady. A, Lytic metaphyseal lesion of proximal fibula in a skeletally immature 15-year-old boy. B, T1-weighted coronal magnetic resonance picture of lesion in A reveals high signal in tumor. C, Sharply demarcated lytic lesion of distal fibular shaft in a skeletally mature 16-year-old lady. B and C, T2-weighted coronal magnetic resonance imageshows excessive sign in lesion involving body of C2. Cytogenetic testing carried out on a couple of cases of large cell reparative granuloma present some clonal rearrangement involving different chromosomes, including t(1;17;18) and t(X;4)(q22; q31.
RGAE (Rehmannia). Indapamide. - What is Rehmannia?
- Are there safety concerns?
- Are there any interactions with medications?
- Diabetes, anemia, fever, osteoporosis, allergies, or other conditions.
- Dosing considerations for Rehmannia.
- How does Rehmannia work?
Source: http://www.rxlist.com/script/main/art.asp?articlekey=97099
Purchase 2.5mg indapamide with mastercardThe involvement of the central nervous system both cranial and spinal is typical for this tumor. Approximately 30% of mesenchymal chondrosarcomas present as extraskeletal gentle tissue lesions. Rare examples of mesenchymal chondrosarcoma arising in visceral organs had been also described. Clinical Symptoms Pain and swelling of the affected space are the first initial symptoms. Radiographic Imaging Mesenchymal chondrosarcoma seems radiographically as a radiolucent lesion with various levels of matrix calcification. Heavy calcified eccentric tumor at junction of rib and vertebral transverse process is present. C, Soft tissue mass with distinguished punctate calcifications adjacent to proximal femoral shaft in a 48-year-old woman. Stippled calcifications disclosing the cartilaginous nature of the lesion are additionally frequently present within the gentle tissue lesions. Surprisingly, this extremely aggressive tumor may occasionally have a sharply demarcated sclerotic margin. The stage of mineralization can vary, and sometimes massive areas of heavily calcified tissue can be present. Larger areas of cartilaginous differentiation can generally be grossly identified. The primitive mesenchymal element regularly displays hemangiopericytomalike options with a number of endothelial-lined vascular spaces. The proportion of cartilaginous and primitive components can vary among the tumors and in numerous areas of the identical lesion. Pleuropulmonary blastoma, or the so-called pulmonary blastoma of childhood, is a tumor that happens within the gentle tissue of the chest wall and lungs in young kids. The prognosis for these sufferers is grave because more than 50% die inside 2 years after analysis. At least some of these tumors have microscopic features much like these of mesenchymal chondrosarcoma. Lipoblastic differentiation, if present, is associated with positivity for S-100 protein. Special Techniques Ultrastructurally, mesenchymal chondrosarcoma consists of oval or plump elongated primitive mesenchymal cells. The cells in these foci are surrounded by a granular low-density matrix consistent with chondroid. The immunohistochemical staining sample is nonspecific and implicates cartilage lineage differentiation. The small cells of mesenchymal chondrosarcoma regularly show divergent differentiation. Scattered positivity of isolated small cells for desmin is a relatively widespread finding. A, Lateral radiograph displaying a damaging tumor with anterior extension involving the distal femoral metaphysis. A, Anteroposterior radiograph showing a calcified destructive tumor mass involving proximal humerus. Note circumferential cortical destruction and extension to soft tissue with radiating mineralized spicules. Such a mineralization sample may be radiographically misinterpreted as an osteosarcoma. B, Fatsaturated T2-weighted axial magnetic resonance picture exhibiting excessive sign intensity tumor with circumferential extension to paraosseous soft tissue. C and D, Gross photographs of the bisected resection specimen in A and B exhibiting fleshy tumor mass involving medullary cavity of proximal humerus with circumferential soft tissue extension. A and B, Oblique and anteroposterior radiographs exhibiting a calcified tumor involving the scapula. C, Resected specimen shows a tan lobulated tumor extending anteriorly and posteriorly to the periscapular gentle tissue. A, Anteroposterior radiograph exhibits a calcified mass in the right paraspinal region. B, Axial computed tomogram demonstrates a calcified mass in the delicate tissue of the best paraspinal area.
Order indapamide 1.5mg with mastercardIncidence and Location Osteofibrous dysplasia is a uncommon lesion, accounting for lower than 1% of all bone tumors. Although it typically happens during the first 20 years of life, some cases have been current at delivery. Additional synchronous, predominantly lytic foci could additionally be current near the distal or proximal finish or, much less commonly within the fibula. The anterior bowing deformity is usually current on the time of prognosis and may turn out to be more pronounced with progression of the disease. In this age group, the origin of the lesion within the anterolateral cortex is probably not obvious on radiographs. Graphic presentation of idea of differentiated adamantinoma of long bones and its relationship to osteofibrous dysplasia�like adjustments. The central portion of the lesion is predominantly fibrous and may exhibit myxomatous or cystic adjustments. Pathologic fracture, hemorrhage, and focal collections of multinucleated big cells can alter this classic pattern. Single, scattered, keratin-positive cells that are verified ultrastructurally as epithelial components are regularly present and help the concept that osteofibrous dysplasia could symbolize an indolent form of adamantinoma. This is to not deny the existence of circumstances by which a scrupulous search is adverse for any epithelial element. The identification of clonal chromosomal abnormalities in osteofibrous dysplasia helps the idea that an underlying indolent neoplastic course of could additionally be involved within the pathogenesis of osteofibrous dysplasia. He postulated that this was an aggressive lesion with an inclination for native recurrence and development. Campanacci and Laus79 designated the identical lesion as osteofibrous dysplasia and noticed that it initially grows in a regionally aggressive means however that the method tends to stabilize at puberty. During the second decade of life, no less than a few of these lesions become stationary and develop gradual sclerosis, but the deformities could persist. This observation necessitated a more conservative method to the treatment of osteofibrous dysplasia, which should be restricted to corrective procedures rather than radical excisions. Differential Diagnosis Clinically, radiographically, and microscopically, osteofibrous dysplasia must be differentiated from typical fibrous dysplasia and from each types of adamantinoma: basic and differentiated. The differential prognosis between osteofibrous dysplasia and adamantinoma of lengthy bones is discussed within the part on osteofibrous dysplasia�like adamantinoma on this chapter. Our delineation of two subsets of adamantinoma, particularly the basic and differentiated (osteofibrous dysplasia�like) varieties, suggests that the latter lesion, regardless of focal presence of epithelial components, pursues a medical course similar to that of conventional osteofibrous dysplasia. Occasionally the lesion might encompass a single larger focus of fibrous tissue surrounded by an expanded shell of sclerotic cortex. Microscopic Findings the lesion is composed of free bundles of fibroblast-like cells that usually present a storiform pattern. In appropriately sampled cases, zonal structure can be observed with progressive widening, maturation, and increased numbers of mineralized bone trabeculae at the periphery of the lesion. A, Multifocal lytic adjustments of tibia identified as osteofibrous dysplasia when affected person was eight years old. Note gradual progression of lesion, with sclerosis and gentle anterior bowing of tibia. Note nearly no development in contrast with B transforming of tibial cortex and partial correction of bowing. At this time, biopsy with immunohistochemical research revealed scattered epithelial elements, and lesion was reclassified as differentiated adamantinoma. Peak age incidence and typical sites of skeletal involvement are indicated by a strong black arrow. A, Lateral radiograph of tibia of an 8-year-old boy with anterior bowing deformity related to intracortical lesion of tibia. A, Lateral view of tibia of young affected person with anterior bowing deformity and fusiform cortical enlargement of anterior cortex.
Buy indapamide with visaOverdistension of the accumulating system ought to be prevented to minimize the risk of sepsis. Overdistension can lead to pyelovenous backflow of urine, carrying along any pathogens contained in the urine. With this method, an equal quantity of pure distinction materials is injected after the withdrawal of a quantity of urine and diluted distinction materials via the needle. With this process, opacification of the urinary system is slower, however overdistension is avoided because the quantity of distinction material injected matches the amount of urine withdrawn. For antegrade pyelography, spot movies are obtained as wanted to reveal the whole pelvicalyceal system and ureter, with particular attention to the sites of suspected abnormality. Antegrade pyelography is being carried out before percutaneous nephrostomy drainage. A skinny needle has been handed (arrowhead) in a vertical path in the region of the renal pelvis with the patient within the inclined position. B, Diagram of skinny-needle puncture of the best kidney in a patient within the susceptible place. A, Prone radiograph of the the Whitaker test is carried out after opacification of the accumulating system for antegrade pyelography. Opacification is performed to ensure that the needle is within the appropriate place, with out extravasation outdoors the urinary tract. With the needle in place, the bladder is emptied, and manometers, infusion strains, a power infusion pump, and a bladder drainage conduit are linked. Bladder and renal pelvic pressures are measured just before and instantly after every timed infusion. For the Whitaker test, dilute contrast materials is infused into the renal pelvis at a rate of 5 mL/minute for 10 minutes. The second infusion is carried out at 10 mL/minute for 10 minutes; and finally a 3rd infusion is performed at 15 mL/minute for 10 minutes. Infusions must be discontinued immediately if adjusted renal pelvis strain exceeds forty cm H2O, of if severe flank pain develops, or vital contrast extravasation occurs. If results are equivocal from this preliminary collection of infusions, the test is repeated, however with the bladder stuffed. Occasionally, mild obstruction could turn out to be evident with increased pressure solely with a full bladder. The affected person ought to be instructed to notify personnel in the course of the procedure if symptoms are reproduced throughout infusion of distinction material. The copy of symptoms, corresponding to flank ache, supports the presence of urodynamically vital obstruction. Net renal pelvic pressures are calculated by subtracting the bladder pressure from the renal pelvic stress, thereby eradicating the part of general intraabdominal pressure from the measurements. Table 10-1 outlines a system for classifying the numerical outcomes of the Whitaker exams and converting them to diploma of ureteral obstruction. The commonest indications are decompression of an obstructed kidney, urinary diversion for therapy of urinary tract fistula or perforation, decompression of an contaminated urinary tract, or as a prelude to extra urinary tract interventions, such as stent placement or endoscopy. The only absolute contraindication is the presence of an uncorrected bleeding dysfunction. With this procedure as with other percutaneous transrenal procedures, antibiotics should be preadministered. Selection of the transrenal puncture website is essential to keep away from pointless vascular injury. Ideally, the nephrostomy tract ought to traverse the kidney close to the junction of the ventral two thirds and the dorsal one third of the kidney. This plane has been used for renal surgical procedures to minimize postoperative renal atrophy. In most situations the best approach for guiding transrenal puncture is fluoroscopy with opacification of the accumulating system. It is most desirable to carry out transrenal puncture of the kidney via this region of the renal parenchyma. This area represents a watershed zone between the distributions of the anterior and posterior divisions of the renal artery.
Cheap 1.5 mg indapamide visaT1-weighted photographs typically present a punctate sign void within the lesion involving the joint capsule. However, T2-weighted images present signal enhancement and will present the lesion to have a multinodular structure. At the opposite finish of the spectrum are longlasting lesions that present as a consolidated, closely calcified mass. Note enlargement of acetabular fossa and calcified intrasynovial cartilaginous our bodies attribute of localized synovial chondrometaplasia. A and B, Computed tomogram of skull reveals involvement of temporomandibular joint by synovial chondromatosis. Note enlargement of joint and areas of sign void inside joint and in thickened synovium. A, Plain radiograph of wrist and hand reveals gentle tissue calcifications in wrist joint overlying triquetrum, hamate, and distal end of ulna (arrows). B, Lateral view of wrist (same case as A) shows gentle tissue calcified bodies that are each dorsal and volar in location (arrows). A, Anteroposterior radiograph of foot shows soft tissue calcification between first and second metatarsals with ringlike and punctate appearance. B, Oblique radiograph reveals gentle tissue calcifications representing unfastened cartilaginous bodies in tendon sheath. A and B, Synovectomy specimen in case of diffuse synovial chondromatosis of knee joint. C and D, Loose cartilaginous our bodies and synovial membrane from two instances of synovial chondromatosis that diffusely concerned knee joint. A, Localized synovial chondromatosis presents as conglomerate of particular person cartilage nodules. B, Pedunculated polypoid lesion of knee joint is composed of individual cartilage nodules and interlacing synovial membrane. C, Radiograph of shoulder displaying a conglomerate of particular person mineralized nodules with punctate and ringlike calcification patterns. D, Central calcification in metaplastic chondroid nodule of synovium in knee joint. A, Low energy photomicrograph of cross section by way of synovium of knee joint in synovial chondromatosis. B, Medium power photomicrograph of typical chondroid metaplastic nodules in synovium of knee joint. C, Low power photomicrograph of synovium with conversion of cartilage nodules to bone. A, Ill outlined nodules composed of chondroblastic cells in the synovial membrane representing early phases of synovial chondromatosis. B, Higher magnification of A displaying a sick defined subsynovial nodule composed of chondroblastic cells with early evidence of matrix deposition within the heart. A, Low energy view displaying hypercellular ill defined nodules composed of chondroblastic cells. B, Higher magnification of A exhibiting an ill outlined nodule composed of chondroblastic cells. A, Medium power photomicrograph of chondroid metaplastic nodules in synovium with clear cell options. B, Higher magnification of A exhibiting cartilage nodules in the synovial membrane with clear cell features and nuclear hyperchromasia. C, Higher magnification of metaplastic synovial cartilage nodules with clear cell features and nuclear hyperchromasia. A, Low power photomicrograph of synovium containing nodules of metaplastic cartilage with hyaline and myxoid features. B, Medium energy photomicrograph reveals hyaline cartilage arising via metaplasia of synovial membrane. Inset on left reveals early stage of improvement with myxoid differentiation of connective tissue cells and intercellular matrix. A and B, Low energy photomicrographs displaying in depth cartilage metaplasia of the synovial membrane with confluent cartilage nodules. C and D, Intermediate and excessive energy photomicrographs showing myxoid and hyaline chondroid matrix formation.
Proven 1.5 mg indapamideThe nuclear chromatin is finely granular, and there are usually one to three clearly identifiable small- to intermediate-sized nucleoli. The cytoplasm is vague and types an ill-defined slender rim across the nucleus. Often a biphasic pattern is simulated by the presence of so-called darkish cells and light cells. These kinds of cells are sometimes referred to as principal (light) and secondary (dark) cells, respectively. The ratio between these two forms of cells varies from tumor to tumor and in numerous areas of the same lesion. In some tumors, cords or clusters of dark apoptotic cells kind an interconnecting network of irregular patches that create a pseudoorganoid pattern. Complete permeation of the cortex and its eventual disruption are associated with the formation of a mass that originally types subperiosteally after which extends into gentle tissue (parosteal). Penetration of the cortex and disturbance of the periosteum are related to new bone formation. The proportion of stromal reticular components and blood vessels is elevated near the advancing fringe of the tumor in contrast with its more central intramedullary portion. Multilayered periosteal new bone formation, similar to an identifiable onion-skin look on radiographs, can accompany the advancing tumor cells. Periosteal bone formation is related to plump reactive osteoblasts and multinucleated osteoclast-like big cells and should have foci of cartilage metaplasia. Peripheral areas of the tumor within delicate tissue may show extra dispersed tumor cells invading collagenized stroma, adipose tissue, and skeletal muscle. Occasionally, a distinct growth pattern in the type of bigger lobules or nests composed of compact tumor cells and separated by fibrous septa may be seen. Vascular formation within the central portion is inconspicuous and is represented by slitlike capillaries with fantastic endothelial cells amongst tumor cells. Larger, thick-walled vessels can be seen within stromal bands separating tumor cells. The morphologic options of cells, and particularly the main points of the nuclei, are often Text continued on p. A Computed tomogram reveals intramedullary tumor with cortical disruption posteriorly and extension into gentle tissue. B and C, Anteroposterior and lateral plain radiographs present permeative lesion in metaphyseal region; so-called cortical saucerization (concave defect) can be seen on posterior floor in C. A, Large destructive tumor of body and glenoid areas of scapula with associated delicate tissue mass. This atypical plain radiographic appearance was interpreted initially as probable vascular tumor. C, Expansile tumor with moth-eaten pattern of bone destruction in distal end of fibula in young adult. B, Radiograph of amputation specimen reveals destruction of proximal plate of nice toe and ill-defined delicate tissue mass. C, Permeative damaging lesion involving whole shaft of proximal phalanx of finger is proven in this indirect radiograph. A, Lateral radiograph of ankle and foot of young grownup exhibits rarefaction of posterior a part of os calcis. B, Anteroposterior radiograph shows permeative destruction of cancellous bone with ill-defined border. C, Technetium 99 bone scan shows excessive uptake of isotope in os calcis, which is extra intense posteriorly. Although distal tibia showed elevated isotope uptake, tumor was not current on this website. A and B, Plain radiographs present harmful lytic mass of proximal tibia with enhance of latest periosteal bone formation. A and B, Coronal and sagittal computed tomograms displaying a big tumor involving the higher portions of the left thoracic wall and pulmonary cavity. C and D, Axial and sagittal magnetic resonance pictures showing a large low signal intensity tumor involving the left paraspinal area and thoracic wall. Proximal circumferential gentle tissue extension with elevation of periosteum is evident.
|